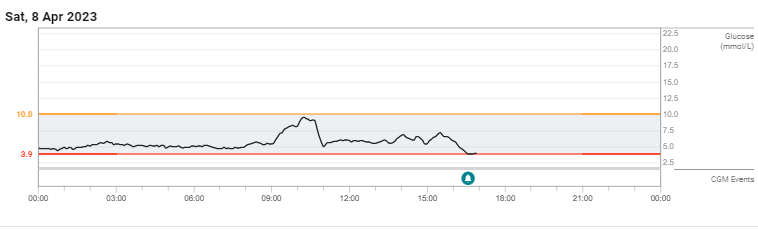
Here are a few more days:
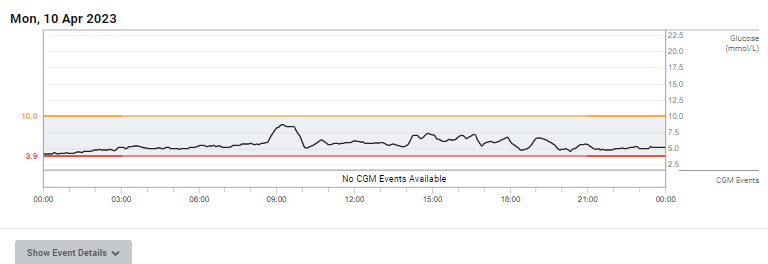
The only thing that is really consistent amongst these is that I go for breakfast in a particular pub and the breakfast is the same (apart from Day 2 Rapamycin 4mg which was 100g of sucrose in water).
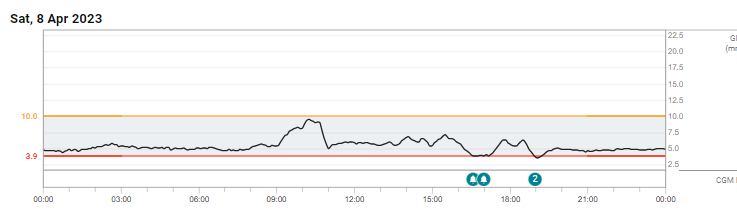
From a breakfast point of view yesterday and today were both quite interesting as I had breakfast (at different times) and then immediately left the pub. Yesterday I was doing the live streaming for a memorial service so I needed to get in early to test all the equipment. Today actually I wanted to go home really quickly so that any effect of exercise would be soon after eating.
I then don’t tend to eat until about noon 1pm.
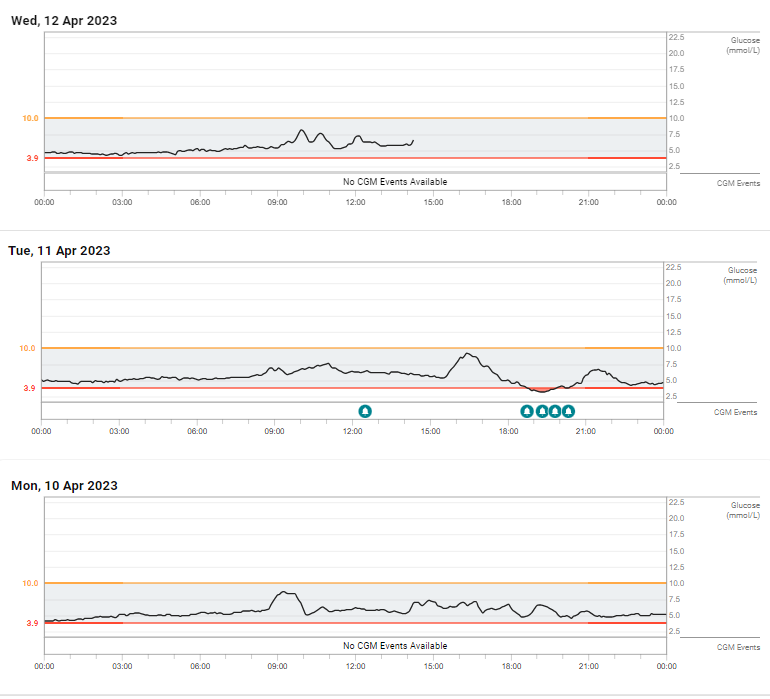
So today I was home at 9.32 having been shopping and have finished breakfast at 9.09, but started walking at 9.15. There is, I think, a slight delay as the blood glucose levels get reflected in the interstitial fluid hence I think you can see a false summit of glucose at 9.24, that then dips until 9.34, and then there is a first peak at 9.59 then a second peak at 10.39.
My serum rapamycin levels will be quite low by now.
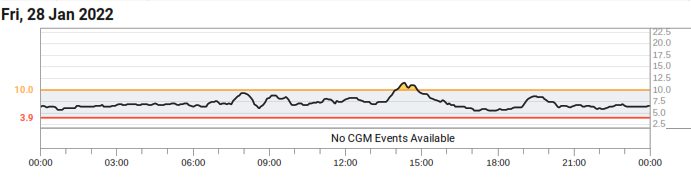
Looking (as I can in Dexcom’s cloud service) at the detailed figures I think when I had peak Rapamycin my blood glucose would be perhaps 0.5 mmol/L (approx) higher than it would be at trough or zero Rapamycin. I intend to download the data in a digital form and calculate some averages.
It is hard with this as obviously we have a number of varying factors, Food and Rapamycin are quite easy to control. Alcohol is controllable up to a point. Cortisol is harder to control although exercise can be planned. Insulin will follow on in interesting ways.
I am not quite sure how Melatonin affects blood sugar (I know it generally reduces it), I think that may be through a reduction in Cortisol.
As a second point I think there is also an issue where the way in which Glucose and Alcohol interact is changed by Rapamycin. However, I think there is a need for more testing controlling more of the different elements and timing.
I have, however, been very pleased with where I have placed the implant. Previously I have used my abdomen and it has been difficult to keep it functioning. On the back of my upper right arm has to some extent enabled me to forget about it and it continues functioning well. In retrospect I should have used the left arm because the vagus nerve is on the right and AIUI if I wish to stimulate the parasympathetic nervous system I should turn to lie on the right. (A good final step to NSDR aka Yoga Nidra) This has not been an issue, but I have been careful to avoid lying on the implant and it woudl be nice not to have to worry about this.
I definitely want to have a CGM when I next take Rapamycin. I have, however, being doing a range of things along with taking Rapamycin such as aiming to increase the ability of RNA Polymerase II to transcribe BECN1 (the gene for Beclin 1). (along with other long genes).
It would be really good if we could track cortisol levels in real time. I have read of research that uses interstitial fluid for that as well.
I have another 72 hours of this G7. I am tempted to power up my remaining G7 session to follow on, but that decision can wait.
Sadly my blood test from last Thursday resulted in the Courier not delivering it until Tuesday this week (Bank Holidays in the UK) which was too late. The courier is supposed to deliver it on the same day. I had another blood test today, but this does mean tracking WBC and HbA1c between the two tests won’t be possible.
I expect WBC to go down and HbA1c to go up. How quickly the Lipids move (if at all) will be interesting, but I have quite a lot of movement in those anyway so there may not be any meaningful result.
The next thing to think about is whether to increase the dose. My concern is that I would then get a longer period of disrupted sleep so I would need to have a useful school holiday within which to do this. I may even drop back down to 2mg from 4, but that is something to think about in the future.
There is, of course, the question as to what impact this is having. My objective is to increase autophagy to ensure that the mitochondrial efficiency of cells is higher so that there is a higher level of cytosolic Acetyl-CoA.
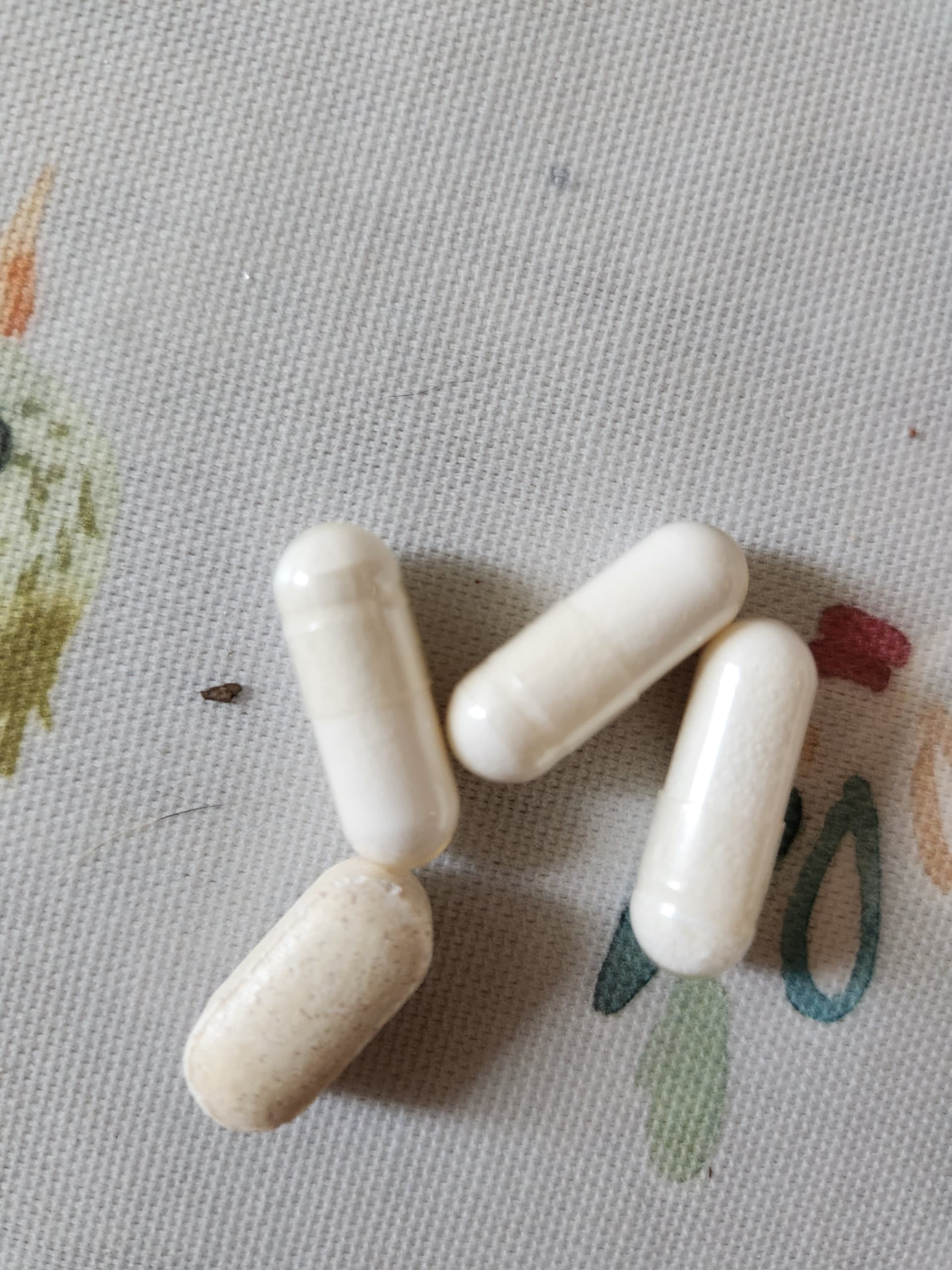
Obviously this is measured by the biomarkers, but I also use a macro camera to look at my bald patch. It does not take static photos that well, but here is one:
What seems to be happening is the developing of quite a few further dark pigmented hair follicles and really fine pigmented hair coming from some of them. I start with the assumption that hair grows quite slowly and the newer follicles have either shorter hair or no hair and just the skin colouring that preceeds producing hair.
It is, of course, the same processes for other cells, but not as visible.