All 11 TK inhibitors were inversely-associated with PD. Beneficiaries taking tyrosine kinase inhibitors targeting ERBb (Erlotinib, RR 0.51, CI 0.35–0.74), TEC (Ibrutinib, RR 0.60, CI 0.49–0.74), or PDGF, VEGF, FGFR, and/or SRC, i.e. Sorafenib (RR 0.48, CI 0.27–0.84), Imatinib (RR 0.59, CI 0.46–0.75), Pazopanib (RR 0.58, CI 0.39–0.88), Nintedanib (RR 0.67, CI 0.50–0.90), Sunitinib (RR 0.64, CI 0.41–1.00), and Dasatinib (RR 0.54, CI 0.35–0.83) tended to have the most marked inverse associations. The nrTKIs inhibiting JAK, i.e., Ruxolitinib (RR 0.81, CI 0.60–1.10) and Tofacitinib (RR 0.88, CI 0.68–1.14), exhibited more modest inverse associations, as did the ABL/PDGF inhibitor Nilotinib (RR 0.71, CI 0.47–1.09).
@DrFraser: might be worth an article on your blog (I still think there’s not enough data, but we’ll soon have the results of risvodetinib in PD and baricitinib and dasatinib in AD: Parkinson's disease - #341 by adssx )
Importantly, there was an 82% slowing in the total neuropsychiatric inventory (NPI) with particularly strong reduction in anxiety, hallucinations, and delusions in the CT1812 treated arms. In addition, there was a marked reduction in caregiver distress, which suggests a positive impact on the day-to-day lives of those receiving the drug. Participants treated with CT1812 experienced a slowing of decline across all three cognitive measures compared to placebo, including fluctuations in attention which declined by 91%.
Very impressive. Markets were positively surprised:
CT1812 is an experimental orally delivered small molecule oligomer antagonist that penetrates the blood-brain barrier and binds selectively to the sigma-2 (σ-2) receptor complex, which is involved in the regulation of key cellular processes. These processes are disrupted by toxic interaction with Aβ or α-synuclein oligomers, oxidative stress and other disease drivers. The ensuing damage to sensitive synapses can progress to a loss of synaptic function, which manifests as cognitive impairment and disease progression.
It’s also tested in Alzheimer’s disease and dry age-related macular degeneration.
The one I have the most access to (and have even taken myself) is Dasatinib, which taken short term (e.g. a few days) seems probably safe. But taken long term daily, I have concerns.
Do we know anything about the doses/duration they were looking at. Off shore, Dasatinib is cheap, and most folks are taking with Quercetin/Fisetin.
Melatonin is indeed a case where reverse causality is often present as most people only take it because they have bad sleep, hence the correlation. That said I would guess that it’s totally different for people megadosing for other reasons.
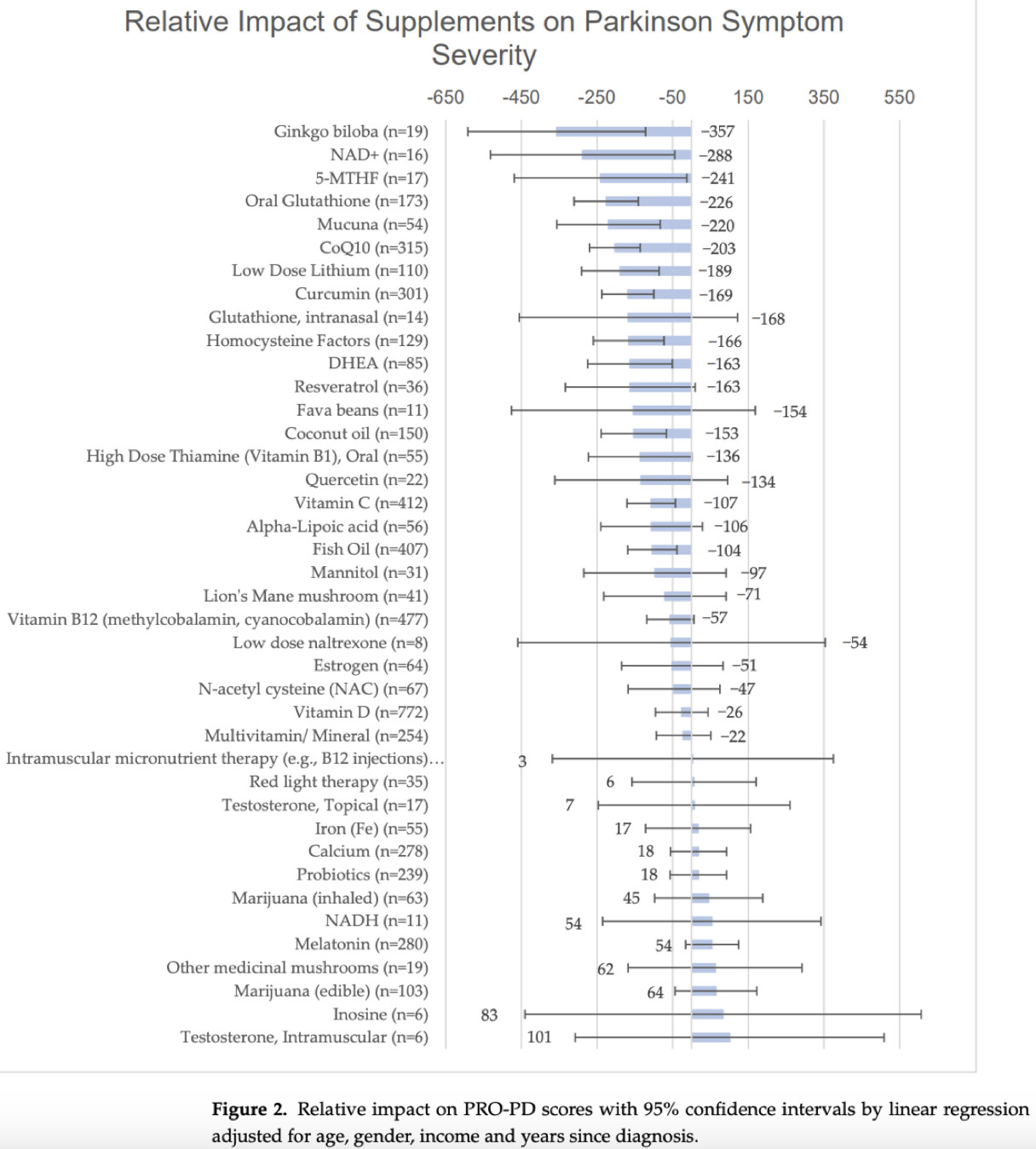
As I read it, only the error bar crosses the line for melatonin. Melatonin looks to have little or no effect.
What is more interesting to me is Gingko Biloba, which is known to increase blood circulation to the brain. From the list, if I were going to pick one supplement to ward off Parkinson’s, it would be Ginko Biloba.
You can also argue that all people with Parkinson’s have sleep issues to some extent and that those who take melatonin are those who take care of their sleep the most. (Playing the devil’s advocate here.)
From what I remember clinical trials of melatonin in PD improved sleep but not other symptoms. Not a great signal.
But with melatonin the dose + timing (before sleep? After waking up?) matter a lot. So… The jury is still out.
The number of users is too small to conclude anything. But as she said in the report: after these good results for Gingko Biloba we can expect many people with PD to start supplementing with it so in the next study in a few years we’ll have more data that could confirm or infirm the result.
Also, there’s not much data supporting Gingko Biloba in the literature for PD.
From the list I’m most surprised by oral glutathione VS NAC. There’s one good trial of NAC in PD and NAC is a rate limiting precursor of glutathione. So I would expect NAC to do as good as glutathione. And yet…
I think PD is a mitochondrial problem. Hence Yang Qi herbs should help. Having a combination of Yang Qi (AMPK activators) may be a synergistically positive approach.
Would there be an increased risk of heart attack/stroke with administration of exogenous PF4 in the non-surgical setting since it promotes coagulation?
PD-like pathogenesis induced by intestinal exposure to microplastics: An in vivo study of animal models to a public health survey
Hua Bai et al. J Hazard Mater. 2024.
Abstract
Highlights:
Chronic microplastics exposure damages the intestinal barrier and accelerates PD-like phenotypes in mice.
Microplastics facilitate neuroinflammation by triggering excessive ROS production and sustained UPRmt.
MPs detection and intestinal phenotypes are associated with a high frequency of disposable plastic use.
With the increasing incidence of non-hereditary Parkinson’s disease (PD), research into the involvement of specific environmental factors, in addition to aging, has become more prominent. The effects of microplastic exposure on public health have gained increased attention as it is known to cause a range of neurotoxic changes, some of which are similar to the pathological features of PD. We carried out low-dose microplastic exposure experiments on mice and Caenorhabditis elegans models and implemented a survey regarding the utilization of plastic products in the population. We found that low-dose microplastic exposure accelerated dopamine neuron degeneration and the onset of movement disorders in vivo, inducing a PD-like neuronal pathology through its effects on the intestinal mucosal barrier, immune barrier, and microbial barrier. Notably, non-penetrating microplastics facilitated neuroinflammation by triggering excessive reactive oxygen species production and a sustained UPRmt. Furthermore, our population survey demonstrated that inappropriate use was a major source of microplastics in the gastrointestinal tract. The high use of disposable plastic tableware, especially in those with definite microplastic exposure, was also associated with intestinal inflammatory symptoms. As a novel pollutant, microplastic exposure in vivo undoubtedly executes an important role in the degeneration of dopamine neurons, regardless of barrier penetration, which is a non-independent risk factor that cannot be ignored in the pathogenesis of PD. [PMID: 39397046]
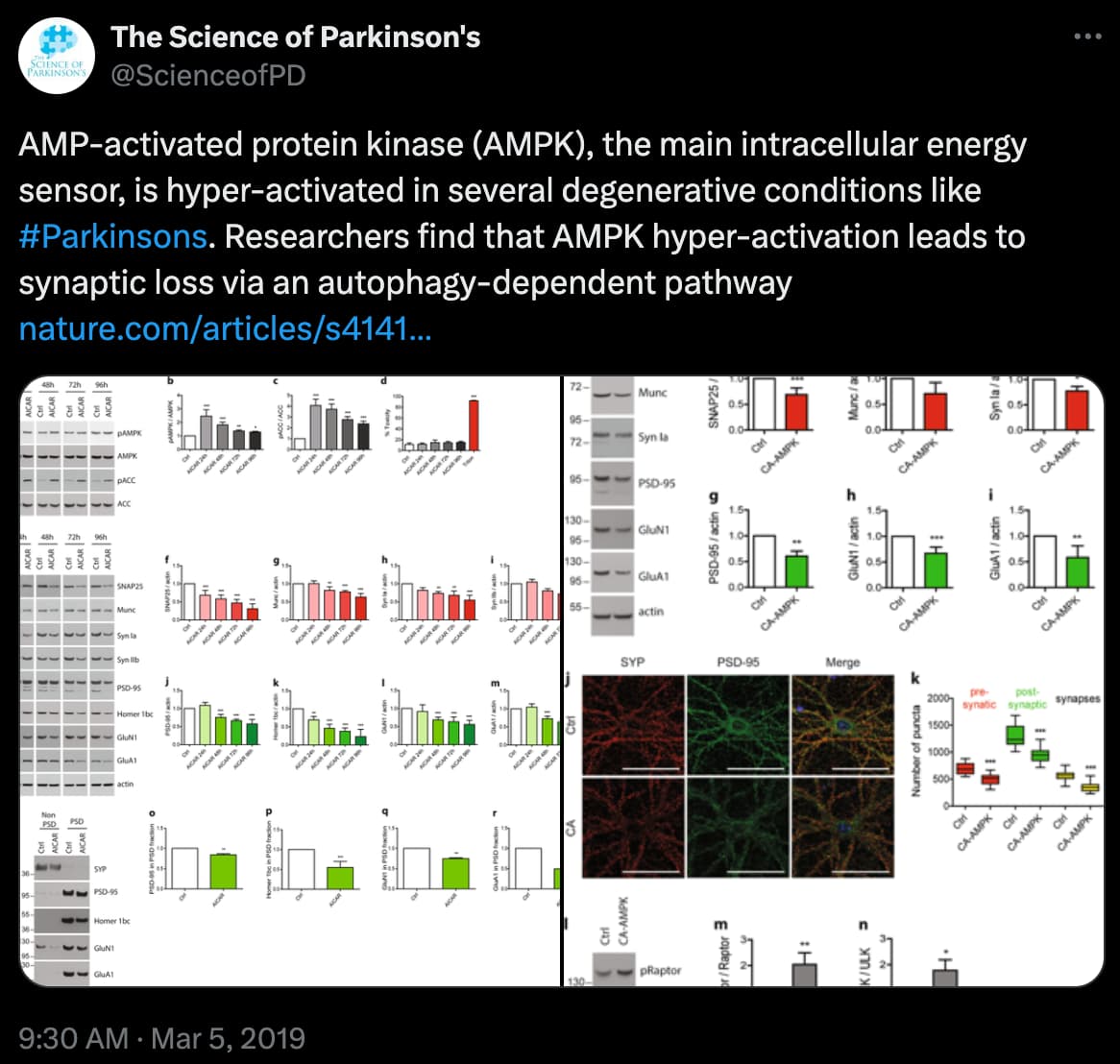
It may be that the cells already recognise they are short of energy and hence are activating AMPK, but for some reason or other are not getting enough from the mitochondria.
Right, But many things activate AMPK, so should they be avoided? For example exercise strongly activates AMPK - yet exercise shows benefits in PD, at least in the early stages of PD. I suspect JH is right, the problem might not be with activating AMPK, but downstream from AMPK, somehow the signalling doesn’t work. The increase in AMPK, might be a compensatory attempt, since the signal is not getting through. That might explain why exercise works in early PD, because there is still some signalling downstream from AMPK, and inreasing the levels through exercise helps with the inefficiency.
Medicare beneficiaries using the calcineurin inhibitor tacrolimus (RR 0.49, CI 0.40-0.60) and mTOR inhibitors everolimus (RR 0.38, CI 0.26-0.56) and sirolimus (RR 0.59, CI 0.37-0.93) had a lower risk of PD compared to those not taking the medication. The TNF inhibitor certolizumab was also associated with lower PD risk (RR 0.54, CI 0.34-0.84). Tacrolimus and everolimus remained significant after Bonferroni correction. Sensitivity analyses otherwise confirmed results for all four medications.