@DrFraser I am statin intolerant (at least for Rosuvastatin) and I am currently taking Bempedoic Acid. I haven’t gotten my bloodwork done yet because I want to trial BA for 3 months to get a feel for how it is affecting my LDL and ApoB. Do you think there is a great benefit to trialing a different statin over BA? Cost is not a factor for me as BA is as cheap as statins when bought from India. Thank you.
2 Likes
I won’t give anyone personalized medical advice on this forum, but I can give some general context and information.
In general when I start people on statins, I utilize Atorvastatin most times, and go with 10 mg every other day, and if tolerated x 2 weeks then either go to daily or 20 mg every other day. Many who have intolerance do better with alternate day dosing.
Much of the benefit of most drugs occurs at their lower range of dosing, and as we push doses up the benefits are smaller and risk of side effects go up. I personally do 20 mg of Atorvastatin every other day and 5 mg of Ezetimibe daily. There is a nice trial showing 5 mg of ezetimibe essentially gets same result as 10 mg.
With using 2 agents in super low doses, unlikely to cause side effects in most people, ApoB drop by 40 pts in me.
Cheap, easy, well tolerated by most people.
I take the same approach with blood pressure, with many of my patients on 4 meds, but tiny doses, way better tolerated and more effective than 2 meds pushed to maximum doses which generally results in a high frequency of side effects.
I’d not going to other agents as first line therapy for my patients.
Your situation might differ, but hopefully this general context of how I approach this topic with my patients is helpful.
8 Likes
Thanks. I originally tried Rosuvastatin at 5 mg every other day and the muscle soreness was unbearable. That’s why I took Dr. Attias advice and tried Bempedoic Acid which hasn’t caused any side effects. Ezetemibe at 10 mg actually had positive side effects (energy boost). I guess I’ll just wait for the next blood work results and then go from there. Sometimes you just need the hard data to see what’s happening.
2 Likes
It sounds like you are completely on top of everything and doing your own management. You might well not tolerate statins by the sounds of things.
For most patients a check of a comprehensive metabolic panel, lipid panel and apoB at 3 months post any medication change is pretty reasonable - and you’ve indicated that is your plan … this is as long as there are no adverse reactions.
The study on ezetimibe 5mg being as effective as 10 mg is here:
Ultimately getting one’s ApoB into the 50-70 range is a goal, and holding it there for life, and starting as early as possible to avoid cumulative vascular disease.
I have seen some posts of individuals getting serial coronary artery calcium scores and following those. I know of no scientific evidence of that being a sensible plan. Getting that study once might be sensible, as a normal score CAC=0 is reassuring, but doesn’t change the need to optimize ApoB. If you have an elevated CAC then I think this can be used as a motivator for someone who isn’t taking their vascular risk seriously, to realize they need to stop ignoring it. But the outcome is the same - manage the ApoB and other vascular disease risks tightly.
We know that doing heart caths on these individuals happens a lot, which there is no evidence for (unless there are symptoms of an unstable cardiac issue) and know that tight management of vascular risks is at least a good as these invasive approaches that have risks and costs, and no proven benefit - on my reading of the literature.
10 Likes
There is zero reason not to take the full dose of ezetimibe other than perhaps cost.
2 Likes
Hmm …
Taking a higher dose of anything increases rate of side effects, and Ezetimibe has significant side effects that occasionally occur. Why take more of something and raise your risk of side effects with absolutely no clear better outcome in the measure of the item you are trying to treat (in the case of that article LDL)?
Here are the potential adverse reactions to Ezetimibe:
https://www.mayoclinic.org/drugs-supplements/ezetimibe-oral-route/side-effects/drg-20067172
Less is more when it comes to medication. Once there is trivial to no benefit and only risk of increased adverse outcome … I’d disagree with the “zero reason.”
7 Likes
Conclusions Ezetimibe results in little to no difference in adverse events or other undesirable effects compared with placebo, usual care or other lipid-lowering agents.
Based on that meta-analysis (and other studies), ezetimibe is likely the safeat out of all apoB lowering medications.
2 Likes
What’s the thought process for preferring to start with atorvastatin over other statins?
1 Like
I prefer atorvastatin because at high dose 80 mg is almost equivalent to Rosuvastatin 40 mg and in early trials we saw excess (comparatively) type 2 diabetes develop in Rosuvastatin vs. Atorvastatin.
Regards,
Grant
5 Likes
5 Likes
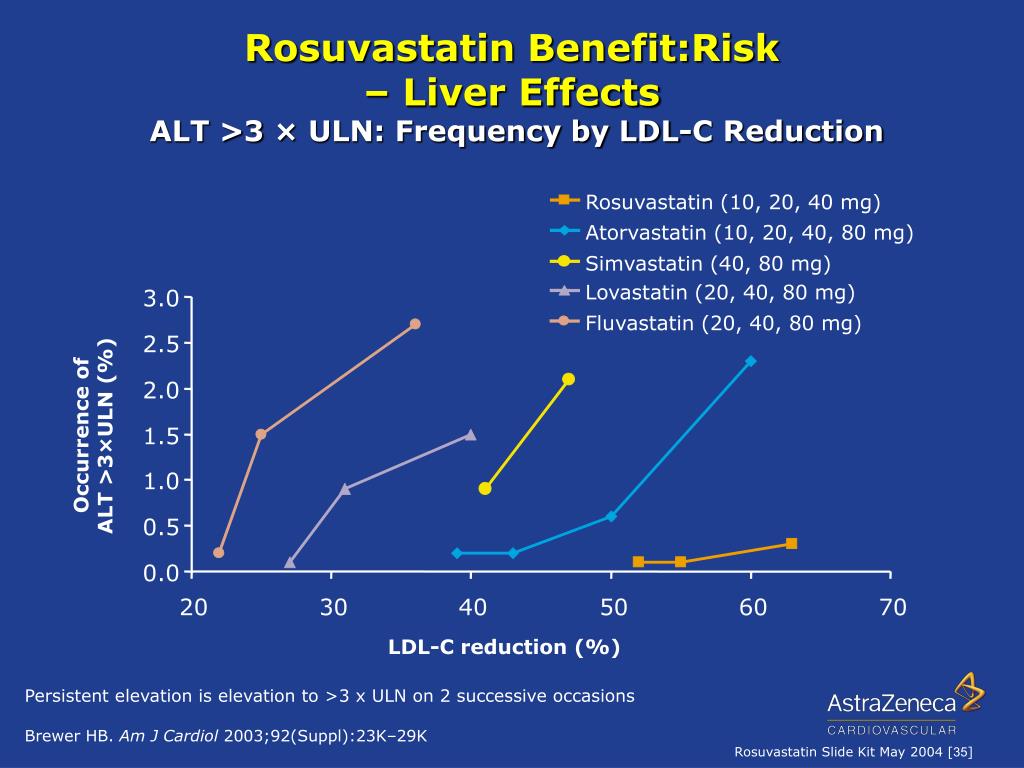
I must say that I rarely go beyond 20 mg daily, but beyond that, there are 2 points. First it is a tiny % irrespective that get this. Second is a transaminase rise is not liver damage. It is something we occasionally check and if 2-3 times upper limit of normal when previously normal, this is an indication for change in agent or dosing with many medications. Actually seeing “damage” in any measurable way from statins, I’ve seen zero cases in 29 years as a doctor. Not that it hasn’t ever occurred, but remarkably rare
5 Likes
there are many articles over the past 10 years which demonstrate poor to no efficacy for statins. The cholesterol hypothesis is proving untrue.
News Health
UK World Scotland Education
the basis for statins] were predicting we may see the end of heart disease by the beginning of the 21st century.
“But we haven’t - it is still the single biggest killer of both and men and women worldwide with 18 million deaths a year - so I began my own investigations.”
Dr Malhotra’s new book, A Statin-Free Life: A revolutionary life plan for tackling heart disease - without the use of statins, is the end result. The central argument is that the pills - the most commonly prescribed drug in the UK, with around seven million people taking them - are given out far too quickly in many cases, often causing unhelpful side effects, when a focus should be on specific lifestyle changes instead. It is advice he gives his own patients and follows himself.
"Lowering cholesterol needs to be relegated to 1 division four of the league of tackling heart disease, because for 99 per cent of the population total levels of cholesterol, and so-called ‘bad’ LDL cholesterol, has almost no value at all in predicting whether or not someone is going to
1 Like
Looks like more in the 5 mg group were getting high intensity statin; titrating to effect will be key with this strategy,
This is so wrong that it’s pointless to argue against as it’s clear you have done no research outside of your bubble. Start by listening to podcasts with Thomas Dayspring, Allan Sniderman, Peter Attia, etc. Then look at the articles written by them. Then the research papers they’ve either written or cite.
5 Likes
I think its best to ignore articles and focus on the research. The research is fairly conclusive now that statins improve cvd risk at a population level.
Where Dr Malhotra seems to have a blind spot, is that he is only focussed on 10 year risk. Most people considering statins are interested in living considerably longer than that. But even with only a 10 year time horizon the benefits are clear: “NICE estimates that under this new recommendation, on average, for every 1,000 people with a risk of 5% over the next 10 years who take a statin, about 20 people will not get heart disease or have a stroke because they take a statin. This figure doubles to 40 for people with a risk of 10%, and for people with a risk of 20% NICE estimates that, on average, around 70 people would not get heart disease or have a stroke in the next 10 years.”
Statins could be a choice for more people to reduce their risk of heart attacks and strokes, says NICE | News | News | NICE.
The other area where Dr Malhotra seems off base are the side effect risks. https://www.bmj.com/about-bmj/independent-statins-review-panel
Where i think most people can agree is that exercise, high fibre diet, and oily fish all improve blood lipids (apo-b) and cvd risk. And controlling blood sugar independently improves cvd risk.
6 Likes
Imo it is because of books like those that heart disease has not been eliminated yet.
2 Likes
Can you explain to me what you consider adequate efficacy?
Managing CAC score growth is a reasonable goal. Keeping annual growth to below 15% reduces risk of an cardiovascular event significantly. This true even when the starting CAC score is high.
1 Like
It’s simple: If you have CVD (positive Calcium score) lowering LDL reduces risk. If you don’t (CAC=0) it does not reduce risk. Why? Not clear, but some people tend to get CVD, and higher LDL increases the risk.
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.122.061010
That study had a follow up time of only 4.3 years.
So it’s worth qualifying “If you don’t (CAC=0) it does not reduce risk” in the near future
It’s also important to mention that a CAC score of zero doesn’t mean cardiovascular immortality.
In another study analyzing outcome data from the Multi-Ethnic Study of Atherosclerosis, investigators found that 10-year event rates for individuals between the ages of 55-64 with a CAC score of zero were 3.1% compared to 16.7% for people with a CAC score 300 or above. Ten-year association of coronary artery calcium with atherosclerotic cardiovascular disease (ASCVD) events: the multi-ethnic study of atherosclerosis (MESA) | European Heart Journal | Oxford Academic
3 Likes