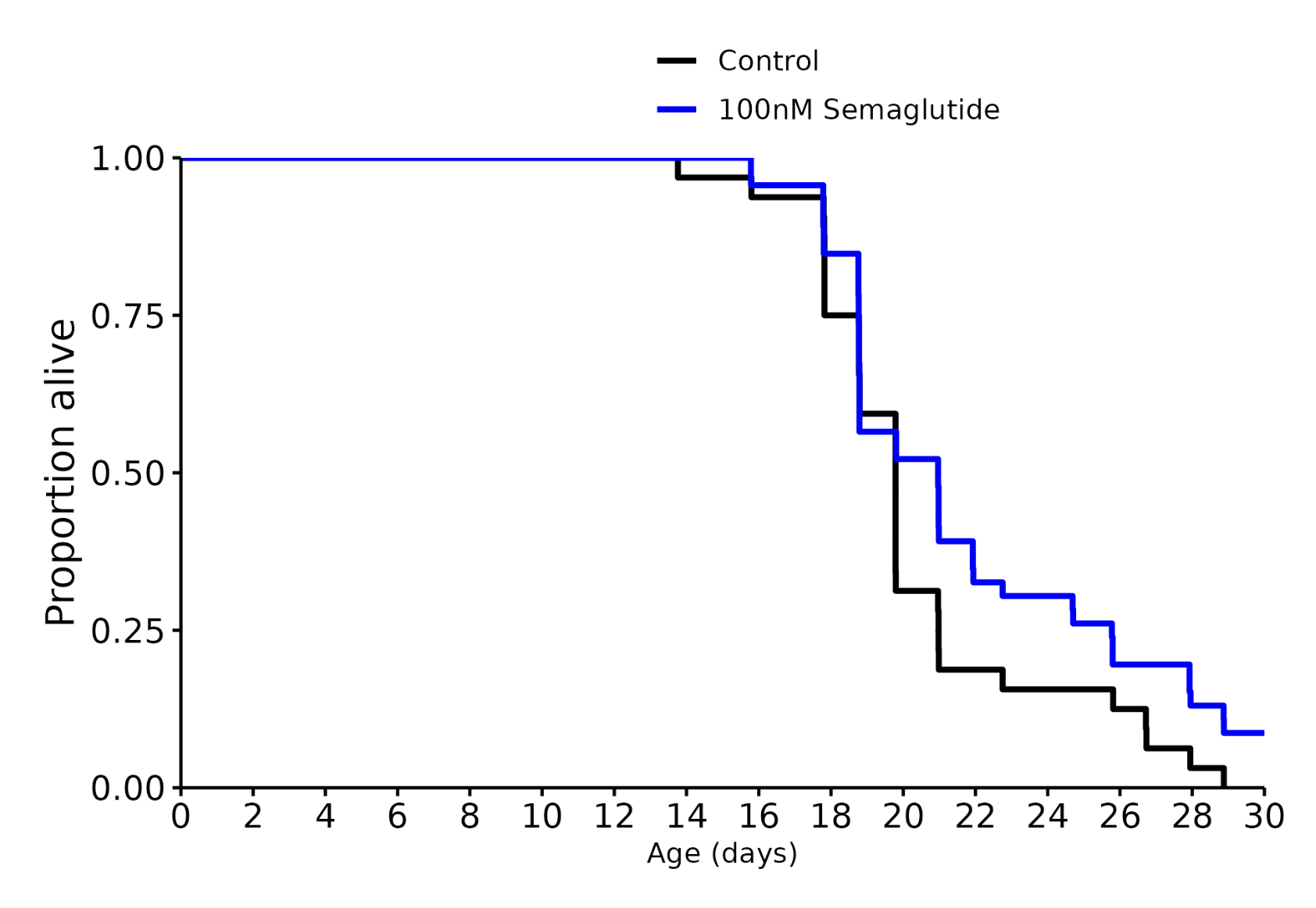
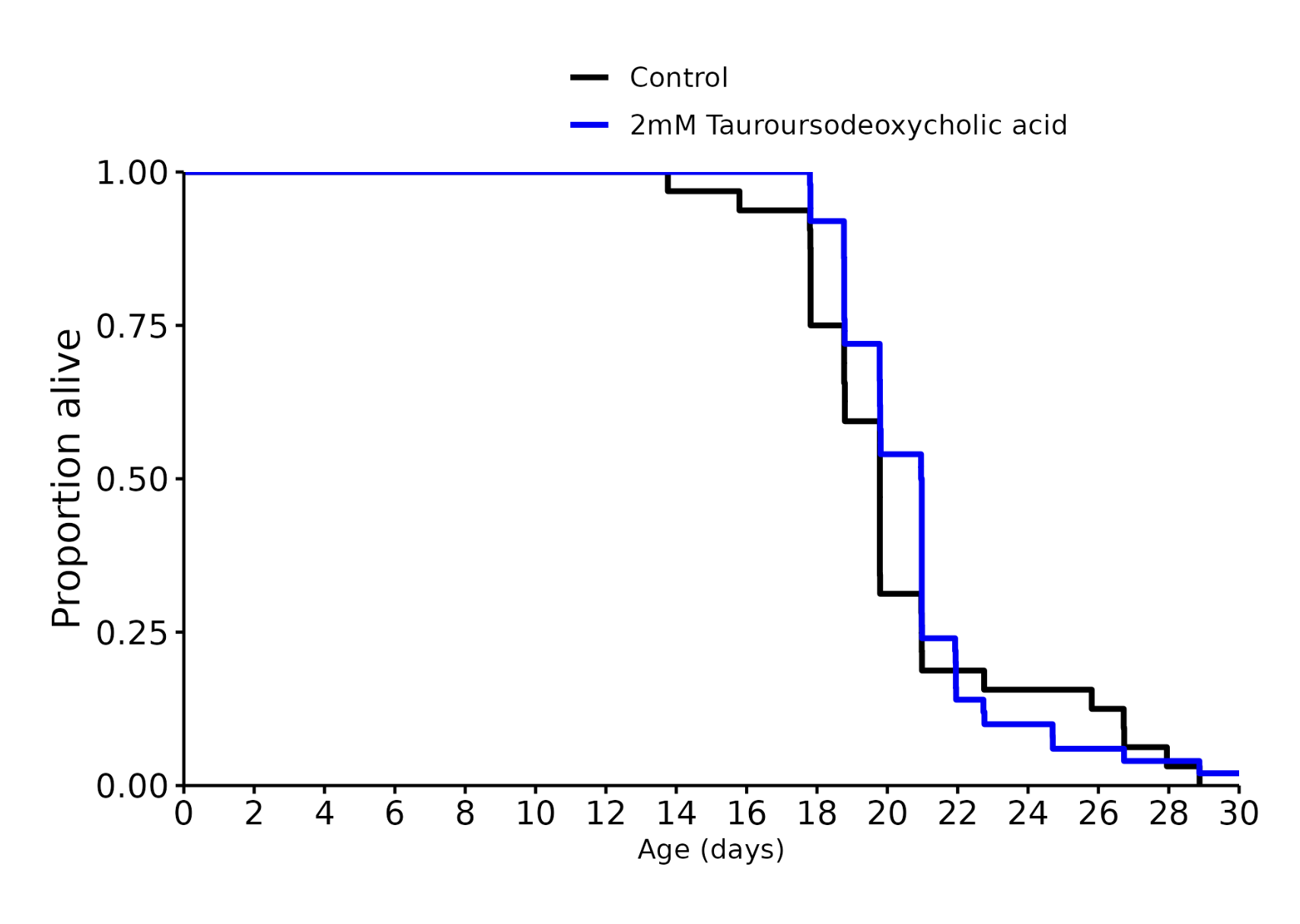
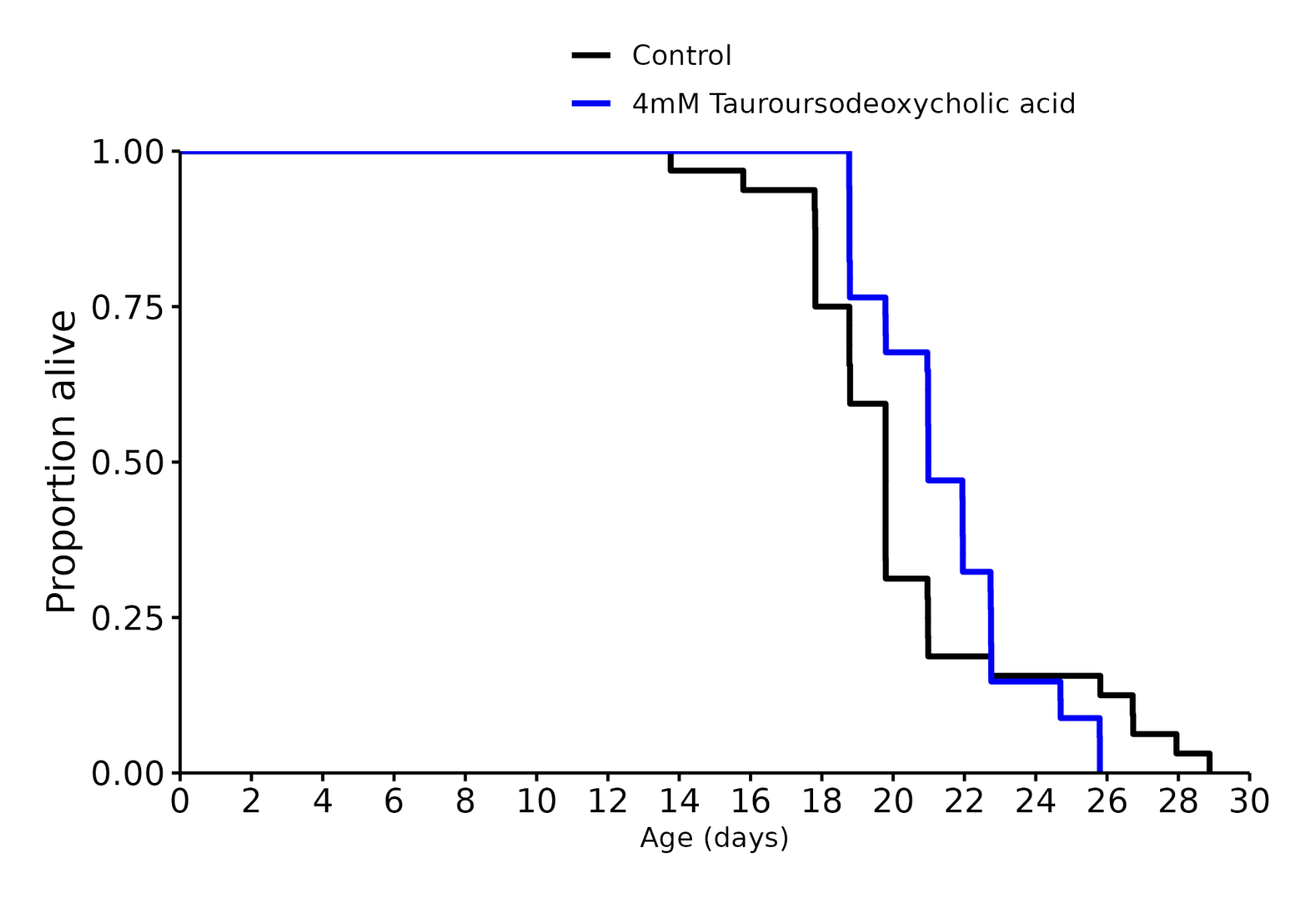
It’s interesting to see how the dose changes the trajectories.
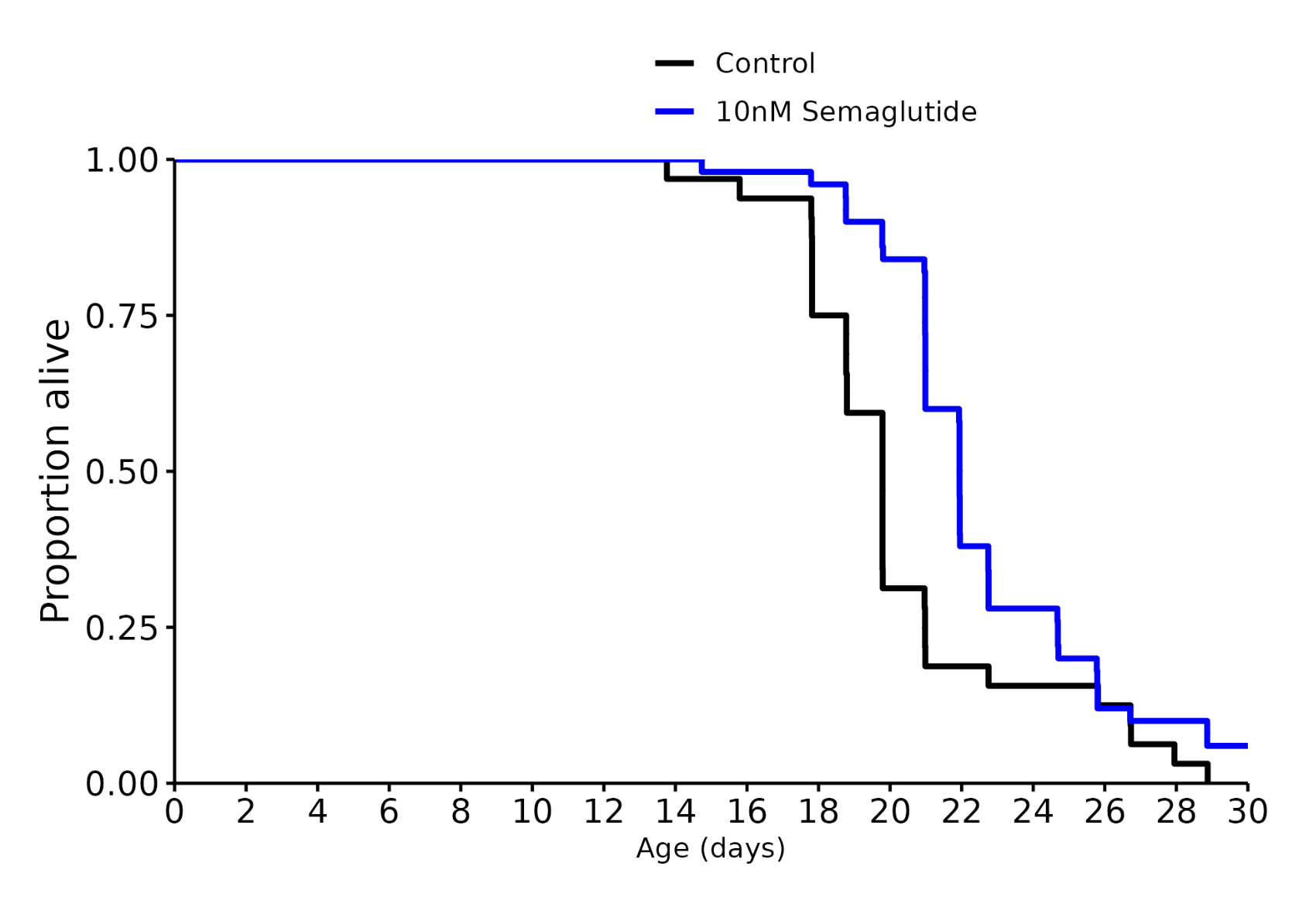
For instance for semaglutide the optimal for middle aged worms is 10nM but it is 100nM for the older ones.
In the similar way TUDCA is good for middle age but kill older worms faster.
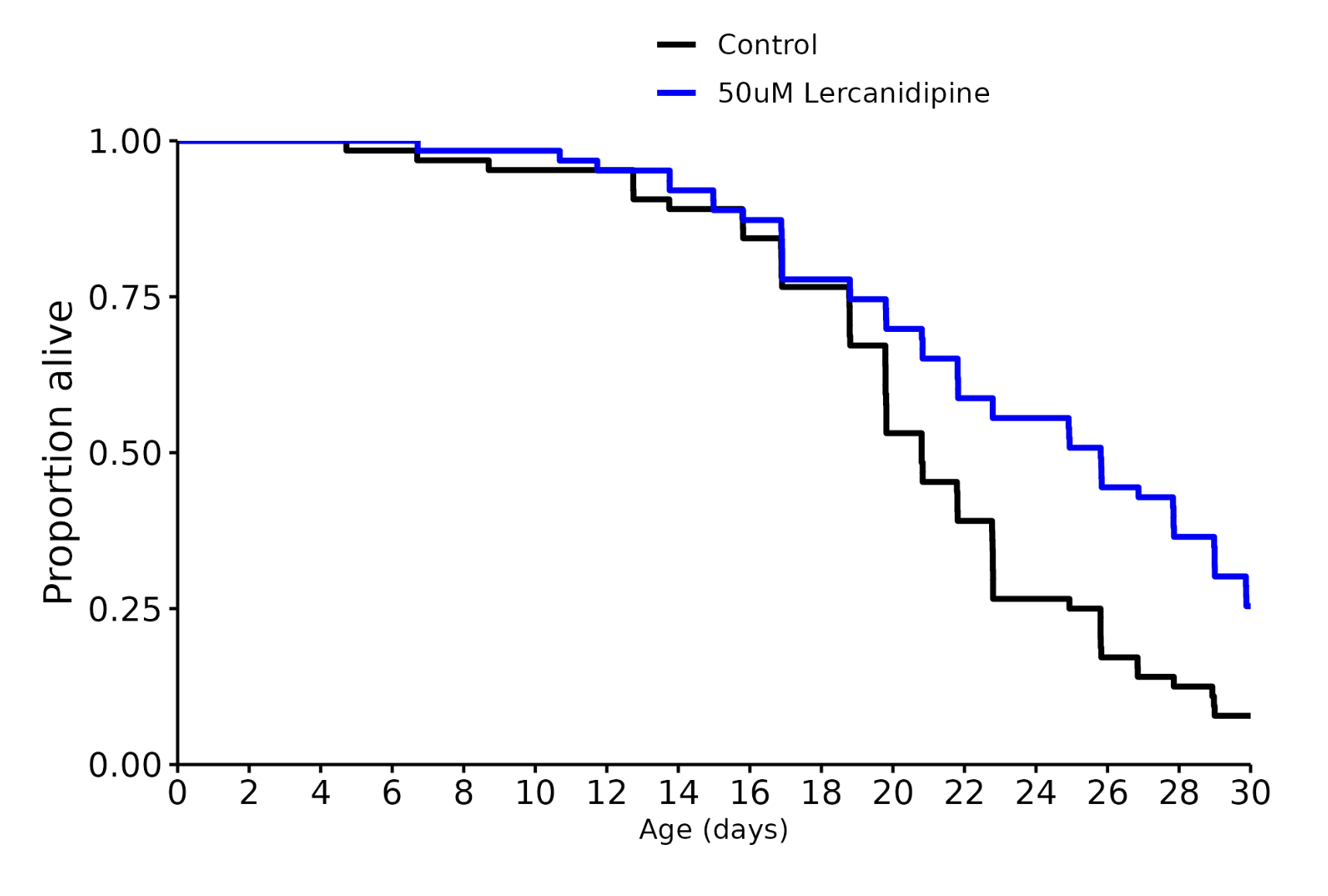
Thanks for sharing. Lercanidipine is interesting. Calcium channel blocker used for treating hypertension. But obviously the worms don’t have a heart or such a thing as blood pressure.
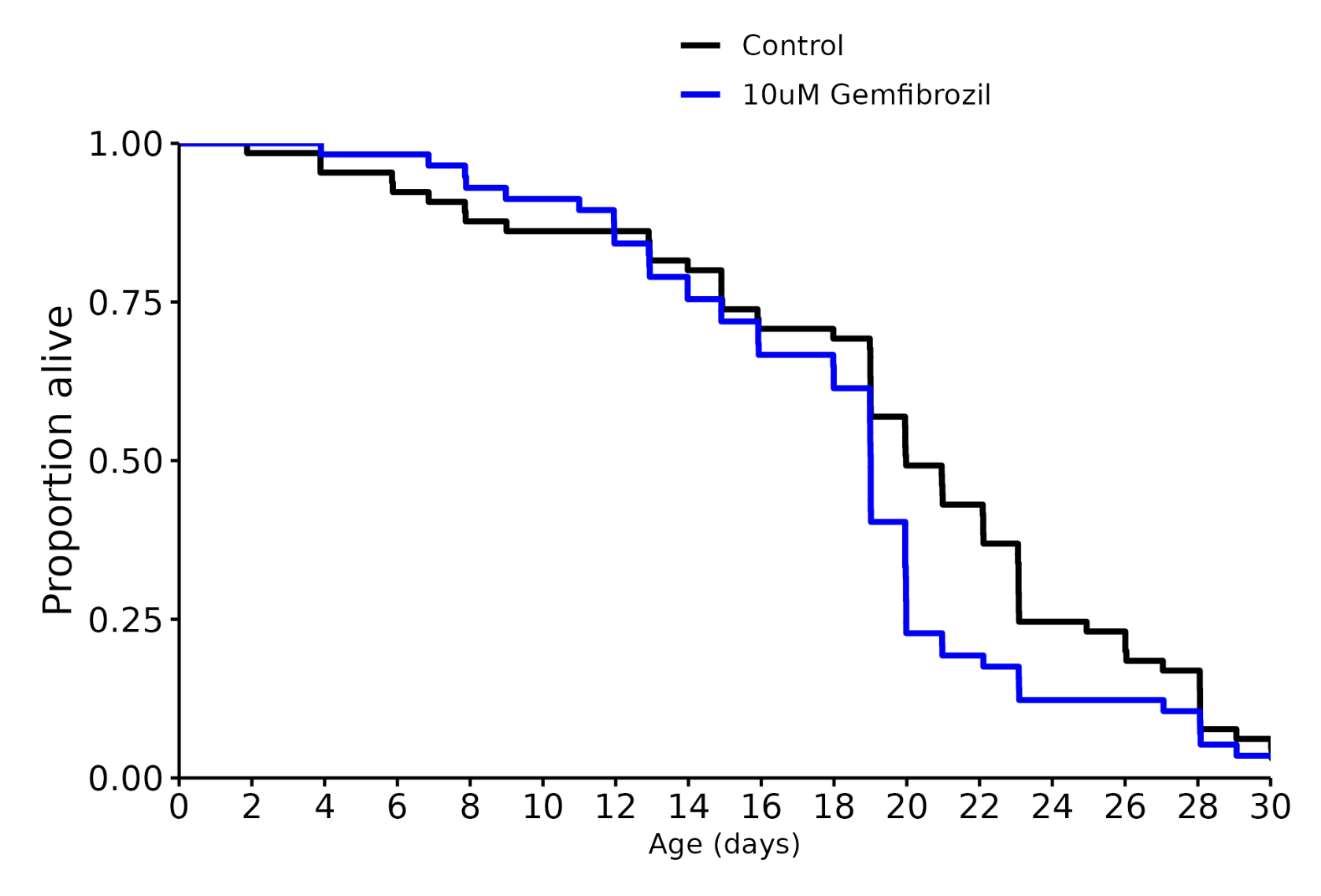
I don’t know how much you can interpret from it. To me, it looks like there is a lot of variability between each batch of worms. For example, controls for Gemfibrozil and Semaglutide have completely different survival curves. Semaglutide there are no control deaths until 14 days. For Gemfibrozil you have deaths starting almost immediately.
Personally I would only “value” this if the same thing can be replicated a couple of times in separate batches.
They also seem to re-use the same controls for the different doses of the same drug. I wonder if they account for that in the statistical analyses, because re-using the same controls changes the number of comparisons.
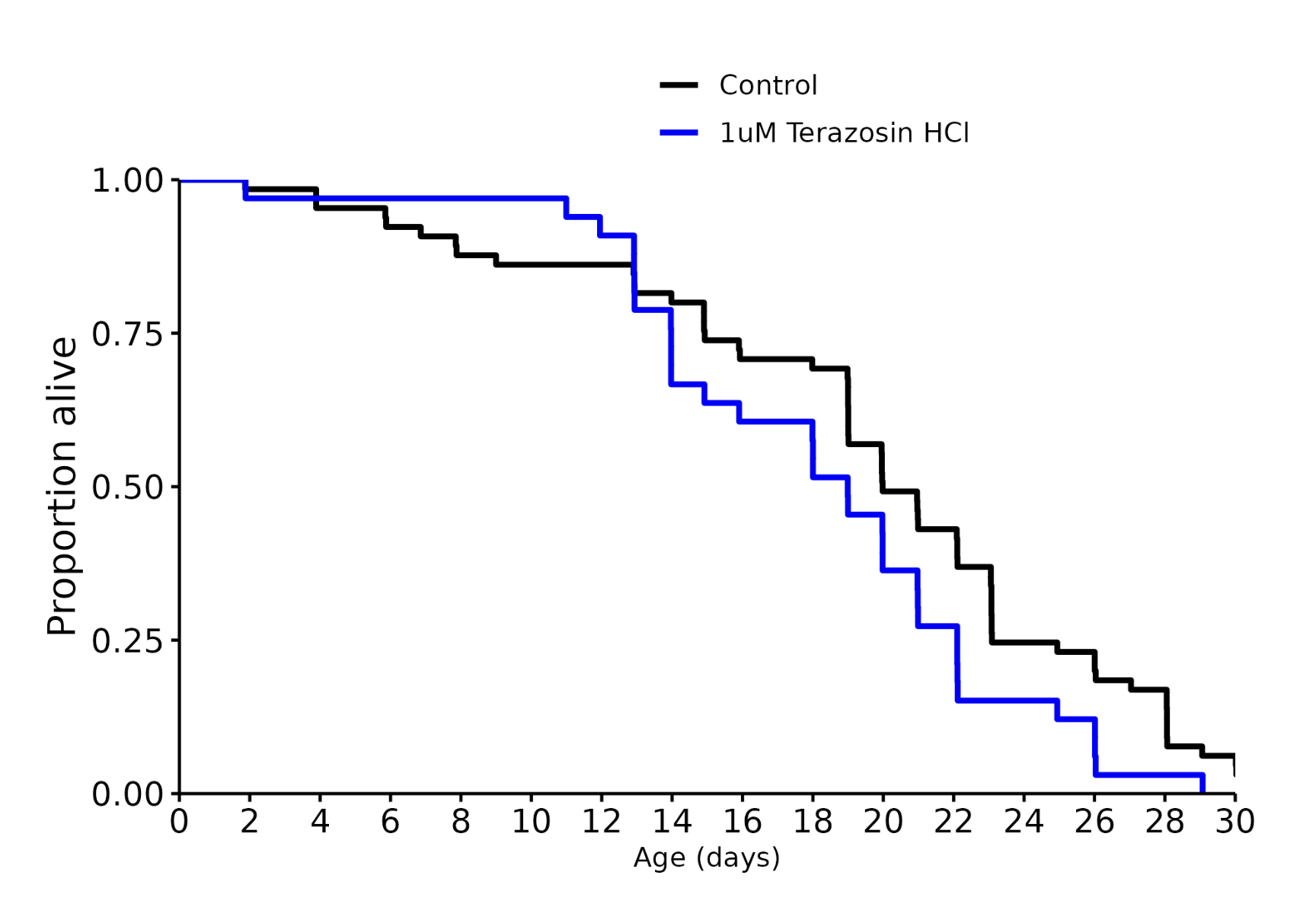
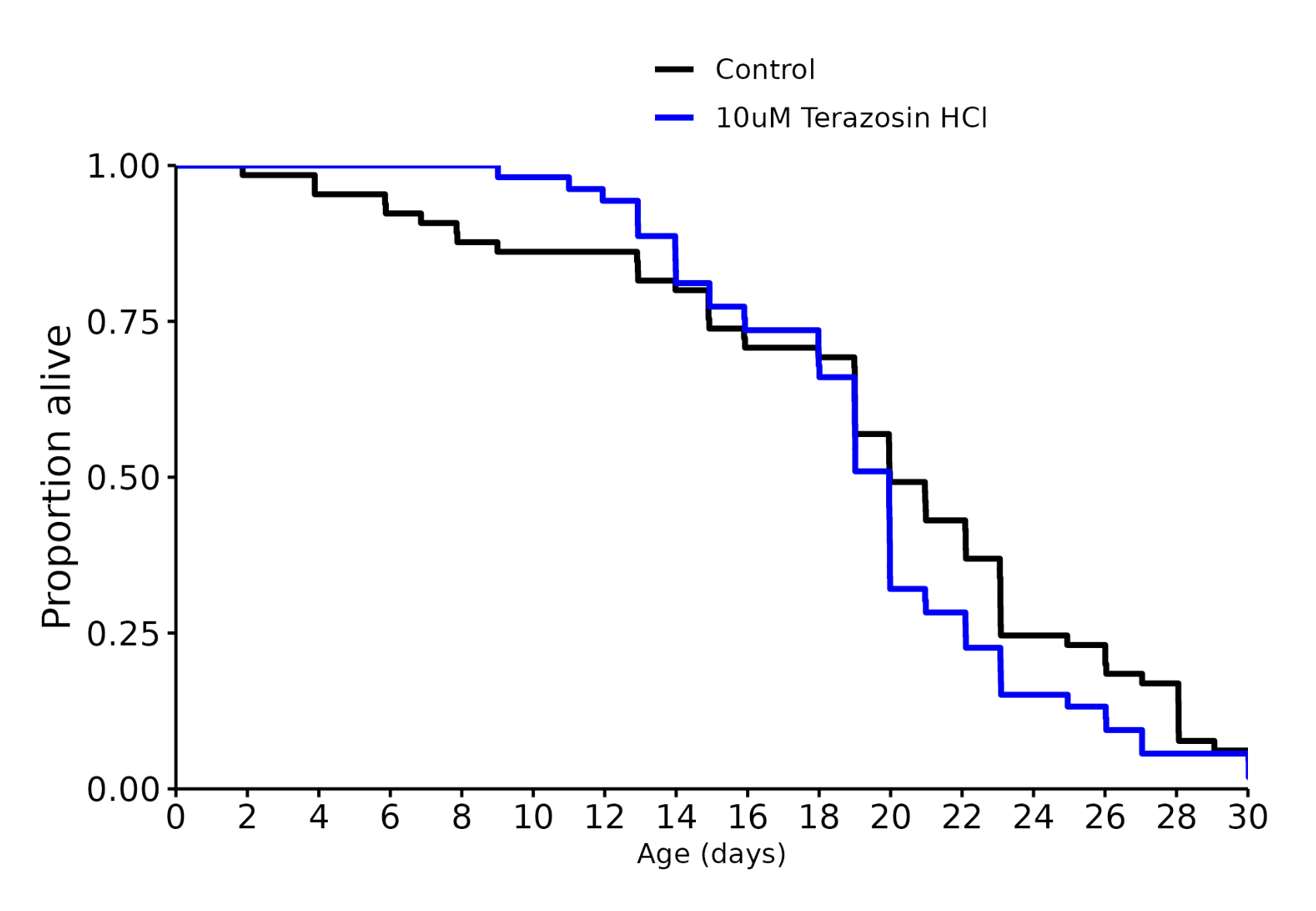
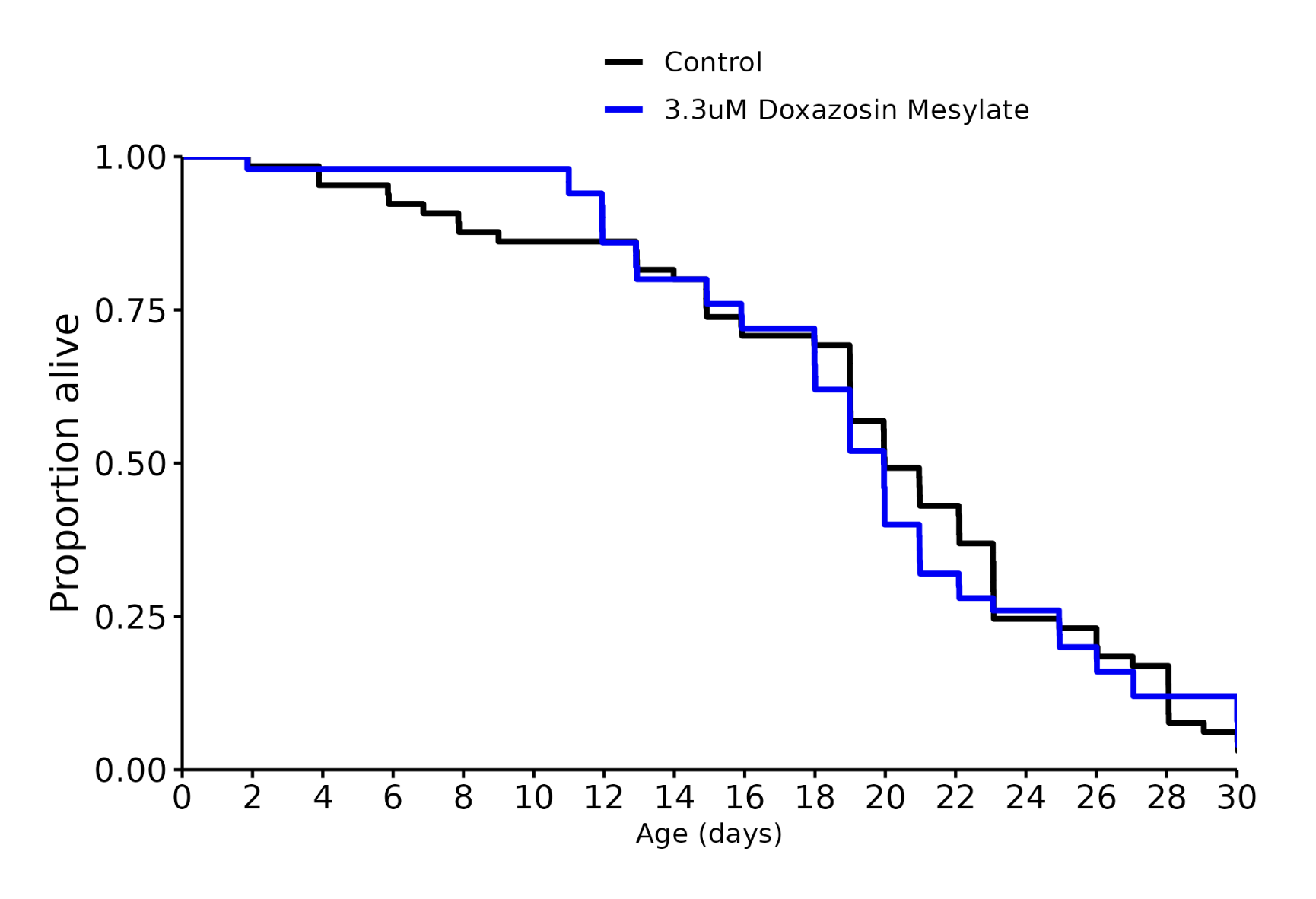
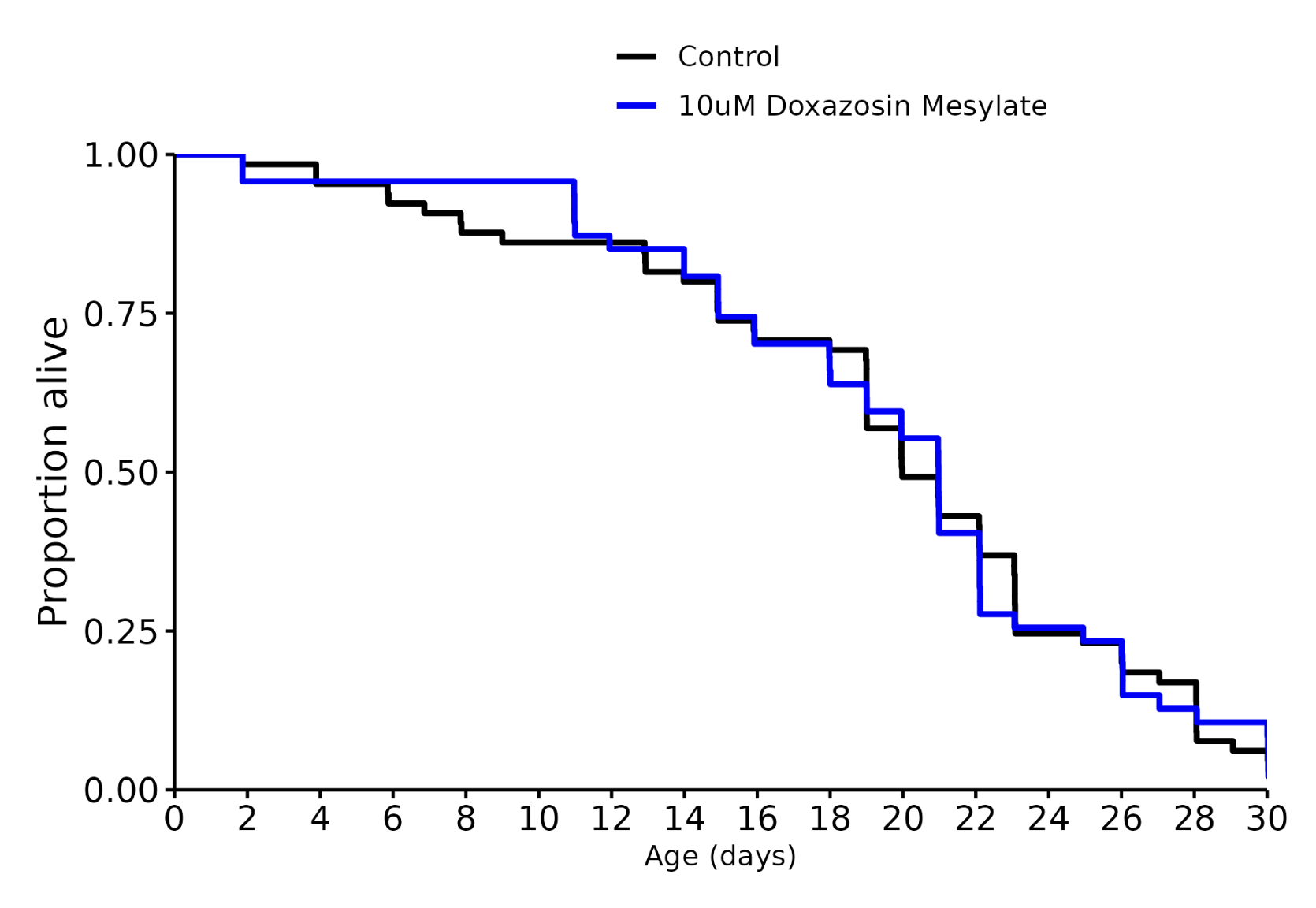
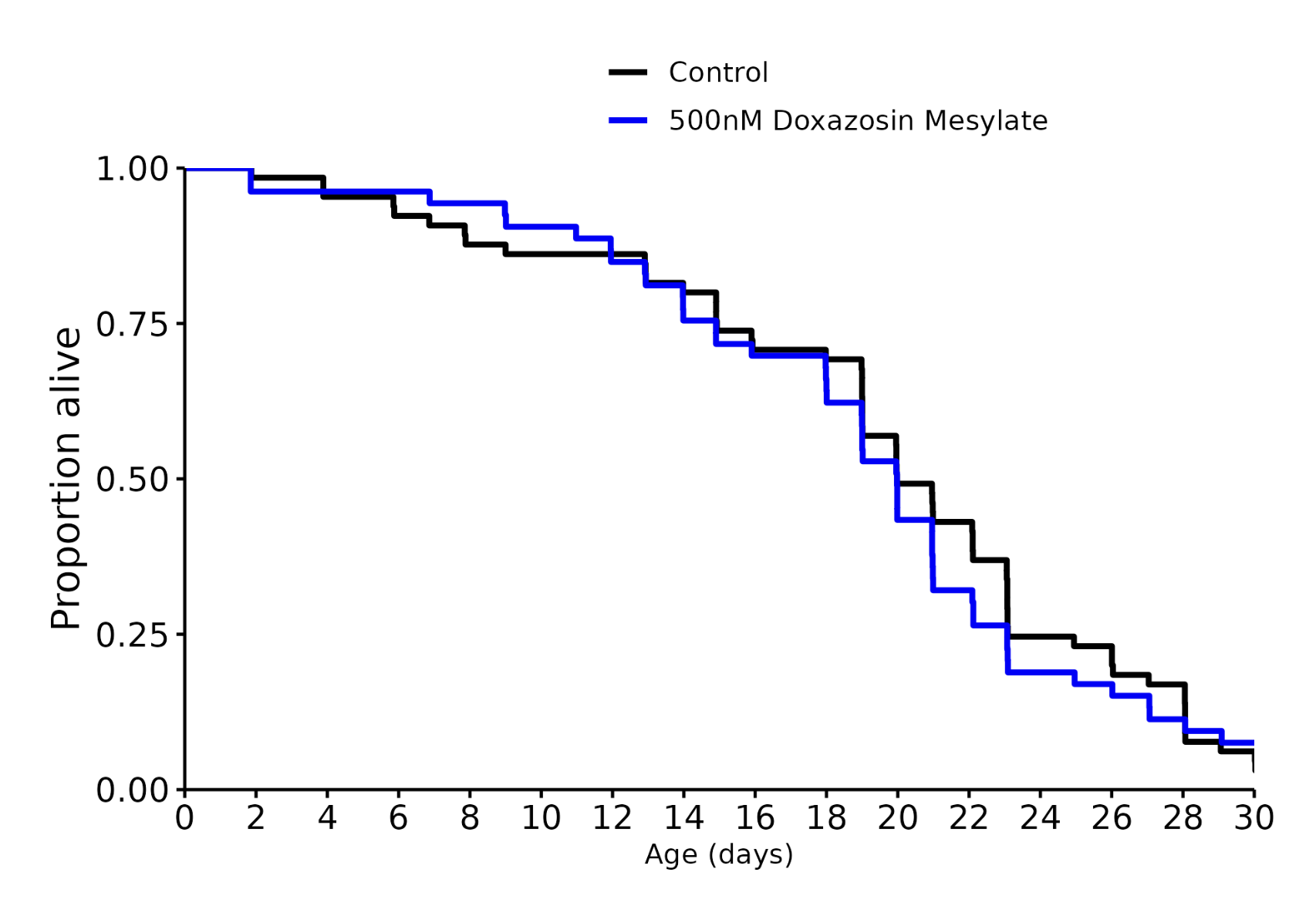
I asked Ora why doxazosin and gemfibrozil failed where they previously succeeded, answer:
While the previous 3.3uM Doxasozin Mesylate test did have an extension of median lifespan, my records show that the P-value was ~.06. While promising this does indicate that the first test wasn’t technically statistically significant from the control. Something so close to significant was definitely worth the follow up alongside a dosage curve to see if there was a better acting dose (you’ll be receiving those results very soon but my looking at the raw data, I’m seeing similar result).
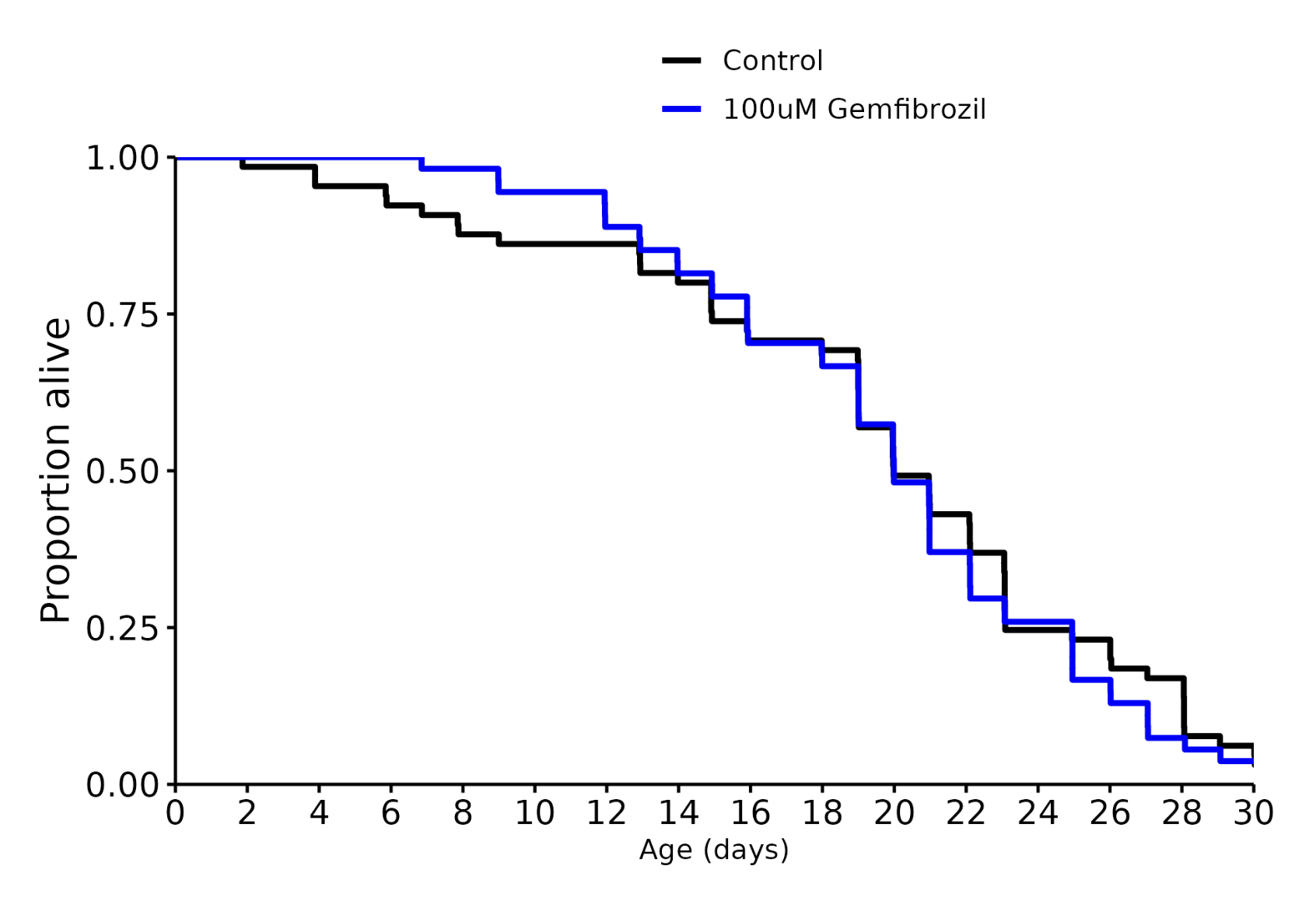
Gemfibrozil, however, did produce a significantly significant result last time. The data from the recent current experiment doesn’t show any confounds that would cause me pause. We did order a fresh stock of Gemfibrozil for this experiment, but it was from the exact same supplier as the first test. However, some molecules do change over time and the chemical supplier recommends using the reagents shortly after arrival which, to me, indicates that the Gemfibrozil is relatively unstable. I’ll dig a little deeper into the chemistry and see if there’s any interesting derivatives!
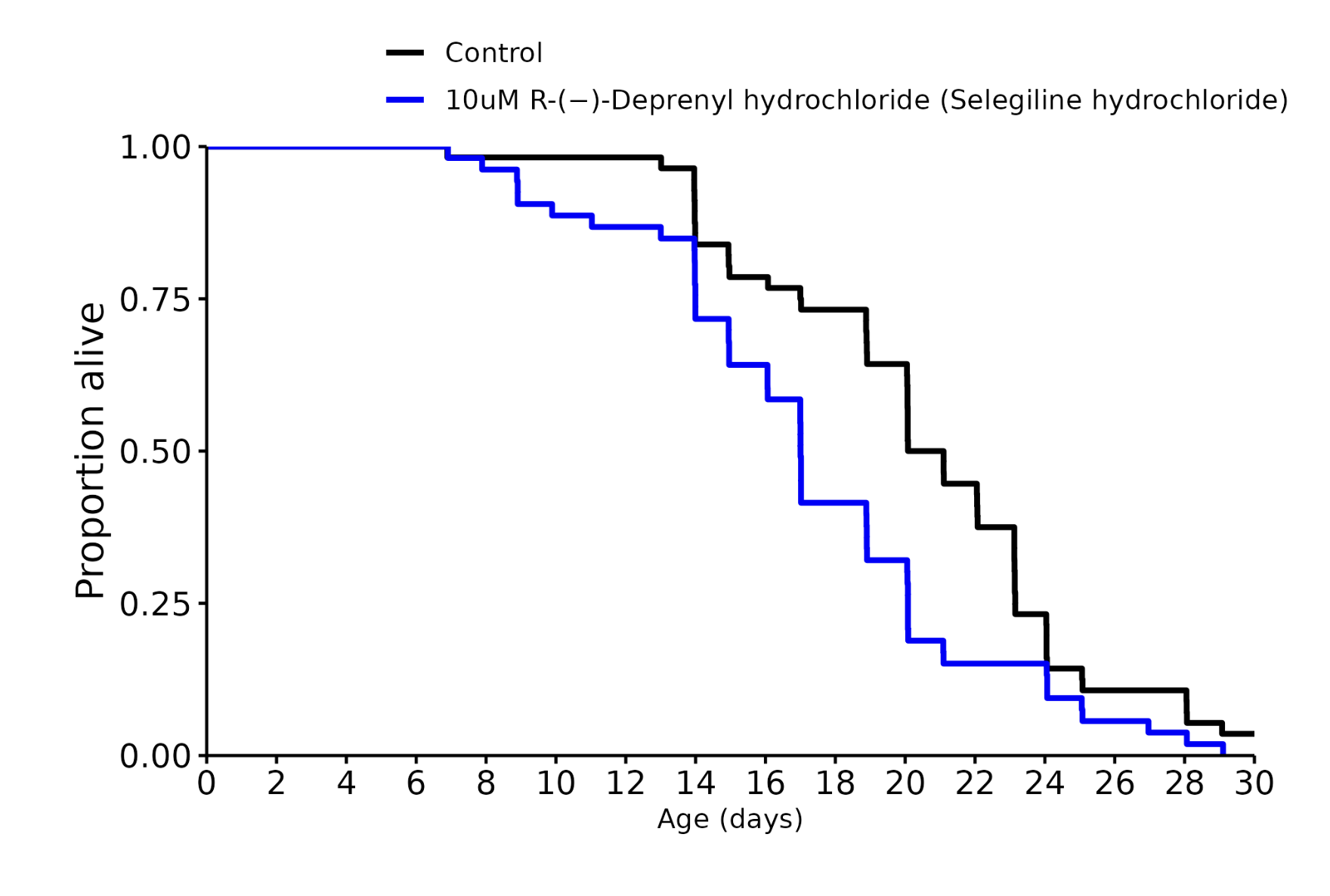
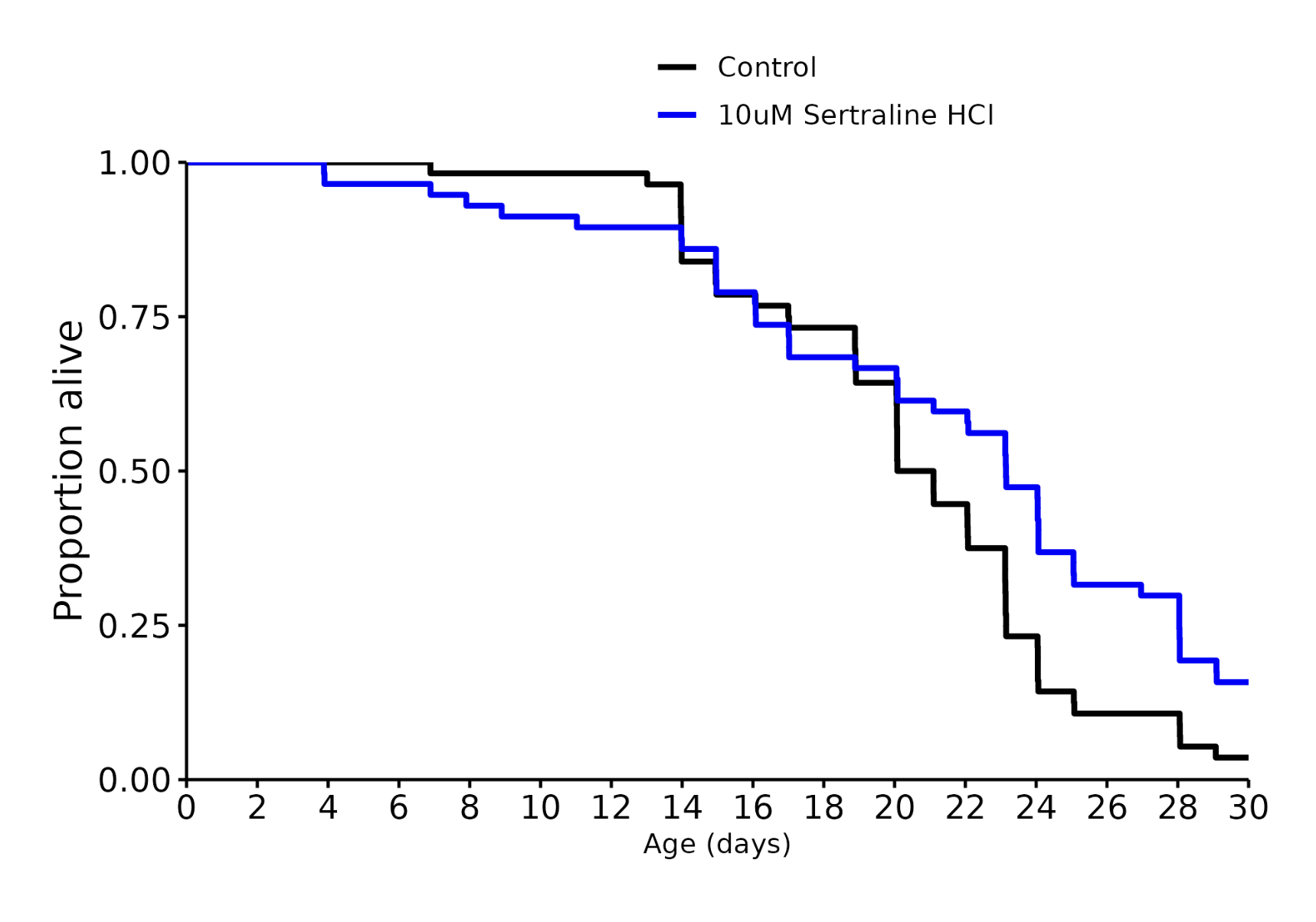
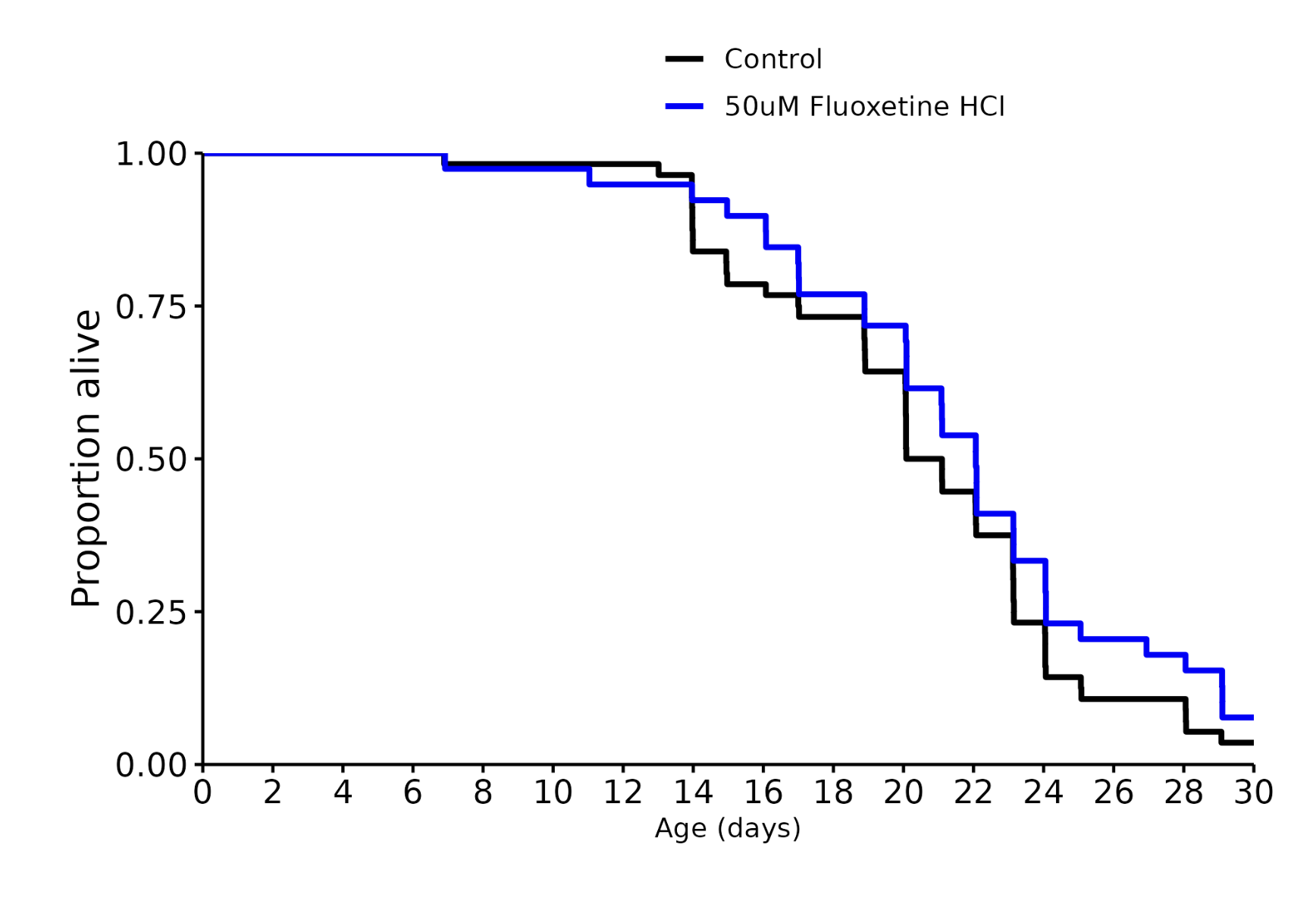
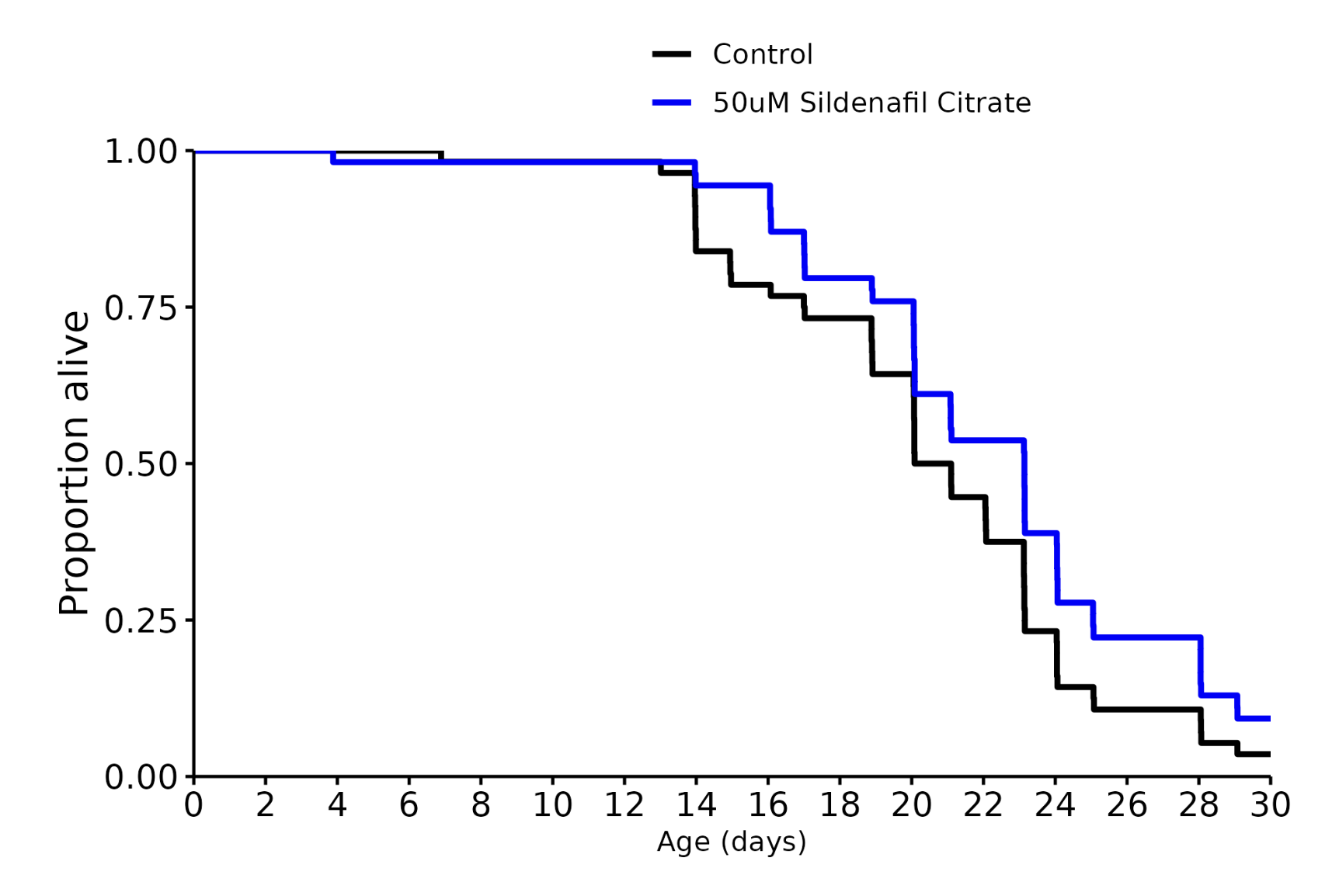
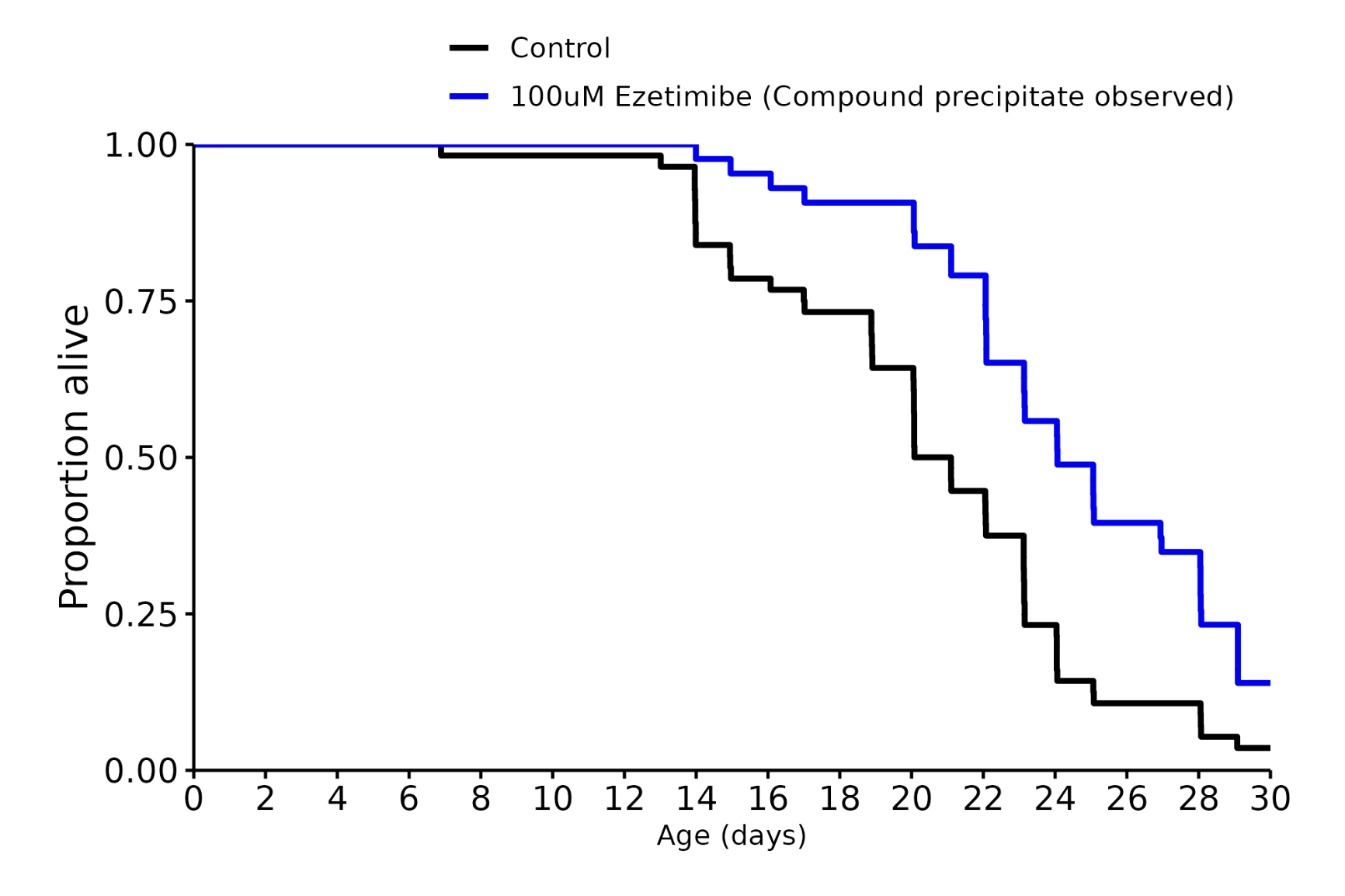
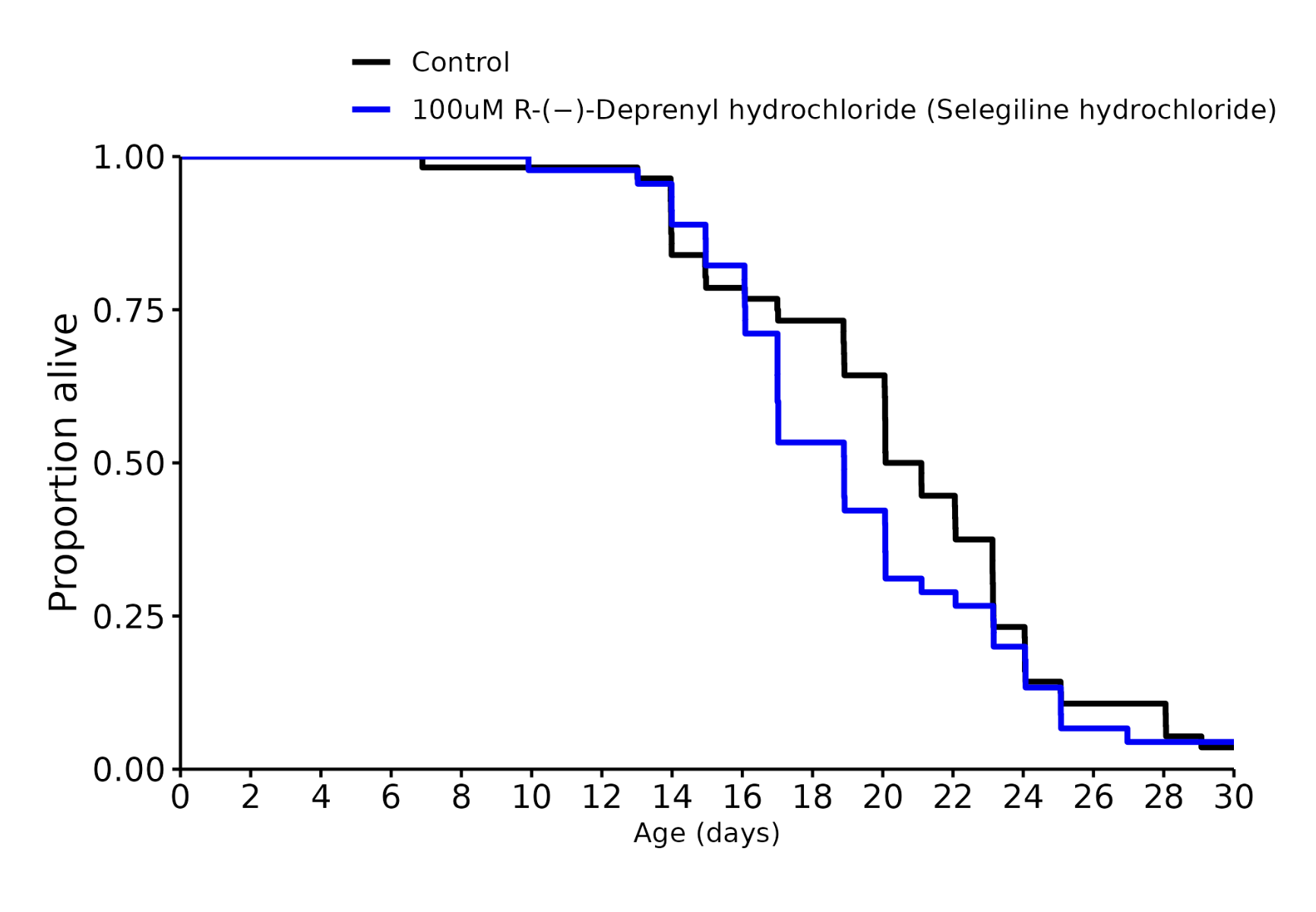
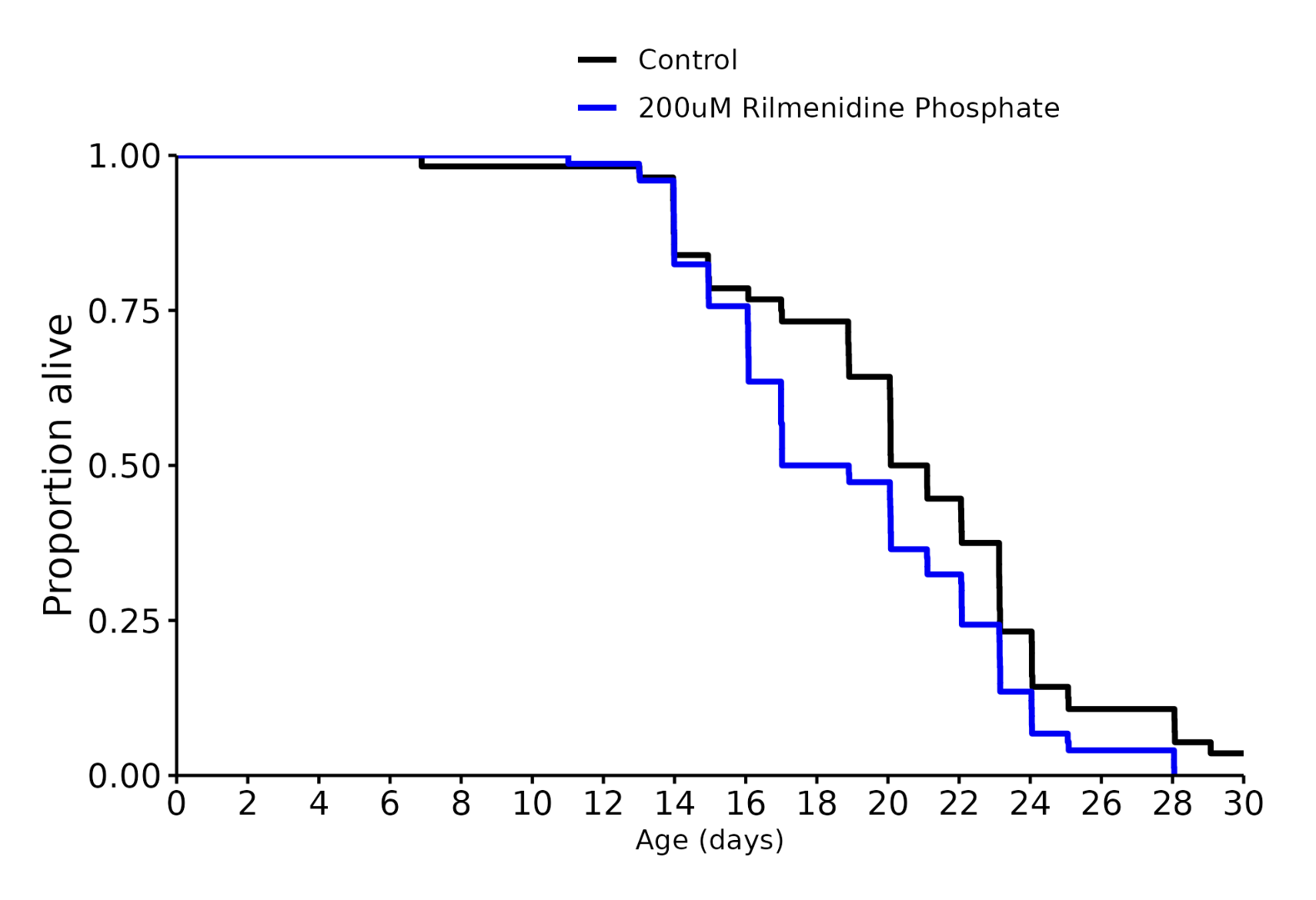
More results, most of them not statistically significant (p<0.05) except for selegiline and rilmenidipine (SHORTEN lifespan) and sertraline and ezetimibe (increase it, but with an issue for ezetimibe). Sildenafil also very close.
Has anybody, maybe from Ora, ever comments on the controls? To my eyes, they are all over the place. This really shows how important the batch effect is. Like, I think that UK/Swiss group in the Aging Cell paper should be legit, but obviously replication and consistency at different labs is a huge limitation. Surely Ora must have considered this?
Edit: For example, Rapamycin at 15µM seems to have been run three times. Median lifespan for the 3 replicates was 15.9, 17 and 17. The control was is identical every time, so I assume they used the same control population for the 3 comparisons. So all 3 Rapamycin trials had P values of almost 1.0.
But if you look at Rapamycin 15µM / Berberine-Hcl 50µM, the median survival was 19.8 days. Slightly better than 17 in the other trials. But in this experiment, the control median lifespan was only 14 days, so there was a very high statistical significance.
I also note that Berberine 50 µM by itself had a median lifespan of 20.8 days, with longer-lived controls (17.8 days).
The Aging Cell paper posted by @adssx doesn’t seem to explicitly state the median lifespan, but looking at Figure 1a, it looks to be around 20 days in their untreated controls and around 26 days in the best-performing Rilmenidine group.
So really, comparing these, even within Ora results, is extremely difficult because the control population varies wider than the improvements from some statistically significant interventions.
I don’t think it’s Ora’s “fault” but it seems like a big limitation. Guess we need to help fund a bunch more replication studies.
Hi all! Mitchell from Ora here. Looks like I was summoned by adssx
Great question about controls! When we were just starting our screening, we were testing at 25C and median lifespan for controls was around 15 days. More than a year ago by now, we switched over to 20C and have seen control median lifespans shift to around 18-20 days. The shift in temperature accounts for most of the difference and is well documented in the literature.
That said, it is incredibly important to look at the internal experimental controls when assessing lifespan effect. There is random variation and sometimes unaccounted for experimental variation, even in standardized experimental pipelines like at Ora.
We are always trying to capture more data to give us a better understanding of what covariates influence lifespan and have an NIH grant that is letting us develop the best systems for egg-to-death tracking. That’s in development and will be rolling out in the next few months!
Another great point is around replication studies. Because experimental methodologies vary greatly from lab to lab and there is latent variation, understanding consistency and robustness of effects are key. I really appreciate that so many in the community are leading retests of published results. Replicating published studies is not done that often and is a huge unmet need in science.
Thank you all again for helping advance longevity science! And let me know if I can answer any other questions!
Interlab variability is why the ITP is such a treasure. I think people underestimate how often studies that show various effects in animals (and humans) are extremely lab dependent. When I see a study, particularly one with outsize or unusual results, I always keep in mind “let’s see this replicated in a different lab”. Meanwhile a ton of research is often “replicated” by the same lab or team of researchers. I just finished a deep dive on a supplement and was frustrated by this very problem - big result, and the only replications and consequent self-citations were by the same lab over the span of years.
This is why just reading the abstract and conclusions is completely worthless (the usual MO of pop press headlines). You really have to dig into the methodology because that’s usually where the crimes are hidden.
Looks like c. elegans have MAO-A enzymes but not MAO-B. Selegiline is primarily a selective MAO-B inhibitor, though it also does have MAO-A inhibition at high enough doses. I’m not sure what the mechanism would be for the purported longevity promoting effects of selegiline, but I thought it’d be good to point out the very big difference between c. Elegans and humans (and likely other species).
That’s awesome, thanks. I hadn’t spotted the differences attributed to temperature, but now I see it. What you’re doing is brilliant, and my post wasn’t intended as a criticism.
So what is the biggest thing we, as a community, can do to help? Should we help fund more replications of some successful interventions, which would then run a new set of controls? Or should we be looking at alternative dosing? What’s your advice?
I’ve noticed the exact same thing. For example, in senolytic field the consistent, best results really come from only one lab. Then irisin failed the ITP, and when the same lab received blinded samples from the mice, they couldn’t measure any difference in senescence. That just screams investigator bias to me. Presumably unintentional, but if a molecule only “works” in the hands of one lab, with one mouse strain, that’s not very useful in helping me to live to 110.
Replication and dose response studies are two very important ways we can improve the quality of the science across the field and advance our Million Molecule Challenge Database together.
When you have a study in mind and want to get an experimental quote, send us over the paper as well. We’ll have a look and do our best to understand differences between approaches. We are also bringing online killed food studies, which gives us even more ability to replicate findings and understand how food type impacts intervention efficacy.
I think the biggest problem with the MMC results for now is the huge question marks surrounding translation. The physiology of roundworms is so different from us that any sort of superficial analysis of how these interventions affect them will fall short. Even getting down to the level of cellular assays, due to the much greater cell type diversity in humans, it’s almost impossible to predict how a result might translate.
At least with mice we can show that an intervention modulated inflammation, fibrosis, markers of active immunity (roundworms don’t even have an active immunes system), etc, and due to the conservation of these processes, along with the various organs/tissues, stem cell niches, endocrine regulation, etc, it’s much more likely that results in mice will translate to humans, at least compared to roundworms
I think one potential path forward is to standardize one or a few epigenetic assays for C. elegans. They don’t generally regulate their DNA by tagging cytosine bases with methyl groups, so DNA methylation assays are not appropriate. But if we obtained their histone modification data instead, we could study how the principal components evolve with age/in response to the drugs and how these changes relate to the patterns seen in the methylation PCA data of mice and humans (similar to what Fedichev is doing).
Acetylation (my favourite PTM - Post Translational Modification) is quite dynamic so I think it would be really hard to monitor it might need some form of flourescence or something to monitor it as it is going on. Obviouly it can be tested for, but at that point the cell is probably broken in some way so what you see is not going to be exactly what you would get in vivo.
My approach with acetylation is to try macroscopic interventions and see what macroscopic changes occur.
In the mean time I think C. Elegans has relatively little value because of things like not having senescent cells and the sensitivity to the health of E. Coli (food). On the other hand I am willing to fund the experiments being proposed with Indolepropionamide where we have three people willing to put up USD100 towards the USD400 costs because Indolepropionamide is such an interesting molecule with so little data and a little data would be good value even it is simply that the worms don’t have a lifespan change.