He Was Expected to Get Alzheimer’s 25 Years Ago. Why Hasn’t He?
Scientists are searching for the secret in Doug Whitney’s biology that has protected him from dementia, hoping it could lead to ways to treat or prevent Alzheimer’s for many other people.
For 14 years now, Mr. Whitney has been the one-person focus of exceptionally detailed scientific investigation, for which he travels periodically to St. Louis from his home in Port Orchard, Wash. It is not because he is ill. It is because he was supposed to be ill.
Mr. Whitney, 76, is a scientific unicorn with potential to provide answers about one of the world’s most devastating diseases. He has a rare genetic mutation that essentially guaranteed he would develop Alzheimer’s disease in his late 40s or early 50s and would likely die within a decade.
His mother and nine of her 13 siblings developed Alzheimer’s and died in the prime of their lives. So did his oldest brother, and other relatives going back generations. It is the largest family in the United States known to have an Alzheimer’s-causing mutation.
“Nobody in history had ever dodged that bullet,” Mr. Whitney said.
But somehow, he has done just that. Something has shielded him from his genetic destiny, allowing him to escape Alzheimer’s for at least 25 years longer than anyone expected.
Rapid amyloid-β clearance and cognitive recovery through multivalent modulation of blood–brain barrier transport -Nature 2025
They built “supramolecular” nanoparticles that mimic the ligands of the BBB receptor LRP1. After IV injection in AD mice, the particles restored BBB transport and triggered the brain’s own clearance pathway. Within ~1 hour, brain amyloid-β dropped by ~50–60%, with longer-term behavioral recovery reported in follow-ups. The key point is that the nanoparticles are bioactive (drug-like)—not mere carriers—and they re-establish BBB function, which then clears plaque. It also rapidly lowered albuminuria.
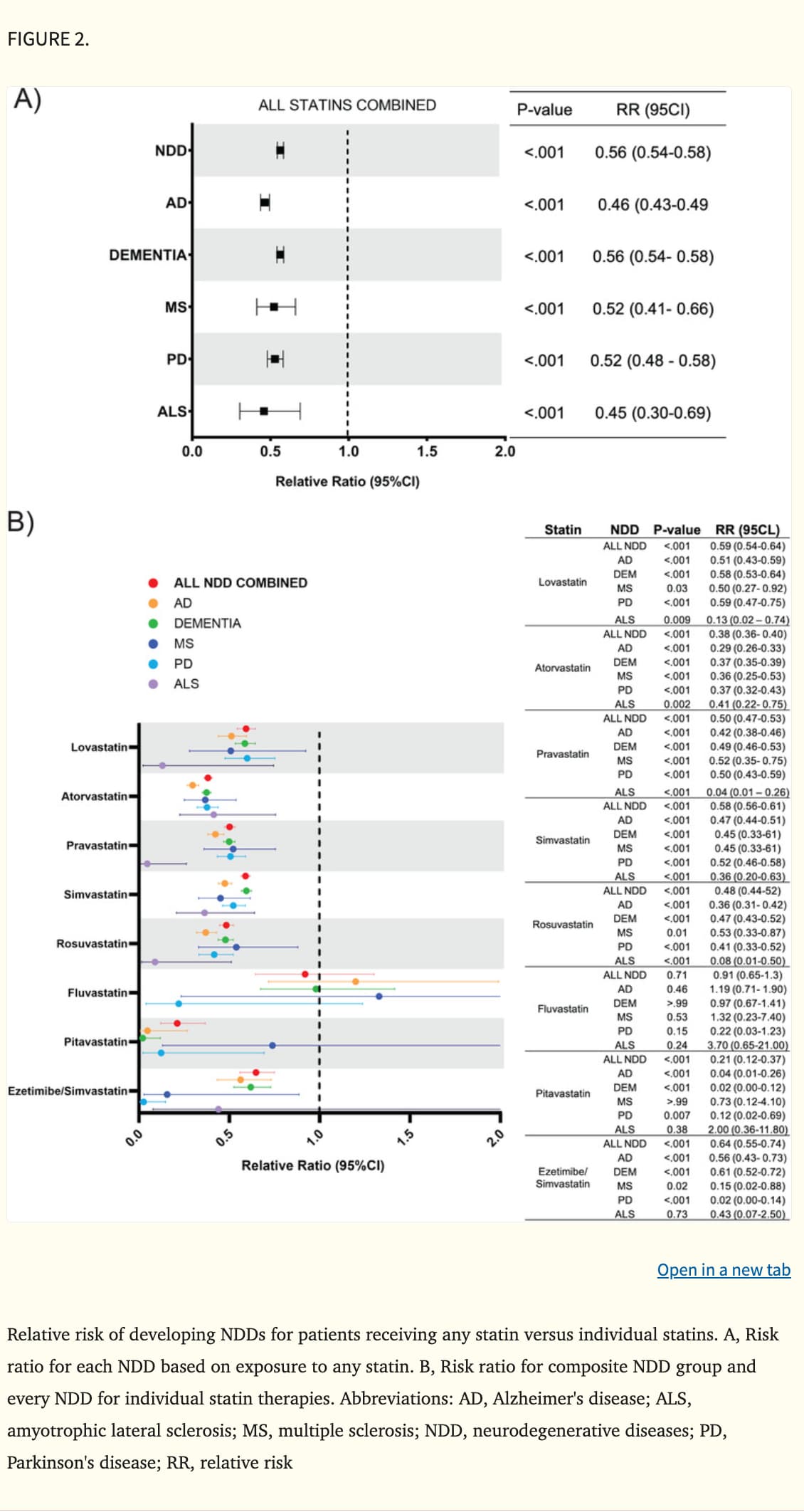
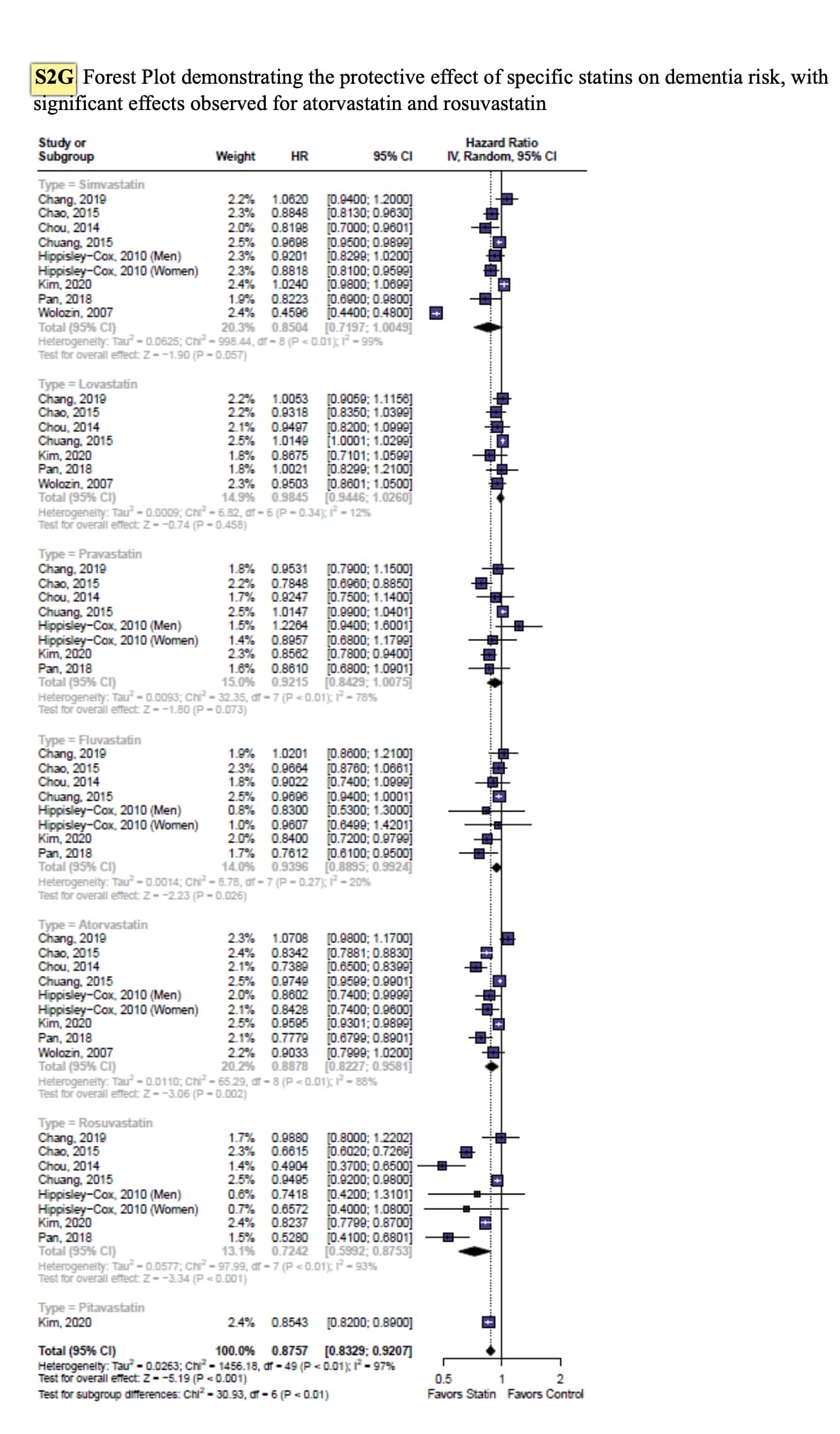
In contrast, this study found no statistically significant benefit for pitavastatin and concluded that rosuvastatin performs best. Unfortunately, it doesn’t report the odds ratio or confidence interval for pitavastatin.
"Additionally, rosuvastatin demonstrated the most pronounced protective effect for all‐cause dementia among specific statins (HR 0.72; 95% CI: 0.60 to 0.88). "
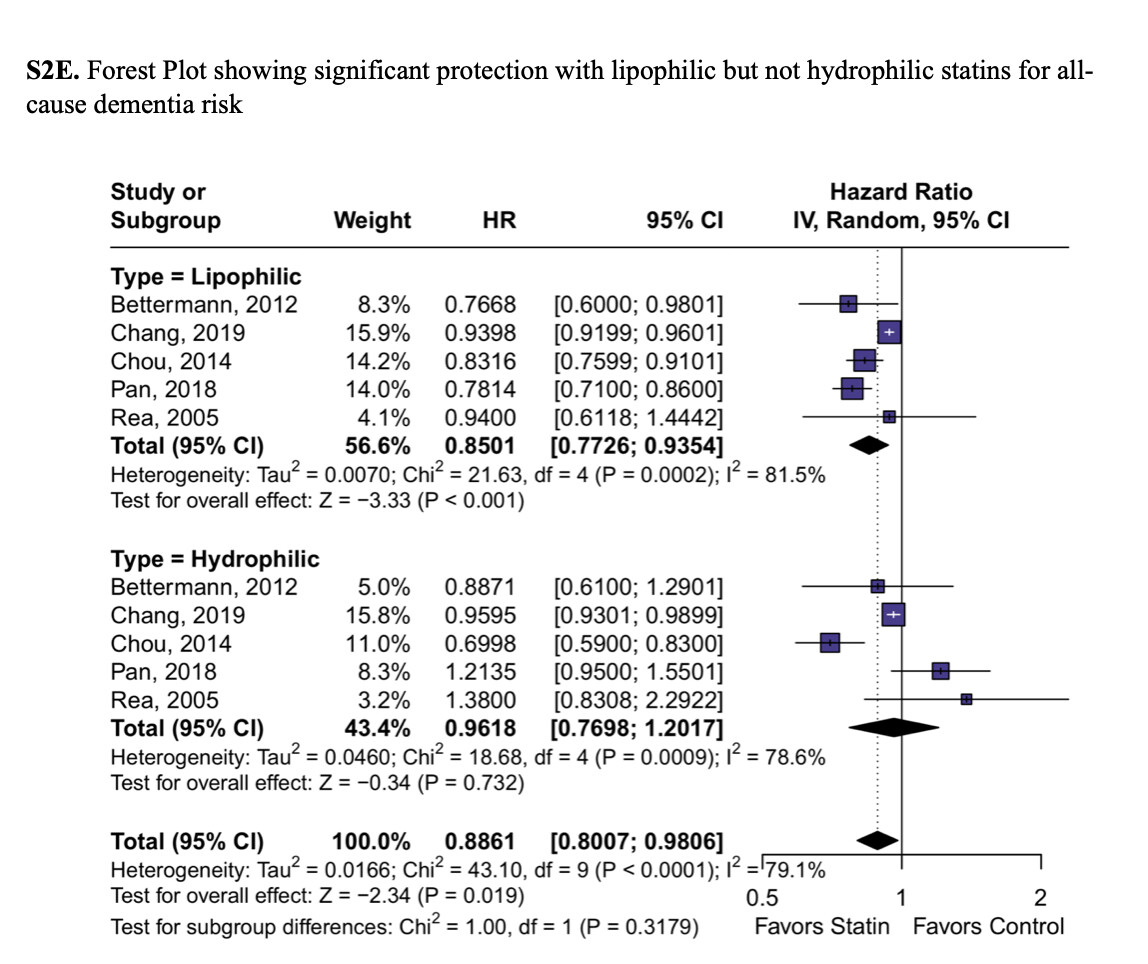
They also looked into hydrophilic vs lipophilic statins:
For AD specifically, both hydrophilic (17% reduction) and lipophilic (15% reduction) statins showed significant effects.
Cholesterol-lowering drug targets reduce risk of dementia: Mendelian randomization and meta-analyses of 1 million individuals
INTRODUCTION
We tested whether genetically proxied non-high-density lipoprotein cholesterol (non-HDL-C)–lowering drug targets reduce risk of all-cause dementia.
DISCUSSION
Genetic lowering of non-HDL cholesterol via HMGCR, NPC1L1, and CETP reduces the risk of dementia. This reflects the effect of lifelong differences in non-HDL cholesterol on risk of dementia.
Highlights
Variants in HMGCR, NPC1L1, and CETP reduce the risk of dementia via non-high-density lipoprotein cholesterol (non-HDL-C).
An effect of PCSK9, ANGPTL4, and LPL variants on dementia risk cannot be excluded.
This reflects the effect of lifelong lower non-HDL-C on risk of dementia.
RapAdmin, I’m going out on a limb here to give an opinion from a non-medical person about this article. My thought is that damaged capillaries in the brain lead to reduced blood flow with resulting reductions in incoming nutrients and outgoing contaminants. This results in a poorly functioning brain with a buildup of plaques.
Damaged capillaries can be caused by too much sugar (glucose) in the blood. Whether it’s just high blood sugar in general or technically classified as diabetes, controlling blood sugar levels is one of my major concerns for maintaining brain health.
I’ll leave it up to the experts to correct any of my errors.
So the first dataset suggests rosuvastatin is the most protective and the second suggests that hydrophilic statins are not protective? Isn’t that inconsistent?
No amount of alcohol is safe, at least for dementia risk, study finds (WaPo)
Even a drink or two a day isn’t risk-free, a new study suggests.
For years, the common wisdom and science was that a little bit of alcohol wasn’t bad — and even beneficial — for your health: A toast to moderation.
But new research published in BMJ Evidence-Based Medicine suggests that even light alcohol consumption can increase dementia risk.
The finding comes from data of more than 550,000 adults ages 56 to 72, as well as genetics information from 2.4 million study participants. It adds to evidence that even small amounts of alcohol can be harmful to our health, including increasing the risk of cancer or disrupting sleep.
Excessive alcohol consumption — more than 12 drinks per week — and alcohol use disorder have long been linked to dementia, an umbrella term for different types of progressive cognitive impairment, including Alzheimer’s disease.
Alcohol use and risk of dementia in diverse populations: evidence from cohort, case–control and Mendelian randomisation approaches
Conclusions These findings provide evidence for a relationship between all types of alcohol use and increased dementia risk. While correlational observational data suggested a protective effect of light drinking, this could be in part attributable to reduced drinking seen in early dementia; genetic analyses did not support any protective effect, suggesting that any level of alcohol consumption may contribute to dementia risk. Public health strategies that reduce the prevalence of alcohol use disorder could potentially lower the incidence of dementia by up to 16%.
As your youth fades further into the past, you may start to fear growing older.
But research my colleague and I have recently published in the journal Intelligence shows there’s also very good reason to be excited: for many of us, overall psychological functioning actually peaks between ages 55 and 60.
And knowing this highlights why people in this age range may be at their best for complex problem-solving and leadership in the workforce.
Research Paper (Open access):
Humans peak in midlife: A combined cognitive and personality trait perspective
Highlights
Age trends reviewed across 16 key cognitive and personality-related dimensions.
All variables plotted on a common scale to enable direct cross-domain comparisons.
Age trajectories varied widely: some traits declined, others improved with age.
A weighted composite index of functioning was developed from theory and evidence.
Overall cognitive-personality functioning peaks between ages 55 and 60.
Ah. It’s great to recognize that midlife is now 55-60. In my grandparents’ day, that was the twilight years, as most died in their 70s. Now we’re pushing into the mid-80s and even 90s.
It feels like we really have gained a decade or two of healthy life beyond what our grandparents and their forbears had!
I know I’m going to sound greedy, but even that seems like not enough though!
Blood tests are now approved for Alzheimer’s: how accurate are they? (Nature)
A second blood test has been been approved by the US Food and Drug Administration to assist in diagnosing Alzheimer’s disease. Will these tests change how cognitive decline is measured?
A new blood test to aid with the diagnosis of Alzheimer’s disease has been approved by the US Food and Drug Administration (FDA). The test, which is designed to rule out cognitive decline caused by Alzheimer’s disease, is the first blood test cleared for use in primary-care settings but not a first for Alzheimer’s.
Elecsys pTau181 — developed by two pharmaceutical companies, Roche in Basel, Switzerland and Eli Lilly in Indianapolis, Indiana — measures a specific phosphorylated form of tau, known as pTau181 in blood plasma. The test quantifies how much tau protein in the body has been modified as a result of Alzheimer’s disease.
In a press release on 13 October, Roche reported that in a clinical trial of 312 participants, the Elecsys pTau181 test was correctly able to rule out Alzheimer’s 97.9% of the time. The test uses a negative predictive value and helps to rule out Alzheimer’s in individuals with cognitive decline, rather than giving a positive indication that someone has the disease.
Comparative Effects of SGLT2 Inhibitors and Incretin-Based Therapies on Dementia Risk in Type 2 Diabetes: A Systematic Review and Meta-analysis
Conclusion: SGLT2is may provide neuroprotective benefits beyond glycemic control in patients with T2D, particularly in older populations at higher risk of cognitive decline. These findings support consideration of SGLT2is as a preferred therapeutic option for patients with T2D at increased risk of dementia, although randomized controlled trials would further strengthen this evidence base.