“Although REDMOD outperformed experienced radiologists, the team notes that it still needs further testing in high risk patients, including those with unexplained weight loss and newly diagnosed diabetes, before it can be used widely in clinical settings.”
It’s not yet used to diagnose in clinical settings. I bet your doc “loves” you.
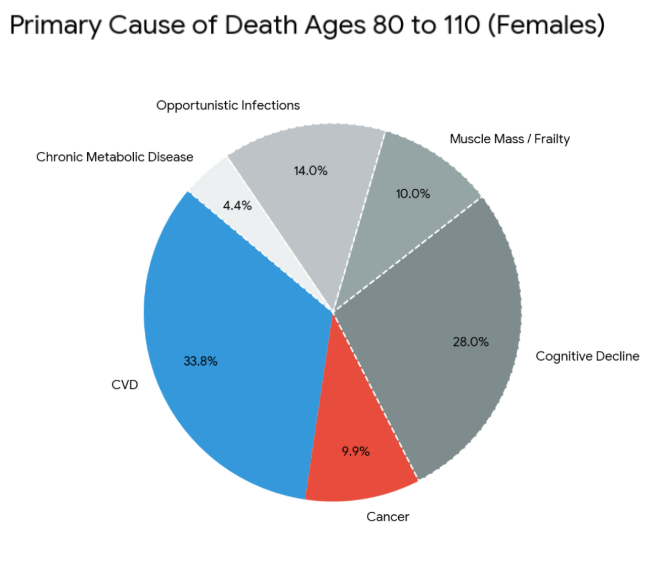
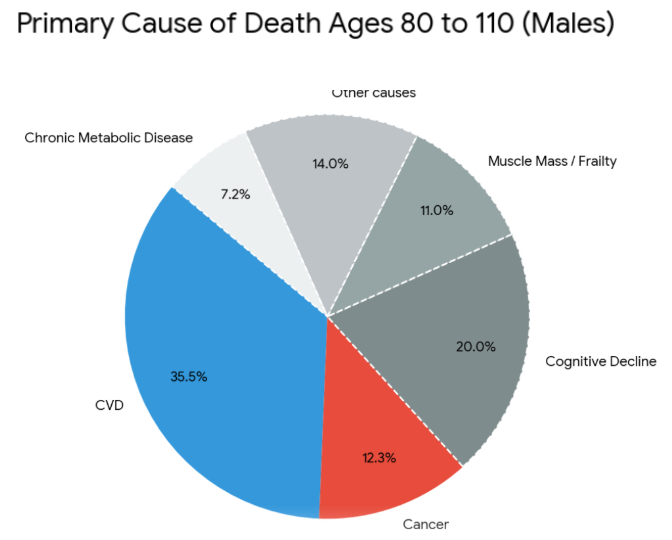
Some factoids from various AIs. I was a little surprised at some of the results. Of course, these figures will vary depending on the populations studied. These are for the USA. One reason I was surprised was because of a fairly common saying I used to hear from time to time: “We all get cancer if we live long enough.” That certainly isn’t the case. Also, I thought the risk of getting cancer increased as we got older. That certainly isn’t the case either.
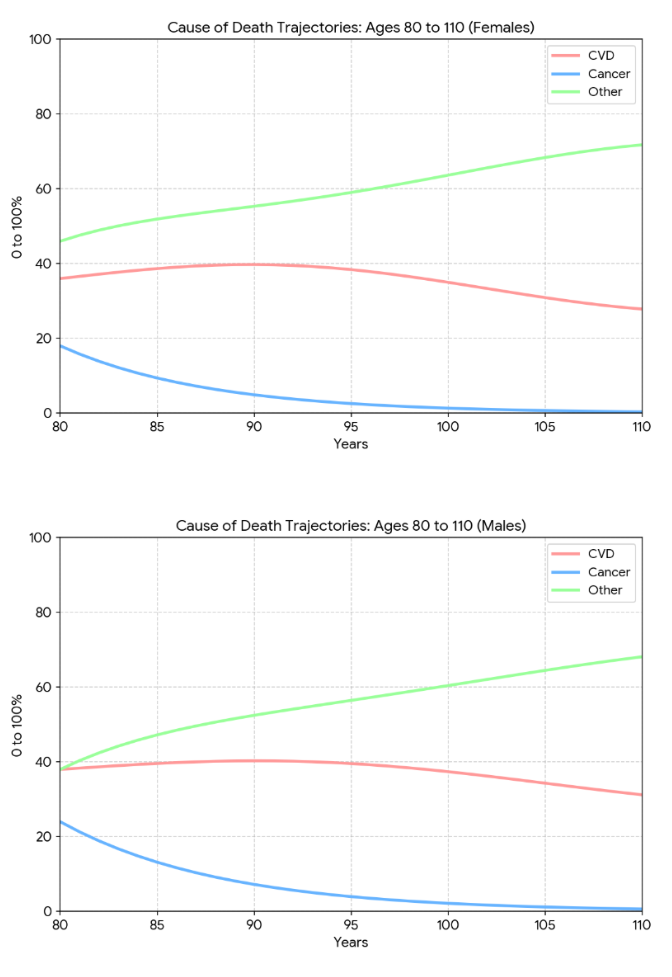
While for ages 80-110 taken as a whole, CVD is the single largest cause of death in both sexes, but the answer is genuinely “Other” once you aggregate everything that isn’t CVD or cancer — Alzheimer’s, stroke, pneumonia, COPD, frailty/old age, falls, sepsis, and so on. In 2024 in the U.S., heart disease was the leading cause of death for those 80 and older, but its share shrinks dramatically as age advances. USAFacts
As an aggregate category, "Other Causes" becomes the largest sector over the entire 80–110 age span. This is because “Other” groups together dozens of distinct conditions that increase drastically with extreme age, including Alzheimer’s disease/dementia, respiratory infections (like pneumonia), chronic kidney disease, accidents (such as fatal falls), and frailty/senescence.
I find the trajectories very interesting, and they weren’t what I expected.
Let me share a basic tip on preventing gastric cancer: Helicobacter pylori (H. pylori) is the leading Group 1 carcinogen responsible for stomach cancer, but testing for it is actually quite nuanced. For non-invasive screening, the best combo right now is the Urea Breath Test (UBT) combined with a Stool Antigen Test. If you want the highest possible accuracy, the ultimate combination is the Stool Antigen Test plus H&E (Hematoxylin and Eosin) staining. Relying on any single test carries a pretty high risk of a missed diagnosis (false negative), especially for people whose gastric microenvironment isn’t in great shape.
H. pylori infects over half the world’s population.
Stomach cancer is relatively uncommon in the U.S. (1.4% of all cancers), but more common in East Asia, Eastern Europe, and parts of Latin America.
About 1–3% of people with chronic H. pylori infection will ever develop stomach cancer.
Worldwide, assuming no change to the current gastric cancer control measures, 15.6 million gastric cancer cases are expected to occur within these birth cohorts, of which 76% are attributable to H. pylori infection and are therefore potentially preventable.
I seriously don’t get how anyone could dispute H. pylori screening, let alone people giving those takes a thumbs-up. But as I always say, just let them stick to their guns. Life would be too boring if everyone was sensible.
An upper GI scope 4 years ago showed that I had intestinal metaplasia. A recent scope six months ago did not find any. It is possible that the biopsy missed it, or perhaps h pylori eradication, careful diet, and rapamycin has reversed the condition. The Correa cascade is thought to be irreversible so prevention is always best. Good old pepto bismol can help kill h pylori but multiple antibiotics are still needed
Did they associate your dysplasia with h pylori? I mean did you have it and then killed it with antibiotics? How did it go? I know people who went through a full optimized bismuth quadruple therapy and then tested positive in 6 months, then repeated the therapy and still live with h pylori. Even quadruple therapy does not sometime eradicate it. It’s not 100% guaranteed. It’s only 97-98%. It’s nice to know though that only 1-3% of the infected population develop cancer. Most people do not. And eradication process is too brutal.
I was diagnosed with h pylori about 20 years ago. I was treated with two antibiotics at that time and don’t recall which ones. I’ve had stomach issues ever since. In hindsight it was self inflicted since I drank too much alcohol for years. Abstaining from alcohol and salt are two things high on the list for stomach cancer prevention
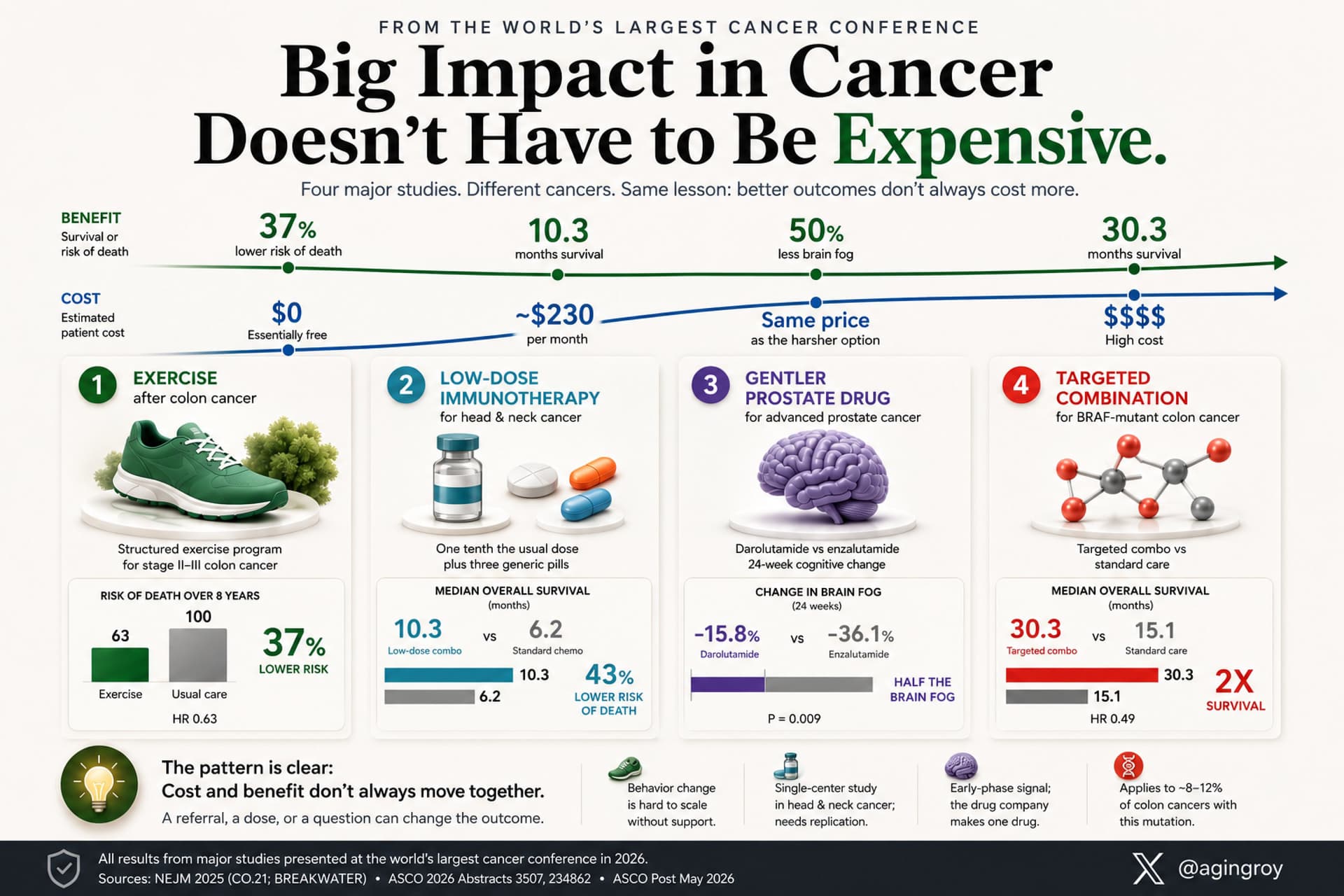
The data from recent the American Society of Clinical Oncology (ASCO) 2026 annual meeting highlights a critical, often underreported shift in oncology: significant survival gains can be achieved through non-pharmacological interventions, dose optimization, and toxicity management, rather than relying solely on high-cost novel therapeutics.
The following structured analysis categorizes these four key findings by cost-efficiency, detailing their clinical outcomes, systemic economic impacts, and the therapeutic trade-offs presented.
Intervention: A structured physical exercise program implemented following primary treatment for colon cancer.
Clinical Outcomes:
37% reduction in the relative risk of death.
8-Year Survival Rate: 90% in the exercise cohort versus 83% in the usual care cohort.
Economic Impact: Health economists classified the intervention as “dominant.” In health economics, a dominant strategy is one that simultaneously improves clinical outcomes (extends life) while reducing total healthcare system expenditures relative to the comparator.
Intervention: Administration of 1/10th of the standard dose of an immune checkpoint inhibitor (programmed death receptor-1 [PD-1] or programmed death-ligand 1 [PD-L1] inhibitor), combined with three generic adjuvant medications.
Clinical Outcomes:
Median Overall Survival (mOS): 10.3 months for the low-dose combination versus 6.2 months for standard-of-care chemotherapy.
Economic Impact: This regimen costs approximately $230 per month, a fraction of the cost associated with standard-dose checkpoint inhibitors, which frequently exceed $10,000 per month. This protocol, developed by researchers in Mumbai, demonstrates a scalable model for low- and middle-income countries (LMICs).
3. Toxicity Mitigation via Next-Generation Anti-Androgens (Prostate Cancer)
Intervention: Comparative tolerability of the second-generation androgen receptor inhibitors darolutamide versus enzalutamide in advanced prostate cancer.
Clinical Outcomes: Both agents demonstrate equivalent efficacy regarding objective response rates and progression-free survival. However, darolutamide resulted in a 50% reduction in the incidence of cognitive impairment (brain fog) compared to enzalutamide.
Economic & Practical Impact: Because both therapies occupy a similar pricing tier, the financial cost remains neutral. The clinical “win” relies entirely on provider education and patient advocacy to select the agent with the superior central nervous system (CNS) safety profile.
Intervention: A combination regimen targeting the BRAF V600E mutation in metastatic colorectal cancer.
Clinical Outcomes:
Median Overall Survival (mOS):Doubled to 30 months compared to 15 months with standard chemotherapy controls.
Economic & Practical Impact: This represents a high-cost specialty therapeutic intervention. Unlike many marginal oncology approvals, the substantial magnitude of the survival benefit (1:2 survival ratio) provides a clear clinical justification for the financial expenditure.
Clinical Implications & Paradigm Shift
The 2026 data challenges the prevailing assumption that advancing oncology care inherently requires exponential financial investment. The findings establish three distinct pathways for improving patient outcomes:
Pathway
Mechanism
Primary Barrier
Behavioral Oncology
Epigenetic and metabolic modulation via structured exercise.
Regulatory frameworks and pharmaceutical margin misalignments.
Selective Prescribing
Prioritizing agents with lower blood-brain barrier penetration (darolutamide).
Physician awareness and default prescribing habits.
Scholarly Note & Knowledge Gaps: While the Mumbai low-dose immunotherapy trial offers a compelling model for global health equity, further multi-center genomic and pharmacokinetic validating data are required to confirm if these results can be generalized across diverse patient populations with different mutational burdens. Additionally, the exact molecular pathways by which exercise mitigates colon cancer recurrence (e.g., insulin-like growth factor [IGF] signaling pathways, systemic inflammation reduction) remain an active area of biomarker exploration.
I agree that this could be worth doing, perhaps once during adulthood. However, to my understanding, it’s relatively difficult to become infected, especially in the Western world. For the record, I did the breath test recently and it was all-clear, and I also did gastroscopy which showed absolutely nothing, so I’ve basically ruled out stomach or oesophageal cancer for a while now, which is nice.
Hey Beth, I am not an oncologist or cancer specialist at all, but my first question would be - are these full-body (or torso) scans actually detailed enough to be able to reliably measure the difference between 4mm and 8mm? That’s a genuine question. In my experience (mostly with ultrasound and CT, not MRI) there is some subjectivity when it comes to how you select the area for measurement, and slight differences in your position, scanner alignment etc can change the measurement. For one of these broader screening-type scans, the level of resolution means that 4mm could be literally just a few pixels on the screen. Obviously a targeted scan of the pancreas using the proper contrast agents would be the answer. However, I’d also seek some specialist advice about whether that is actually worth doing - i.e. whether it actually gives you meaningful, actionable information.
To my knowledge, most of us have some sorts of weird benign growths, cysts etc. I have a ~1cm one in my kidney, which was randomly discovered during an abdominal ultrasound. I think the more you look for things, the more you’ll find, and the vast majority are harmless.
To my understanding, there are a couple of peaks during life. Certain cancers are tragically more common in childhood (some brain tumours, leukemias etc). There’s another peak in the 40-50s. And I think once you get to 80, there seems to be less, which is what your factoids also show. I suspect that if people really do manage to live for very long times, cancer will eventually catch them. As we know, lots of people have indolent cancers found during autopsy which wasn’t necessarily the cause of death.
Let’s take this opportunity to remind everybody to do some basic home checks. I try to do this every ~3 months or so. It’s a 10 minute job.
Ladies: check your breasts, including chest wall, and armpits.
Men: check your testicles. Roll each one carefully between your fingers. You’re looking for anything which feels asymmetrical (in feel, size, weight), or like a hard stone inside a boiled egg.
Everybody: check your skin for lesions. Don’t forget bottoms of feet, between fingers and toes, your scalp, genitals, nail beds.
This type of screening really can work. My aunt found a stage 2 breast cancer through a manual exam. That was 5 years ago and she’s doing great now. (And actually, her routine mammogram was cancelled due to Covid, so if not for the manual check, it probably would have advanced to a deadly stage IMO).
Treating pancreatic tumours may have revealed cancer’s master switch
A promising drug could be the first of an entirely new class of treatments
Scientists are not usually an excitable bunch. So when many thousands of them recently gave a spontaneous standing ovation (with cheering) in the middle of a lecture, it meant something special happened. At a conference in Chicago at the end of May oncologists went wild over the results of a drug called daraxonrasib, which treats pancreatic cancer. The drug almost doubled median survival times from 6.7 months to 13.2 months. This victory over one of the most challenging cancers was an emotional moment for some.
The drug isn’t anything close to a cure. Cancers often develop resistance to targeted drugs such as daraxonrasib. The drug’s promise for patients is that, when used alongside other treatments, it might open the door to much longer survival times. Pancreatic cancers are aggressive and usually symptomless. They are usually diagnosed after they have already spread around the body. Few patients survive longer than a year, and this cancer had also turned out to be resistant to immunotherapy, a class of treatment that deploys the body’s immune system to fight tumours and which has been such a lifeline in many other cancers. The mutation in the kras protein, which drives most pancreatic cancers, creates an environment outside each tumour that is hostile to immune cells.
The drug is expected to speed its way through approval in America. Eventually it seems likely to be given as a first-line treatment—rather than to those who have already tried chemotherapy, as was the case in the trial. The drug works by inhibiting kras. Other work suggests this also changes the environment around the tumour in ways that mean the tumour may respond to immunotherapy. If this approach is successful, it could further improve survival times.
Yeah, this is cool. Though this doesn’t sound like much, KRAS was always called an “un-druggable target”. Now they’ve proven that it can be done, so hopefully more will follow quickly.
A colleague of mine is an oncologist, and he’s absolutely thrilled with this. He said they’ll likely be using it as first-line, in combination with other chemo, basically hoping to smash as much potential resistance as possible.