I assume she’s referring to these studies.
1 Like
From Krister…“I would not interpret Kaeberlein’s current view as that rapamycin makes people immune to cancer and alzheimer’s. I know he is very frustrated that trials on Alzheimer’s and Rapamycin because of the promising potential. But he would not say that rapamycin makes humans immune to cancer or alzheimer’s. Even mice who take Rapamycin gets cancer. I think the Radiolab podcast is just a wrong saying from him which happens easy in podcast interview.”
Exactly… which is why I emphasized twice in “mice studies”… do we extrapolate that to people? There does seem a cancer stalling benefit to those like Mikhail Blagosklonny and Seren Segal… lung and colon cancers.
Young people don’t have the cluttered cells, senescence cells issues of older people… and they don’t typically get alzheimer’s and cancers.
It would seem… using rapamycin to clear and repair cells (autophagy). And tamp down senescence would give same benefits as being younger.
Time will tell.
1 Like
@RapamycinCurious Thanks for the reminder of these studies. If I remember right in that thread Matt Kaeberlein, Mikhail Blagosklonny and Alan Green answer quite good about these studies. So I would not say we know that it accelerates Alzheimer’s yet. More research is needed.
@Agetron I agree that it will probably slow down development of cancer but not make people or mice immune to it. In the interview I had with Mikhail Blagosklonny he also talked little bit about that. Here is a good time clip from that interview.

2 Likes
These are great questions/issues.
I think one of the most important to consider discussing with Dr. Mannick is : Individualized Treatment:
“Do you envision a future where rapamycin treatment for longevity is individualized, taking into account genetic factors, age, and overall health? How might personalized approaches mitigate potential risks?”
Thousands of us are experimenting with rapamycin. And yet we still know nothing about the ideal dosage and have no tools to really adjust/individualize the dose. We cannot really dose based on symptoms or change in symptoms (at least for most of us) so it is a somewhat scary black box. As a physician this is really troubling, ie kind of prescribing/dosing on 'faith" based on only a few studies in humans.
Does she have/know of any biomarkers that could help with personalizing the dose?
Does she think higher doses are needed to crosss the blood brain barrier; does it need to cross the BBB?
Thanks for doing this, will be a great interview to listen to.
1 Like

In her ARDD2023 presentation, she said that pending IND-enabling studies Tornado expects to go to the clinic with TOR101 in 2024. What does she expect will be the first indication tested in humans?
In the same presentation she showed data for subchronic (28-day) toxicity on lab abnormalities in rats. Things looked good for lymphocytes, platelets, and triglycerides, but there was something weird about the cholesterol in the males that was not clear in the video. Can she clarify?
She did not present data on another lab abnormality closely associated with rapalogs in rodents and humans: hyperglycemia. Does she have data on that?
Also, she presented in vivo work on S6 phosphotylation (mTORC1 target) but not Akt (mTORC2 target). Was that consistent with the predicted very low inhibition of mTORC2 even after 28 days’ dosing?
At Hevolution, she pressed the case that rapamycin’s anti-aging effects can be translated “right now.” She sounded much more bullish than she has in previous interviews, where she’s often been very cautious. Has something made her more optimistic in the last year or so, or was she just getting feisty in response to David Gems’ inordinate skepticism?
4 Likes
I am interested in the durable effects of rapamycin. Has anyone tested the extent of the immunomodulatory effects of rapamycin beyond 2 weeks?
In rodent models, a single dose of rapamycin (or transient treatment) prolongs life and prevents obesity. Curious if she thinks this is a “reset” of the entire animal (all organs and tissues) or more likely to be immune system driven, and is there anyway to tease that out.
With pulstile dosing, we are presumably trying to “reset” something for a durable change --but want to avoid the direct acute effects of rapamycin over the long term (suppression of healthy protein synthesis and cell proliferation).
4 Likes
@Apug Good question. I’m wondering about this as well. Does rapa improve the body’s ability to heal itself (could be taken for a few months and then stopped for a few months before restarting because aging continues) or does rapa need to be taken regularly to offset some poor functioning caused by aging?
2 Likes
Right!? We are taking a “hit” so to speak each time we dose Rapa: protein synthesis/cell proliferation is suppressed. This can have negative consequences especially with high dosing (lower WBC, GI effects from mucosal layer poor turnover, delayed healing…. )
Our “payback” comes in the durable effects when rapa is no longer constantly in the system-- but has caused some persistent positive change. The immune system seems to somehow make the jump from suppression to rejuvenation-- for at least 2 weeks. Are there other systems/tissues that do something analogous? or , are there those that simply do not have any positive durable effect? What could be that mechanism of action? – and how best to use this information for specific aspects of aging (I’m specifically now thinking of my 90 year “very healthy” mother with a tibial stress fracture. Would a rapa “reset” outweigh any intermittent (if dosed say bi weekly) direct tissue healing suppression?)
3 Likes
@Apug & @Joseph_Lavelle I had the interview on Friday last week and it was really good one.
One interesting thing she mentioned was that the improved immune system could be detected up to 1 year after the treatment. Maybe, Joe, can interview her also in his podcast and dig deeper after I have released my episode in January. Now its time to edit and create slides to the podcast ![]()
4 Likes
Very interesting. I’ve seen tidbits here and there that indicate rapamycin taken for short periods of time has long lasting effects. But perhaps not permanent. This begs the question of whether it is best to take rapa regularly (1x/week forever) or take it for periods (say 1x/1-2 weeks for 3-5 mos) with regular washouts of 1-5 mos. I have already shifted to a 2 week cycle with 1 week off every 2 cycles.
2 Likes
detecting improvement for up to a year! if significant, that is incredible. I’m starting to wonder if rapamycin acts as possibly a type hormetic stressor – “hurts” in the short term but “helps/improves” in the long term. If so, that could really have implications for dosing (think dosing and volume of starting an exercise program versus maintaining, always allowing recovery…). — possibly slower and less initially but building to higher dose more frequently over time?
4 Likes
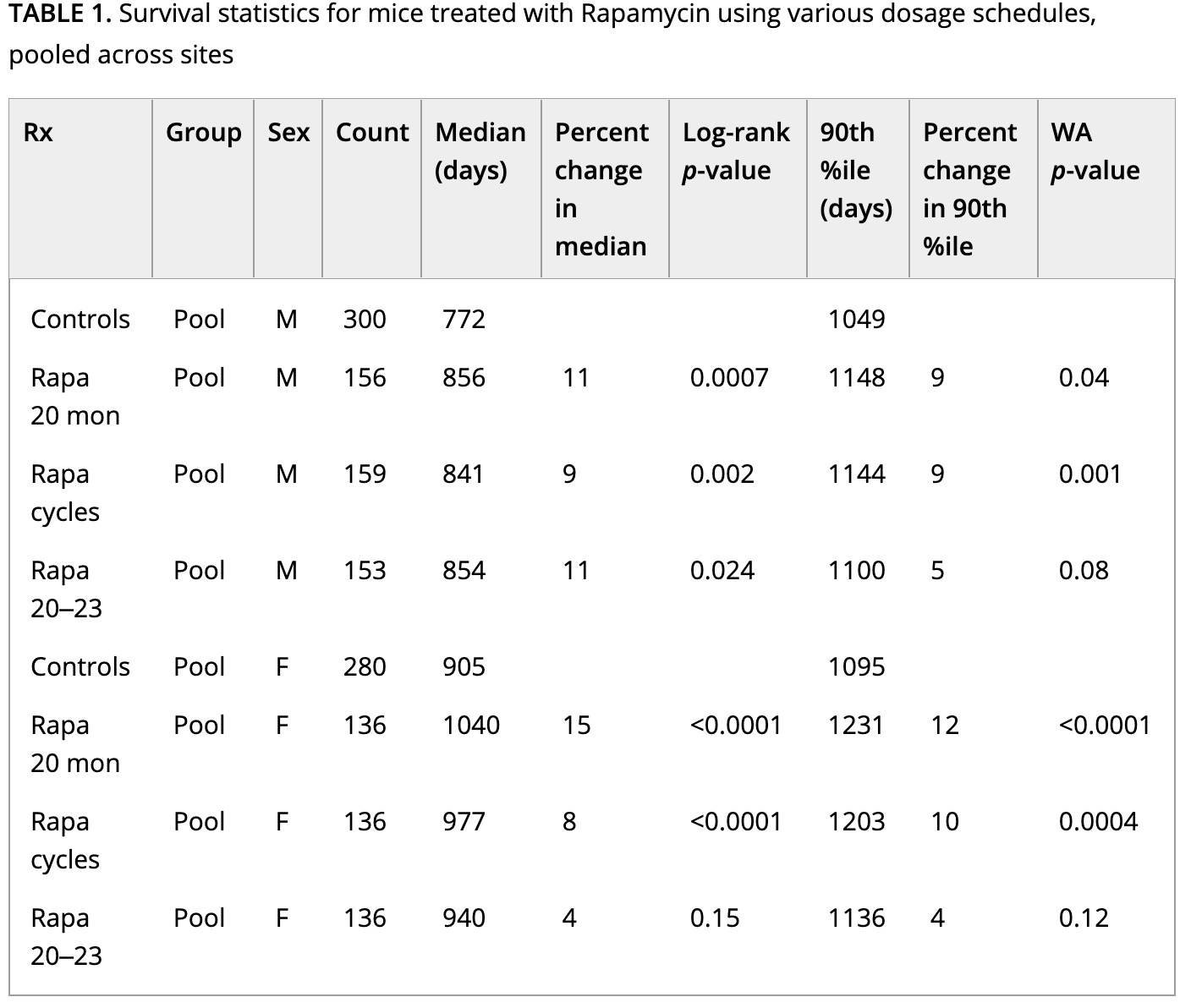
We report here longevity results using three dosing schemes: “Rapa 20 mon” in which Rapa is given at 42 ppm from 20 months until death; “Rapa cycles” in which Rapa is given for 1-month interval interspersed with drug-free months from 20 months until death; and “Rapa 20–23,” in which Rapa is started at 20 months but then terminated at 23 months.
Initiation of Rapa at 42 ppm increased survival significantly in both male and female mice. Exposure to Rapa for a 3-month period led to significant longevity benefit in males only. Protocols in which each month of Rapa treatment was followed by a month without Rapa exposure were also effective in both sexes, though this approach was less effective than continuous exposure in female mice.
Interpretation of these results is made more complicated by unanticipated variation in patterns of weight gain, prior to the initiation of the Rapa treatment, presumably due to the use of drug-free food from two different suppliers.
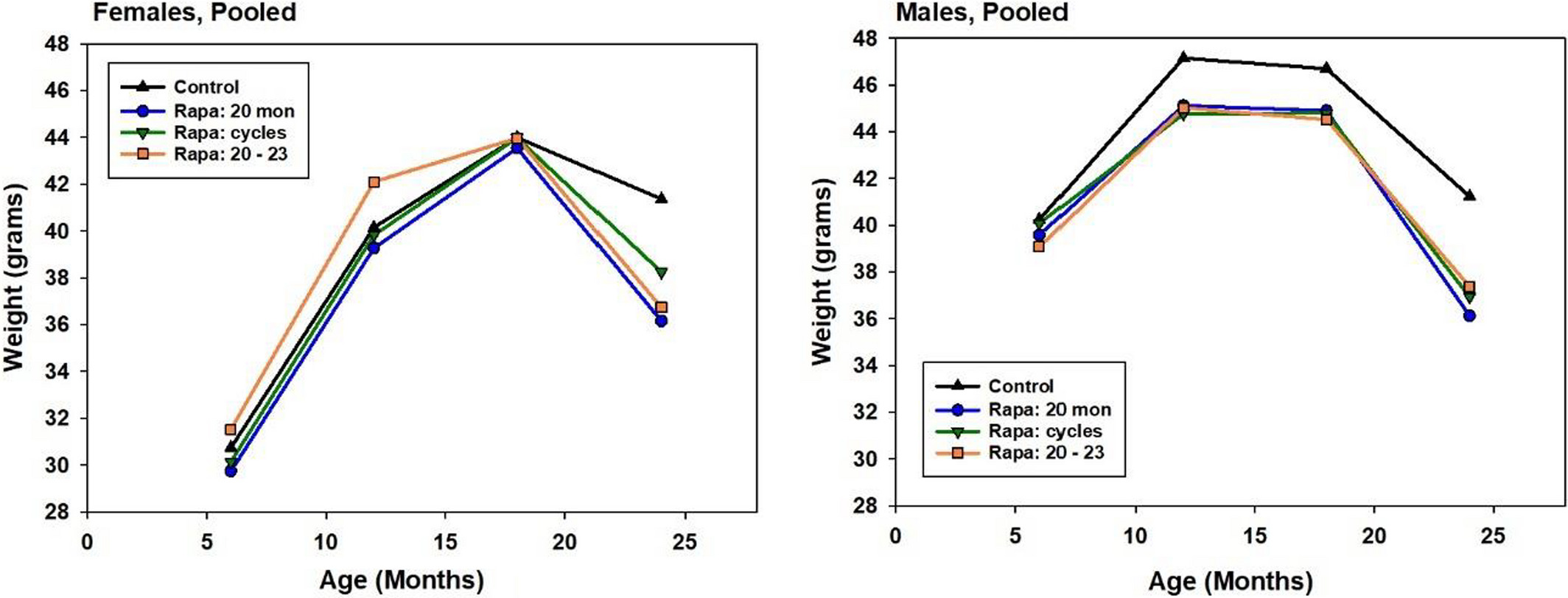
All the males on rapa had retarded growth, which makes you wonder if this was actually a form of crypto-CR rather than the biochemical effects of the rapa itself.
2 Likes
This is very good. Thanks.
If I’m reading this right, for male mice all dosage patterns worked. If the short term dosing worked as well as long term….why keep going? Because a man is not a mouse, I suppose.
Four things.
First, all of these mice were on high-dose daily rapa, not once-weekly piddley doses like almost everyone on this forum is taking.
Second, even a one-month cycle of rapa for a mouse is roughly three years for a human.
Third, the mice on rapa for only 3 months got only half the maximum lifespan increase (which is the better readout for aging) as the other groups.
And fourth, as I quoted, all of these results in the males may actually because they were on crypto-CR before they even got on rapa, so they may amount to nothing at all.
3 Likes
Thanks. A few questions.
- did the CR pre start include the controls? I thought it did.
- a daily mouse dose is roughly equivalent to what in a person: a 4-5 day cycle? Certainly not the same as daily if only for the half life difference.
No: look at the graphs. All the males that would subsequently be put on rapa gained less weight and then started losing from that lower weight from before they were dosed as compared to the animals used as controls. By contrast, the females — in whom these regimens were ineffective — all had the same pre-rapa weight trajectory.
But remember, they’re eating chow most of the day. They’re exposed to the drug throughout their waking hours. It’s not always clear in papers when they test rapa in blood, but it’s only once a day, and I’m skeptical that they’re clear of rapa after an 8-12-hour overnight fast.
1 Like
Interesting. I have heard from other researchers that when the chow is limited…not ad libitum…the mice eat it all at once. Perhaps that only applies to CR experiments, but it would be worth knowing if the rapa dosing was 1x per day or throughout the day.
Why would they treat the controls differently before the experiment start…doesn’t that confuse the findings? I guess that is your point.
1 Like
The rapa is in the food and they’re fed ad lib. This is what food intake looks like in ad lib mice:

(Source). (C) is ad lib; ((G) and (K) are different time- but not energy-restricted feeding regimens; (O) is circadian-aligned CR and (S) is circadian-opposite CR. The rapa dosing would look like the pellet consumption in (C), and levels would stay elevated beyond their last bite of chow.
The didn’t intend to do this. As I quoted the authors,’
Interpretation of these results is made more complicated by unanticipated variation in patterns of weight gain, prior to the initiation of the Rapa treatment, presumably due to the use of drug-free food from two different suppliers.
Just like their original fortuitous mistake with rapa fortification of the chow in 2009, this was just a logistical problem that turned out to have major consequences.
4 Likes
Thanks for posting. The fact that mice eating ad libidum eat their food within a roughly 12 hour window means they get their rapamycin dose in 12 hours and then get about a 12 hour break until their next daily dose. Since 12 hours is almost one rapamycin half-life for mice, this means they get a break of almost one half-life between doses. Comparing this to humans and their longer half-life, this would be more similar to humans getting their rapamycin dose for two days in a row and then two days off (almost one half-life). This would be somewhat of a mini cycling of the dose. The break between doses is not enough for levels to drop to very low, but it’s low enough to drop in half and lead to fluctuation in mTOR levels. In effect this means the dose that increases life-span in mice is not equivalent to a daily dose but more similar to a few days on few days off for humans.
2 Likes
This analysis would work very well if the rodents and human self-experimenters were taking equivalent allometrically-scaled doses. But they aren’t, and when thinking about how it translates we have to account not only for the rate of decay (the half-life) but the starting dose. The mice are on much higher doses than nearly any self-experimenters, even after adjusting for metabolic scaling, such that their trough levels are still higher than humans encounter (or encounter very briefly in a one-week cycle). See this handy chart from @RapAdmin
(Don’t fool yourself by “double counting” using the dose already (roughly) adjusted for half-life).
3 Likes