In the absence of Pyridoxamine being careful to limit dosing of B6 is key. Also ideally taking the active form as well.
What about the source from Japan that RapAdmin mentioned in this thread? The Stiffening Trap: How Aging Tissues Strangle Their Own Blood Supply - #4 by RapAdmin ?
2 Likes
how do you access it in europe? I only see it being sold by one brand, the supersmart Company. That is company I have not bought from before.
1 Like
STOP IT! The efficacy of active vitamin B6 in raising plasma PLP levels is inferior to that of an equivalent dose of pyridoxine. Many people advocate for the active form without understanding the underlying rationale. It is time to stop blindly recommending P5P; the clinical nuances here are far more complex than they appear.
1 Like
The issue with pyridoxine is that you can get toxicity as it self inhibits. Here is a list of cases from chatGPT 5.5-paid
response:
Below is a working list of published case reports / case series of vitamin B6 toxicity that I could identify, with the B6 form stated where the source makes it clear.
| Case report / series | URL | B6 form identified |
|---|---|---|
| Schaumburg et al., 1983, Sensory neuropathy from pyridoxine abuse | https://www.nejm.org/doi/full/10.1056/NEJM198308253090801 | Pyridoxine; title and PubMed record identify pyridoxine abuse. (PubMed) |
| Parry & Bredesen, 1985, Sensory neuropathy with low-dose pyridoxine | https://pubmed.ncbi.nlm.nih.gov/2993949/ | Pyridoxine; 16 patients, 0.2–5 g/day. (PubMed) |
| Foca, 1985, Motor and sensory neuropathy secondary to excessive pyridoxine ingestion | https://pubmed.ncbi.nlm.nih.gov/2994596/ | Pyridoxine. (PubMed) |
| Dalton & Dalton, 1987, Characteristics of pyridoxine overdose neuropathy syndrome | https://pubmed.ncbi.nlm.nih.gov/3630649/ | Pyridoxine. (PubMed) |
| Albin et al., 1987, Acute sensory neuropathy-neuronopathy from pyridoxine overdose | DOI listed in review: https://doi.org/10.1212/WNL.37.11.1729 | Pyridoxine; cited as pyridoxine overdose. (www1.racgp.org.au) |
| Santoro et al., 1991, Pyridoxine neuropathy: a four-year electrophysiological and clinical follow-up of a severe case | https://pubmed.ncbi.nlm.nih.gov/1867126/ | Pyridoxine. (PubMed) |
| Morra et al., 1993, Sensory and motor neuropathy caused by excessive ingestion of vitamin B6: a case report | https://pubmed.ncbi.nlm.nih.gov/8150322/ | Vitamin B6, specific vitamer not clear from accessible abstract/title; likely supplement B6, but I would not label it definitively as pyridoxine without full text. (PubMed) |
| de Kruijk & Notermans, 2005, Sensory disturbances caused by multivitamin preparations | https://pubmed.ncbi.nlm.nih.gov/16320661/ | Multivitamin B6, specific vitamer not clear from accessible abstract. (PubMed) |
| Silva & D’Cruz, 2006, Pyridoxine toxicity courtesy of your local health food store | https://pmc.ncbi.nlm.nih.gov/articles/PMC1798481/ | Pyridoxine. (PMC) |
| Gdynia et al., 2008, Severe sensorimotor neuropathy after intake of highest dosages of vitamin B6 | https://pubmed.ncbi.nlm.nih.gov/18060778/ | Pyridoxine; reported as 9.6 g/day pyridoxine. (PubMed) |
| Castagnet et al., 2010, Chronic demyelinating polyneuropathy and B6 hypervitaminosis | https://pubmed.ncbi.nlm.nih.gov/20627481/ | Vitamin B6, specific vitamer not clear from accessible abstract. (PubMed) |
| Kulkantrakorn, 2014, Pyridoxine-induced sensory ataxic neuronopathy and neuropathy: revisited | https://pubmed.ncbi.nlm.nih.gov/25056196/ | Pyridoxine, 600 mg/day in B1-B6-B12 combination tablets. (PubMed) |
| Bacharach et al., 2017, Pyridoxine toxicity small fiber neuropathy with dysautonomia | https://pubmed.ncbi.nlm.nih.gov/28827489/ | Pyridoxine. (PubMed) |
| Echaniz-Laguna et al., 2018, Regressive pyridoxine-induced sensory neuronopathy in a patient with homocystinuria | https://casereports.bmj.com/content/2018/bcr-2018-225059 | Pyridoxine. (PubMed) |
| Moudgal et al., 2018, Vitamin B6 toxicity revisited: reversible pyridoxine-associated neuropathy and disequilibrium | https://www.neurology.org/doi/10.1212/WNL.90.15_supplement.P4.021 | Pyridoxine. (American Academy of Neurology) |
| Borst & Tchapyjnikov, 2018, B6 and Bleeding: a case report of a novel vitamin toxicity | https://pubmed.ncbi.nlm.nih.gov/29610166/ | Pyridoxal-5-phosphate therapy in PNPO deficiency; source also warns about pyridoxine or PLP supplementation. (Scholars@Duke) |
| Ames et al., 2020, A cautionary tale of pyridoxine toxicity in cystathionine beta-synthase deficiency | https://pubmed.ncbi.nlm.nih.gov/32820583/ | Pyridoxine. (PubMed) |
| Tynes et al., 2021, Regular intake of energy drinks and multivitamin supplements is associated with elevated plasma vitamin B6 levels… | https://pmc.ncbi.nlm.nih.gov/articles/PMC8426371/ | B6/pyridoxine from energy drinks and multivitamins; case report/clinical report rather than classic journal “case report” title. (PMC) |
| Van den Broeck et al., 2022, Neurogenic voiding dysfunction induced by vitamin B6 overdose | https://doi.org/10.1016/j.contre.2022.100004 | Pyridoxine / vitamin B6 from excessive multivitamins. (ResearchGate) |
| Guala et al., 2022, Vitamin B6 neonatal toxicity | https://pmc.ncbi.nlm.nih.gov/articles/PMC9747291/ | Vitamin B6 supplement in pregnancy/breastfeeding; the specific vitamer is not clear from accessible snippets. (PMC) |
| Bugeme et al., 2023, Vitamin B6 induced sensory polyneuropathy: about two clinical observations | https://lupinepublishers.com/neurology-brain-disorders-journal/pdf/OJNBD.MS.ID.000244.pdf | Vitamin B6, specific vitamer not clear from accessible text. (Lupine Publishers) |
| Paluszny & Qiu, 2023, Vitamin B6 toxicity secondary to daily multivitamin use | https://www.cureus.com/articles/199499-vitamin-b6-toxicity-secondary-to-daily-multivitamin-use-a-case-report | Multivitamin B6, specific vitamer not clear from accessible text; case reported 6 mg/day in a multivitamin. (Cureus) |
| Kościńska-Shukla et al., 2025, Underestimated pyridoxine consumption and neurotoxicity | https://link.springer.com/article/10.1007/s00296-025-05900-9 | Pyridoxine; one case explicitly involved 200 mg pyridoxine tablets; others involved B-rich foods/sports supplements or high nut intake. (Springer) |
| Gdynia et al., 2025, Polyneuropathy due to vitamin B6 hypervitaminosis: a case series | https://ruralneuropractice.com/polyneuropathy-due-to-vitamin-b6-hypervitaminosis-a-case-series-and-call-for-more-education/ | Mostly polyvitamin preparations; paper frames toxicity as vitamin B6/pyridoxine but does not specify the exact vitamer in each preparation. (ruralneuropractice.com) |
| Barratt & Achari, 2025, 7 Cases of Vitamin B6 toxicity | https://www.neurology.org/doi/10.1212/WNL.0000000000208917 | Energy drink-associated B6, specific vitamer not clear from abstract. (American Academy of Neurology) |
Pattern: the published toxicity case literature overwhelmingly involves pyridoxine, usually as pyridoxine hydrochloride in supplements/multivitamins, but several recent reports only state “vitamin B6” or “multivitamin/energy drink” without specifying the vitamer in the accessible abstract. The main clear exception above is pyridoxal-5-phosphate in the Borst & Tchapyjnikov bleeding case.
In short P5P although it has one report is much safer. Low dose pyridoxine is OK, however. Some of the reported problems, however, are with a dose more like 10mg than 50mg.
Claims of neuropathy occurring at doses below 200 mg can essentially be dismissed as false. To date, no objective neurological examinations across any studies have ever detected such an effect at these levels. You will even find individuals claiming to experience neuropathy from a mere 2 mg dose, but this is purely subjective, if not entirely psychological.
The FNB noted that although several reports show sensory neuropathy occurring at doses lower than 500 mg/day, studies in patients treated with vitamin B6 (average dose of 200 mg/day) for up to 5 years found no evidence of this effect.
I personally experienced a mild neuropathy (tingling) from I think 100mg, but I would need to check. I accept that to get severe symptoms requires a higher dose, but I think it is best to avoid any conflict.
Different regulators take different views:
https://efsa.onlinelibrary.wiley.com/doi/10.2903/j.efsa.2016.4485
SCF (2000) set a Tolerable Upper Intake Level (UL) based on adverse neurological effects of vitamin B6 in humans. For setting a UL for vitamin B6, SCF (2000) focused on a study in women attending a clinic for the treatment of premenstrual syndrome and who received supplemental vitamin B6, for less than 6 months to more than 5 years (Dalton and Dalton, 1987). In this study, out of 172 women, high supplemental doses of vitamin B6 taken for long periods (on average about 100 mg/day for 2.9 years) were related to the development of reversible peripheral sensory and motor neuropathy in 103 women. The symptoms included ataxia, muscle weakness and an impaired sense of touch of the limbs. However, the studies on adverse effects of vitamin B6 were not carried out under controlled conditions.
The SCF could not establish a No Observed Adverse Effect Level (NOAEL). The SCF considered that severe toxicity can be produced at doses of 500 mg/day or more, and that minor neurological symptoms may be apparent at doses of 100 mg/day or more if consumed for long periods. Using twice an uncertainty factor of 2 on the average intake (about 100 mg/day) observed in one study (Dalton and Dalton, 1987), a UL of 25 mg/day was derived for adults, including pregnant and lactating women. For children from 1 year of age onwards, the UL was extrapolated from the adult UL on a body weight basis, and was set at values between 5 mg/day (for 1–3 years) and 20 mg/day (for 15–17 years).
So the EU goes for 25mg a day.
What does the Department of Health and Social Care advise?
You should be able to get the vitamin B6 you need by eating a varied and balanced diet.
If you take vitamin B6 supplements, do not take too much as this could be harmful.
Do not take more than 10mg of vitamin B6 a day in supplements unless advised to by a doctor.
The UK says no more than 10mg unless advised by a doctor.
chatGPT5.5-paid summary:
Regulators usually give two different numbers for pyridoxine / vitamin B6:
- Requirement / recommended intake: roughly 1–2 mg/day for adults.
- Safety ceiling / upper limit: varies a lot, from about 10–12 mg/day in the more cautious European/UK approach up to 100 mg/day in the older US/Canada/ASEAN-style approach.
Adult pyridoxine / vitamin B6 levels by regulator
| Jurisdiction / regulator | Adult recommended intake | Adult upper / safety limit | Notes |
|---|---|---|---|
| UK / NHS / DHSC advice | Men 1.4 mg/day, women 1.2 mg/day | Do not take >10 mg/day in supplements unless advised by a doctor | This is supplement-specific public advice, not a total-diet UL. (nhs.uk) |
| EU / EFSA 2023 | EFSA PRI: women 1.6 mg/day, men about 1.7 mg/day | 12 mg/day adult UL, including pregnancy/lactation | EFSA lowered the previous adult UL substantially because of peripheral neuropathy concerns. (EFSA Journal) |
| US / National Academies; NIH summary | Most adults 1.3 mg/day; older adults higher | 100 mg/day adult UL | US UL is much higher than EFSA’s newer UL. NIH notes EFSA’s newer 12 mg/day limit as a lower expert limit. (NCBI) |
| Canada / Health Canada | Uses North American DRI framework, broadly similar to US | Historically aligned with 100 mg/day UL, but 2026 safety review found possible neuropathy link at ≥10 mg/day in natural health products | Health Canada plans label-risk updates for products with daily dose ≥10 mg B6. (Canada) |
| Australia / New Zealand NRVs | Adults about 1.3–2.0 mg/day depending age/sex | 50 mg/day adult UL | Separate TGA medicine rules require warnings above 10 mg/day and cap adult products at 100 mg/day. (eatforhealth.gov.au) |
| Australia TGA product rules | Not an intake recommendation | Warning if product gives >10 mg/day; current max 100 mg/day for adults; from 1 June 2027, >50 mg/day moves out of general sale | Higher-dose products will require pharmacist/prescription access depending dose. (Therapeutic Goods Administration (TGA)) |
| Singapore / HSA | Not mainly framed as intake recommendation | Health-supplement max 100 mg/day for adults | HSA says this aligns with ASEAN, Canada and US limits. (Health Sciences Authority) |
| ASEAN health supplement standard | Not a dietary RDA | Health supplement max 100 mg/day | Listed as maximum level in health supplements. (ASEAN Main Portal) |
| Netherlands | Follows EU-style risk management | Supplement max 21 mg/day since 2018 | This predates EFSA’s 2023 12 mg/day UL. (Lareb) |
| Norway | Nordic/European context | Historical supplement maximum 4.2 mg/day; VKM assessed scenarios up to 25 mg/day | Norway has been unusually conservative for supplements. (vkm.no) |
| New Zealand Medsafe safety note | RDI 0.5–1.7 mg/day, depending age/sex | Medsafe has discussed limits/warnings; current note stresses neuropathy risk and cumulative intake | Medsafe’s 2025/2026 updates are safety warnings rather than a simple adult UL table. (Medsafe) |
Practical interpretation
For ordinary nutrition, regulators converge around about 1–2 mg/day. The disagreement is about long-term supplemental dosing.
The most conservative current regulatory-style position is effectively:
- ~1–2 mg/day is enough for normal requirements.
- 10 mg/day supplemental pyridoxine is treated as a caution threshold in the UK, Australia/TGA labelling, and now Health Canada labelling discussions.
- 12 mg/day total vitamin B6 is EFSA’s newer adult tolerable upper intake level.
- 50–100 mg/day remains allowed or historically recognised in several jurisdictions, but these levels are increasingly accompanied by neuropathy warnings.
So, for long-term self-supplementation, the safest cross-regulator answer is: keep chronic pyridoxine below about 10–12 mg/day unless there is a specific medical indication and monitoring.
Many companies have substituted pyridoxal-5-phosphate for their pyridoxamine. Life Extension, for example. Is there evidence for this substance causing neuropathy? How much pyridoxal-5-phosphate is the upper limit?
Asking chatGPT it tends to be a global B6 limit. However, the problem is particularly with pyridoxine. P5P tends to be more expensive and hence a smaller dose.
It is also important to monitor total overall dose.
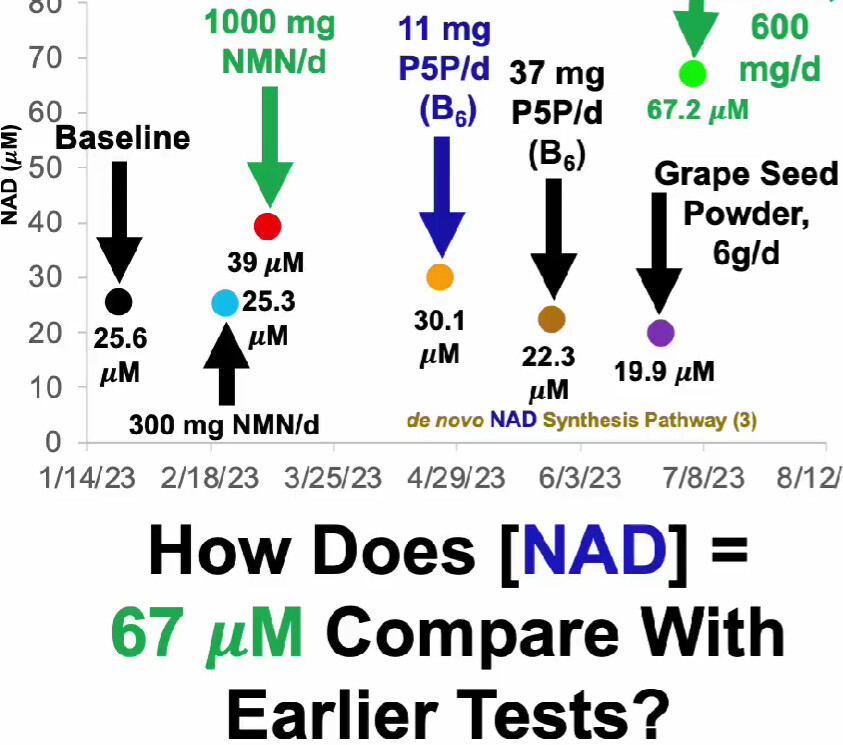
While it would be ideal if P5P offered the same benefits as PN, the reality is that PN is supported by a massive body of research. Based on my in-depth analysis of the literature—evaluating the raw data and cutting-edge studies rather than merely reading abstracts—long-term PLP supplementation is highly detrimental to longevity. The underlying data is overwhelmingly negative. Setting my personal analysis aside, Mike Lustgarten has also shown in his videos that his NAD levels dropped below baseline after taking 37mg of P5P. I strongly advise against using it.
My approach when arguing a case is to obtain references that substantiate my view so that it is possible for other people to read the evidence. I have also got paid chatGPT,claude and gemini accounts.
I put the question “what research exists as to the effect of pyridoxal-5-phosphate supplementation on longevity” into all three. They all say having low serum P5P is bad for longevity. P5P is the active form. However, there is not really much on the issue of supplementation and longevity.
I find the interplay between the B vitamins quite interesting. I like @ConquerAging 's work, but I would not make a decision purely on his reporting of any particular impact on his own metabolism.
I have no problem with the idea that @Cole and I disagree about whether or not to supplement B6, how much to supplement and which form.
However, I think relying on the US regulator when all the other regulators take a different view is a mistake.
If I don’t respond to any other point on this matter that is simply because I have not seen any argument as to why I should change my mind that is worth responding to. I don’t need the last response on any discussion.
I will continue supplementing with P5P although when reordering I may look at taking the dose down a touch.
Are we talking about pyridoxine/P5P neuropathy because there is a theoretical risk of neuropathy from pyridoxamine supplementation?
I think we are talking about it because there is a question as to what is the best form of B6 to supplement. (given that pyridoxamine is hard to get).
I don’t see any point of mega-dosing P5P or pyridoxine when the topic is specifically about pyridoxamine and its unique glycation-inhibiting properties.
2 Likes
There have been reported cases of neuropathy associated with pyridoxal-5-phosphate (P5P), even at very low doses, though overall instances are extremely rare. Currently, safety upper limits for vitamin B6 are based entirely on data from pyridoxine, as long-term safety data specifically for P5P remains unavailable. Theoretically, P5P should be significantly safer than pyridoxine. I suggest you either adhere to the standard safety guidelines for general vitamin B6, or base your intake on the dosages currently utilized in short-term P5P clinical trials.
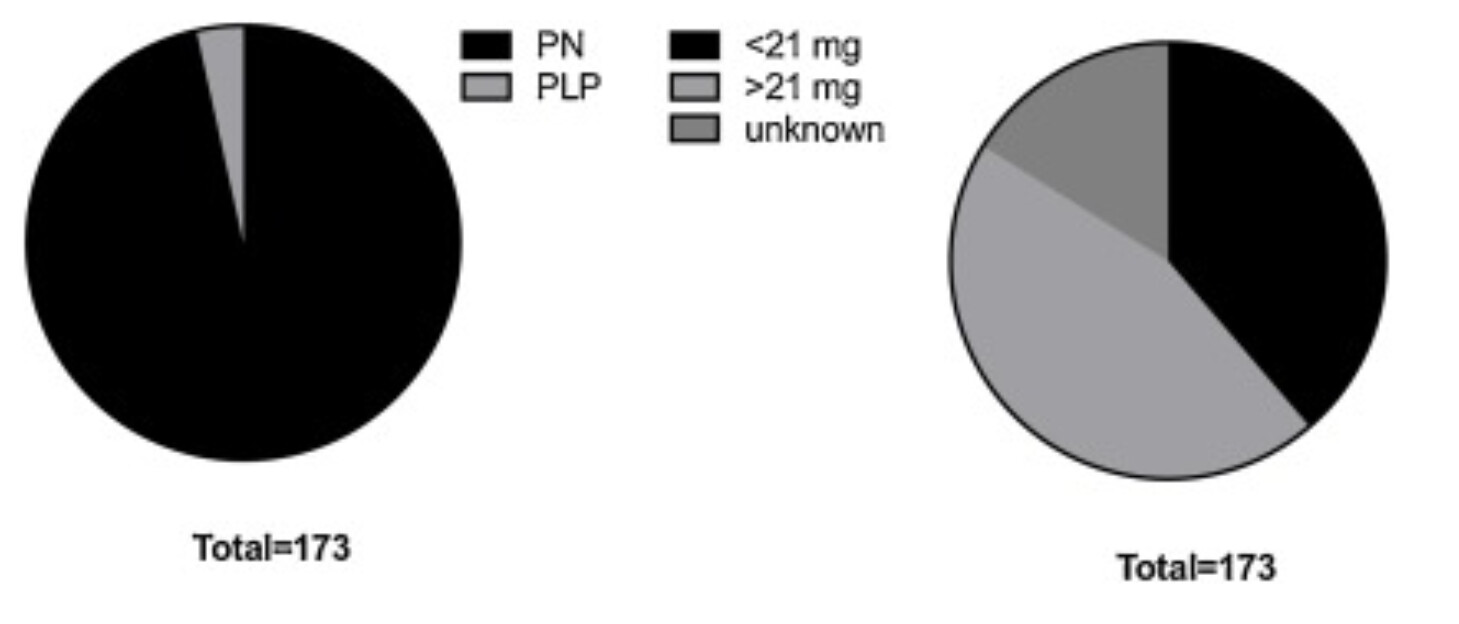
The chart above shows which forms of vitamin B6 were used in cases of vitamin B6–related neuropathy.
It’s an option, but unfortunately you also have to take NAC at 900mg+ to get the approx. 300mg of pyridoxamine… because they all package it that way:
The most useful analytical takeaway is the cross-positioning itself. The identical NAC 300 + pyridoxamine 75 mg tablet is sold by Cafoli as a respiratory mucolytic, by Alniche/Steris as a nephroprotective, and (on some pages) as a dietary supplement — three incompatible regulatory framings for one molecule. That’s the signature of a marketing-led fixed-dose combination with no settled, regulator-sanctioned indication behind it, riding on the antioxidant/anti-AGE rationale of two component molecules whose combination was never approved in a stringent market. None of these four products clears your top-tier entry bar; they’re branded-generic/PCD marketing SKUs.
1 Like
Taking the “active form” is not ideal at all, and in fact, in terms of antiglycative effects, pyridoxamine is the most active form.
Typically pyridoxal-5-phosphate is referred to as the active form of B6, becuase it is the coenzymatically active form that cells use. However, it does not get absorbed intact to a significant extent because it gets hydrolyzed into pyridoxal in the digestive tract, so paying more for the so called “active form” is basically a waste of money.
Also if we’re talking about anti-glycative benefits, then pyridoxamine is the most active form of vitamin B6. You’ll get weaker effect if you consume pyridoxal-5-phosphate or pyridoxine or any other form.
I agree with you though that avoiding toxicity is important. While for most people, it’s not a concern at 100 mg or less daily, there are rare exceptions to that rule as evidenced by case reports in the literature. This usually only shows up after long term exposure. This probably reflects different genes, but some people would be extra sensitive for whatever reason. In any case, regardless of the dose one takes, to reduce the risk of toxicity it is generally adviseable to spread the dose throughout the day and take it with meals to even out the concentration of it in the blood and cells.
All the forms can cause neuropathy. including pyridoxal-5-phosphate. Pyridoxine is the one most likely to cause neurotoxicity.
2 Likes
the easiest and cheapest way to get pyridoxamine is as a research-grade reagent; standalone consumer products are quite rare. To be honest, I’ve never worked in a laboratory, so I’m not sure if substances sold as research reagents are safe for human consumption. From what I’ve observed, their production and bottling lines handle various chemical compounds, meaning the equipment isn’t dedicated solely to pyridoxamine. I have the exact same concern regarding 17α-estradiol. @RapAdmin
1 Like
Buying most chemicals from Legit research lab sales websites is actually pretty hard - they validate that you are part of a lab or educational research group. You can’t, as a typical consumer, just go to the Sigma Aldrich website and expect to buy the reagents.
Then there are the whole world of grey-market “research products” - and thats anther game entirely. Can you trust them? Probably not something you want to do for a long-term dosing strategy (at least I wouldn’t).
2 Likes
In looking at the issue with chatGPT(5.5) I had a partial response on pyridoxamine: “Pyridoxamine is not widely marketed because it was previously developed as a pharmaceutical candidate for diabetic complications, limiting its commercial availability in many countries.”
As far as I can tell it has a dynamic equilibrium with P5P. Although P5P cannot pass into cells it can be dephosphorylated and then pass into cells and be rephosphorylated which is safer than PN. There are a lot more reports from overdosing of PN than P5P. Whichever way B6 is something to be careful with. Particularly Pyridoxine (PN).
Hence unless you can actually supplement with PM (where the active component is phosphorylated to Pyridoxamine 5′-phosphate) best supplement with P5P.