A common method used to estimate the MAP is the following formula:
MAP = DP + 1/3(SP – DP) or MAP = DP + 1/3(PP)
Where DP is the diastolic blood pressure, SP is the systolic blood pressure, and PP is the pulse pressure. This method is often more conducive to measuring MAP in most clinical settings as it offers a quick means of calculation if the blood pressure is known.
Per Wikipedia: “It is used clinically to estimate the risk of cardiovascular diseases, where a MAP of 90 mmHg or less is low risk, and a MAP of greater than 96 mmHg represents “stage one hypertension” with increased risk.” Mean arterial pressure - Wikipedia
My blood pressure variation (on a settled state) is primarily driven by the level of recent alcohol consumption.
I accept that on a net basis alcohol consumption is probably a health negative, but at least that issue should be controlled for before doing a meta analysis.
I am doing a lot of BP tracking at the moment because I think I have driven up my resting heart rate by increasing mitochondrial efficiency and it is taking some time for my cardiovascular system to adjust to this. With a higher heart rate I expect a slightly higher BP until the systems adjust.
However, particularly over Christmas I am also drinking quite a bit of alcohol which has an immediate effect on blood pressure of a substantial (10-20mmHg) of both systolic and diastolic BP. (eg to 106/64 hr 69).
@John_Hemming why would higher mitochondria efficiently lead to a higher RHR? Why wouldn’t higher mitochondrial efficiency lead to less ROS —> lower physiological stress —> lower RHR?
Its a physics thing. If the heart for a given stimulus has more power it will cycle more quickly. The cardiovascular system then needs to adjust for a more powerful heart.
Are you saying RHR increases at first but then would decrease below baseline? I would expect the body to be quick to adjust to mitochondria changes. But that’s just a guess.
The European Society of Hypertension also published a long and detailed position paper on BPV. They note its importance and the lack of clear guidelines. Regarding potential treatments: “In the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) study, calcium channel blockers (CCBs) reduced VVV, whereas β-blockers (BBs) had opposite effect […] In summary, different antihypertensive drug classes may have different effects on BPV, with some evidence that CCBs may induce the most effective long-term BPV lowering. […] Greater BPV reduction is achieved with the use of combination therapy compared to monotherapies […] The sleep-time administration of CCBs as monotherapy or fixed-combination therapy has been associated with decreased BPV and MBPS”
Issue Section: CardioPulse
Systemic hypertension remains a constant threat to global health due to its direct contribution to premature morbidity and excessive mortality.1 The risks associated with hypertension relate to both disease duration and severity. Traditionally, blood pressure (BP) has been categorized as ‘normal’ or ‘abnormal’. This definition of ‘normal’ BP somehow implies a ‘safe’ level in terms of protection against cardiovascular disease (CVD).
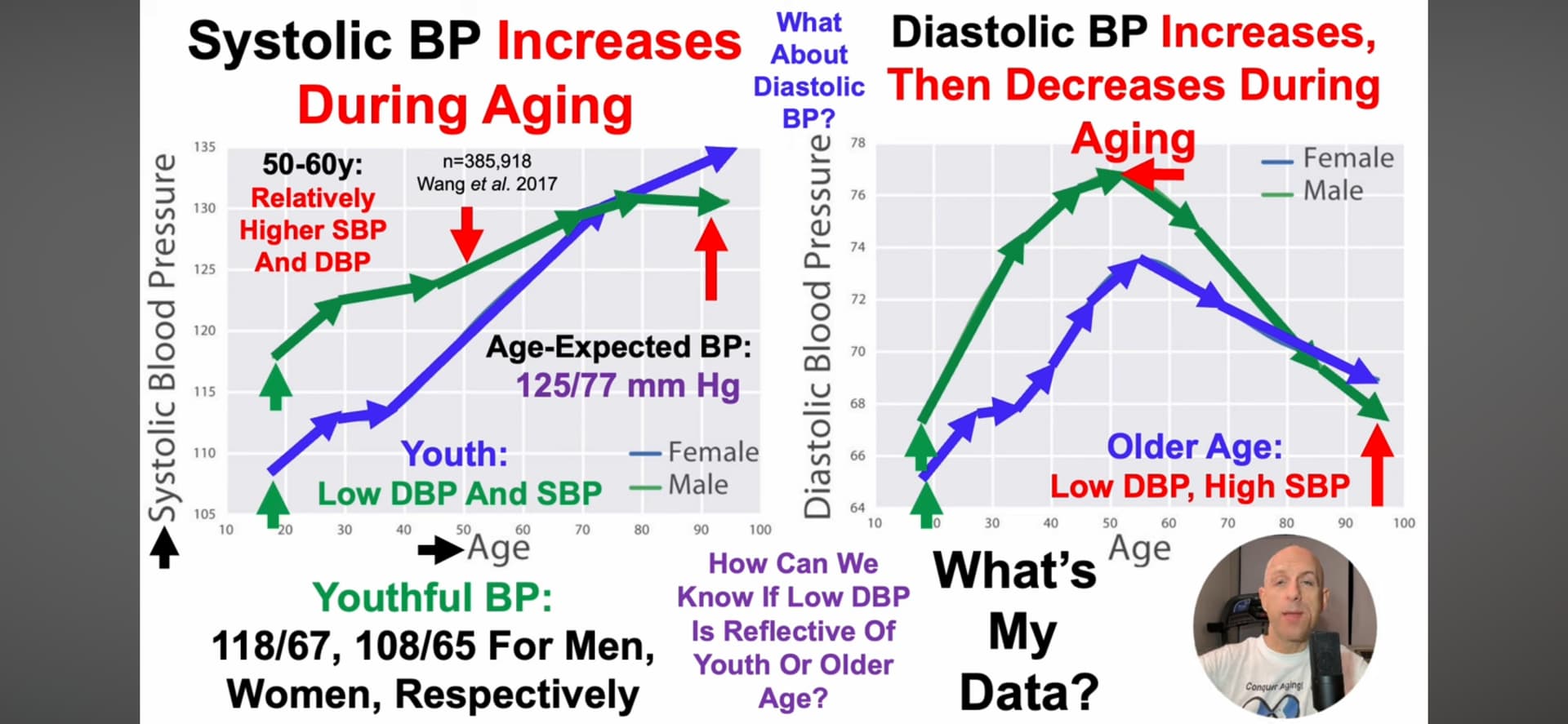
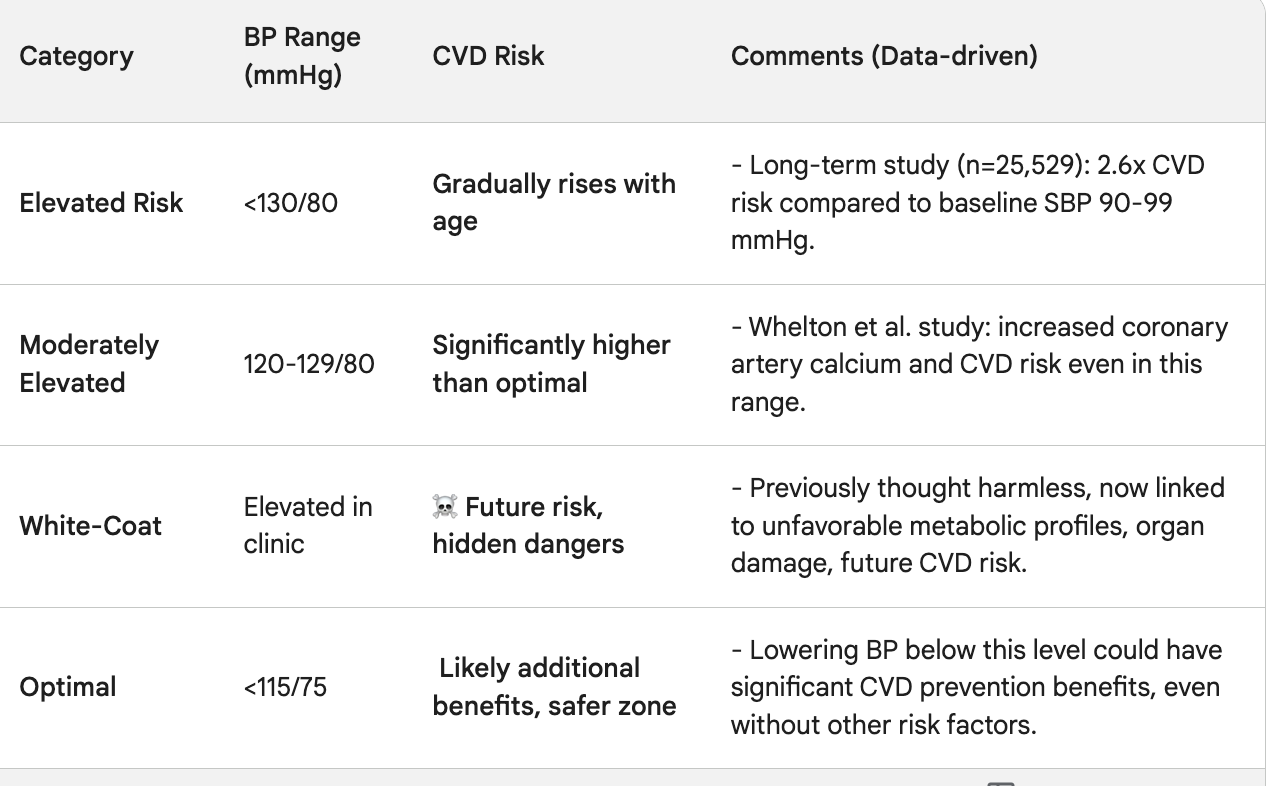
However, the concept of ‘normal’ BP and its definition have evolved over time. A long-term study in which a large Chinese cohort (n = 25 529) was followed for 10 years reported that CVD risk varies and increases within the range of ‘normal’ BP.2 Over a period of 10 years, the unadjusted risk for CVD for individuals with a baseline BP of 120–129 mmHg was found to be 2.6 times higher than that in those with a baseline systolic BP (SBP) in the lowest category (90–99 mmHg). As individuals with a baseline SBP of 120–129 mmHg were older than those with an SBP of <120 mmHg, risk-adjustment analyses indicated that ‘normal’ BP was not safe with progressive aging. Obviously, aging is inevitable. The question is, can we prevent age-related rises in SBP from 90 to 129 mmHg, as maintaining SBP at 90–120 mmHg despite advancing age appears to be protective against CVD?
Notably, even normal BP has been shown to cause pathological changes in the cardiovascular system. SBP levels typically considered normal have been associated with an increase in coronary artery calcium score, further highlighting the increased risk of vascular disease at BP levels that are not in the range of ‘traditional’ hypertension.3
Several population-based studies have demonstrated that SBP levels currently considered normal (<130 mmHg) are not safe, and in fact, there is a graded increase in CVD risk as SBP increases beyond 90 mmHg.4–7 Whelton et al.6 found that the amount of coronary artery calcium and the risk of incident atherosclerotic CVD increase with increasing SBP levels, even in individuals with SBP 90–120 mmHg. In fact, mounting evidence has made it abundantly clear that so-called high normal BP levels (120–129 mmHg) are associated with a significant increase in incident CVD compared with SBP levels of 90–100 mmHg. This connection may be much more pronounced in yet to be identified subgroups. This means that CVD risk starts even when SBP is a long way below 130/80 mmHg, which is the current threshold used to diagnose and define hypertension.8 Therefore, the guideline-based definition of normal BP does not provide freedom from CVD risk. Without a doubt, SBP of 120–130 mmHg is a harbinger of significant chronic disease burden and portends a poor prognosis. Overall, CVD risk appears to be independently associated with SBP levels, starting at 90 mmHg.
In addition, there has been a large shift in the perception towards white-coat hypertension (WCH) in the last two decades. Once believed to be an innocent phenomenon that does not carry any greater risk of poor cardiovascular outcomes compared with ‘normal’ BP levels, WCH has now been linked to unfavourable metabolic risk factor profiles, a higher incidence of asymptomatic organ damage, and a greater risk of progression to high cardiovascular morbidity and mortality.9 This further calls into question what we consider ‘normal’ BP levels.
Even in the absence of any co-existing risk factors, subjects without a diagnosis of hypertension would benefit from having their BP lowered to well below 115/75 mmHg. While the estimates are speculative, there is enough scientific evidence strongly supporting the concept of ‘optimal’ BP rather than ‘normal’ BP. Future guidelines and policies should be substantially modified to advocate optimal BP as the standard, instead of normal BP as currently defined.
The biological risk associated with a given BP level should perhaps be correlated with indices such as left ventricular mass and levels of N-terminal pro B-type natriuretic peptide and high-sensitive cardiac troponin T. However, obtaining these data in clinical practice is expensive, although it could become cost-effective in the future. Furthermore, lowering BP to a new normal—‘optimal’ BP—requires urgent global action to achieve the primary prevention of CVD (Figure 1). Until that lofty goal becomes a realistic possibility, normal BP is no longer a safe haven.
I’m more and more realizing that most of the “normal” ranges for medical/biological measurements that have been developed (at least in the USA) over the past 20 or 30 years are likely heavily skewed into the unhealthy range by the ever-worsening obesity epidemic in the US.
Moreover, it seems that many of the measures are the “average” that has been measured over time and have no relationship to the optimal… if you want to live as long and healthy as possible.
I was in a hospital last week fro a planned surgery and spent three days there. They were measuring my BP every 2-3 hours and the average was 105/65 which I consider a great BP, but when it came to pain management after surgery I was told my BP is too low to use opiates without heart monitor. They had me first on saline solution to raise my BP
Like I’ve said about people happy about a normal cholesterol result: “Well I suppose that’s correct, but will result in normal levels of heart disease?” And then they defend it by mentioning fake U-shape curves with lots of confounders!
Well, each person has their own priorities. Some only care about healthspan so cholesterol is not an issue for them if all they want are 50-60 healthy years.
Well, heart attacks are no fun, and reduce healthspan. There is for most people no side effects to reduce cholesterol, so it’s very nice to be able to avoid them and strokes.
People mistakenly think they have to change anything when they just have to pop some pills.