By the way, I have the “NEW Aktiia” that is supposed to be waterproof, “70% easier to initialise” (what does that even mean?!), “31% lighter”, and with “a 7.5% increase in daytime data density”. However, it seems that you can only buy that new device on this special hidden Christmas page. The normal page still shows “Not Water Resistant” and “Weight 20g”. Great product but terrible communication…
I ordered the “NEw Akttia” and had it delivered to a friend in the UK. Looking forward to playing with it when it arrives in Canada. Thanks for the background info @adssx!
Hi @Tomnook: which interventions did you do (if any) to go from 169/96 to 117/72?
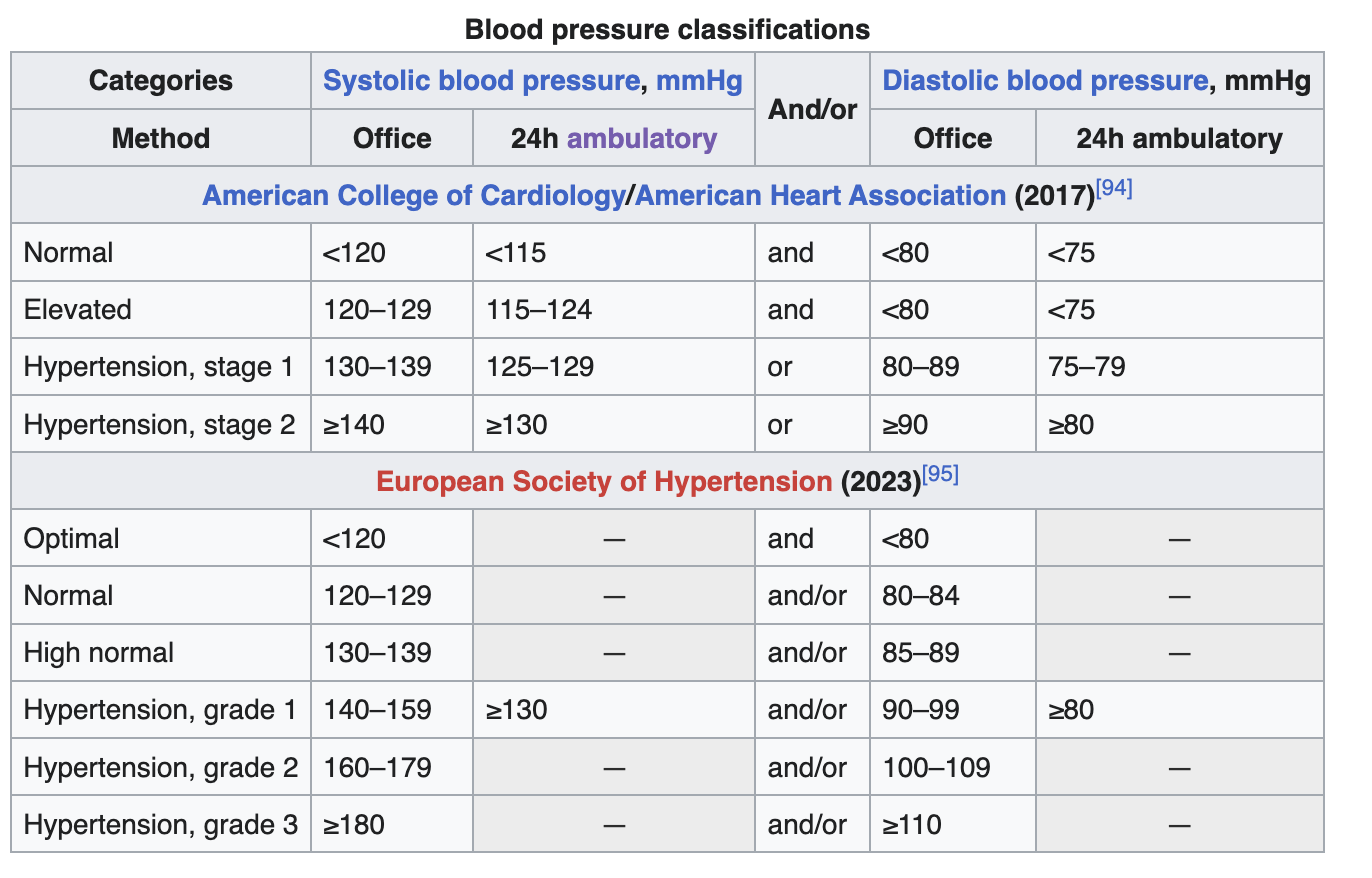
Also, on these reports, I find it so annoying that they use different definitions of hypertension. On the “Monthly graph view - BP”, the red lines show 130/80, which is the European threshold for hypertension based on 24h ABPM. It makes sense as Aktiia is a 24h ABPM. However, in the “Percentages in range”, the color map uses the office limits (still from the European guidelines), so 140/90 at the limit for hypertension. It’s not their fault, as the European guidelines only give the detailed classification of hypertension for office BP measurements. (And to make things worse, on the home page of the app, they use the 135/85 cutoff, which is for home measurements) It doesn’t change the value but it makes the interpretation less easy. For instance, I appear in “High blood pressure stage 1” in the monthly graph but “Elevated” (aka normal) in the color map.
Anyway, I’ve just started telmisartan 20 mg. I guess it’ll take a few weeks to see the effects.
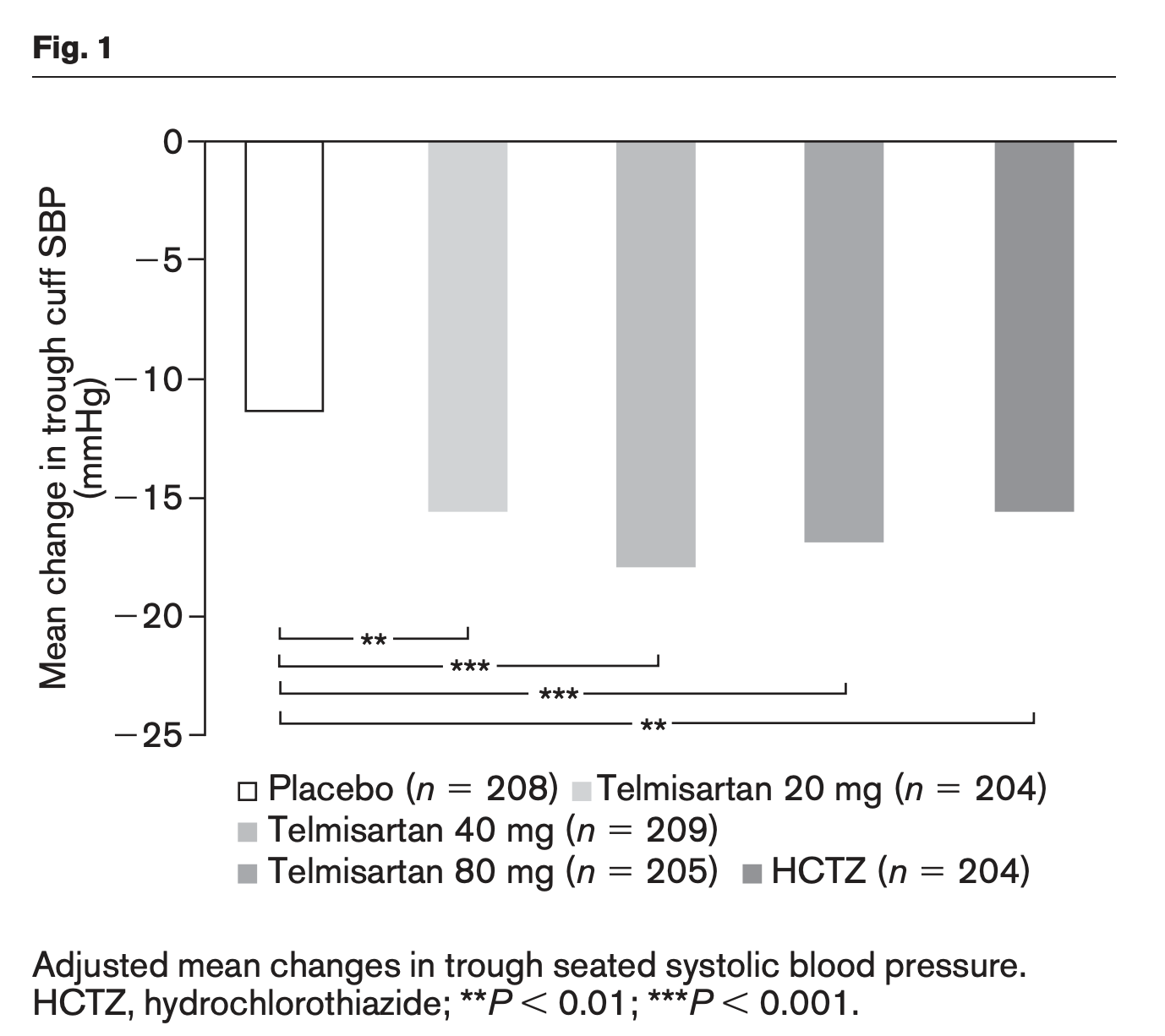
Following once daily administration of telmisartan, the magnitude of blood pressure reduction from baseline after placebo subtraction was approximately (SBP/DBP) 6-8/6 mmHg for 20 mg, 9-13/6-8 mmHg for 40 mg, and 12-13/7-8 mmHg for 80 mg. Larger doses (up to 160 mg) did not appear to cause a further decrease in blood pressure. (https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020850s022s023lbl.pdf)
Overall, the dose–response curve with ARBs was shallow with decrease of 10.3/6.7 (systolic/diastolic), 11.7/7.6, and 13.0/8.3 mmHg with 25% max dose, 50% max dose, and with the max dose of ARBs, respectively. […] we observed a shallow dose–response curve, and uptitration marginally enhanced the antihypertensive efficacy.
So, what would be the second-best antihypertensive after telmisartan? So far I’d say dihydropyridine CCBs such as amlodipine but there’s not much data. Amlodipine seems to have good synergy with telmisartan (and telmisartan/amlodipine is on the WHO List of Essential Medicines):
Hi!
I’m still doing pretty much the same as I was when asked earlier in this thread. I now use the ‘new’ Aktiia (seems virtually identical to the previous version although I must say the bracelet connects more easily for readings). My BP has risen slightly over the past month 119/74 average up from 114/73 - maybe I wasn’t as relaxed when I ran this month’s calibration.
Two years ago when I was admitted to hospital my BP at the doctor’s was 220/100 - it fell to 200/100 at admission and after two or three days it was down to 180/90 - they started me on ramipril 2.5mg od and amlodipine ccb 10mg od. There was little change so the ramipril was upped to 10mg od. After four days I was discharged after showing the consultant my Akttia readings when I was relaxed in the hospital bed compared to the hospital readings when they wheeled their infernal machine over to me - the readings were never under 180 (which I needed them to be for discharge).
The consultant suggested reducing salt in my diet (vegetarian but ‘ready meal’ type of food - high salt content) whilst also stopping eating liquorice (which I’d not previously realised the effect of).
A week or so post discharge I stopped the ccb due to a noticeable increase in pulse rate and an apparrent decline in hrv.
Over the following months I reduced the ramipril to 2.5mg od (before bed) and remain at this dose.
I started a number of supplements all of which I still take on a regular basis and many of which I took on and off over the fifteen years prior to this event. The only ones which I’m fairly certain have some effect are arginine and l-citrulline and beetroot powder. Here are all of them:
Arginine 2g am
Citrulline 2g pre bed
Beetroot 1g 20:1 extract
Hawthorn powder (fruit and leaves)1.5g 20:1 extract
Krill oil 1g
EPA/DHA 1g
Astaxanthin 12mg
Pine Bark extract 400mg 15:1
I also practice mindfulness a couple of times a day for 1 minute and also for 5 minutes before sleep.
Increased daily water intake significantly.
I’m retired and, as far as possible, consciously avoid situations which I know would raise my BP - realively easier to do these days.
Your comments about telmisartan are interesting and the studies I’ve just looked at make it the obvious choice as the ARB to try. I asked my GP if he’d prescribe me an ARB originally but he wanted to try ramipril first so I’ve stuck with that. There is synergy in taking low doses of both ramipril and telmisartan in some studies it appears.
Amlodipine appears to be the most commonly prescribed ccb and combined with the telmisartan looks like a good combination.
I understand your comments about the Aktiia kit - I hadn’t thought about them before - I was just keen to get my levels into the green zone and then, once there, keep them in it!
When I got 24h ABPM device I got some patient information that states in short that normal BP is considered 24h average lower than 115/75 mmHg. If BP is greater than 125/75 (again 24h average) you are probably hypertensive and BP will be further evaluated.
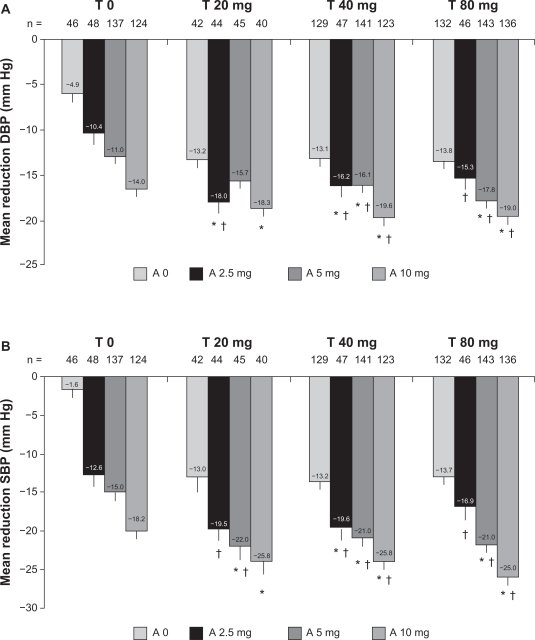
Yes, my conclusion so far is that the best strategy to achieve the desired target is: Telmisartan 20 mg => T 40 mg => T 40 mg + Amlodipine 2.5 mg => T 40 mg + A 5 mg => T 40 mg + A 5 mg + Hydrochlorothiazide (HCTZ) 12.5 mg
In both trials, these ‘hypertension polypills’ were superior to usual care, achieving >80% BP control without increasing withdrawal due to side effects. However, there are no such products available for prescribers. To address this unmet need, George Medicines developed GMRx2 with telmisartan/amlodipine/indapamide in three strengths (mg): 10/1.25/0.625, 20/2.5/1.25; 40/5/2.5.
The systolic BP (SBP)-lowering efficacy of GMRx2 strengths 1, 2 and 3 (Table 2) from a baseline SBP of 150 mmHg are expected to be approximately 13 mmHg, 18 mmHg and 25 mmHg, respectively. This represents a much greater and clinically important BP reduction in comparison to standard-dose monotherapy, which reduces SBP compared with placebo by only 8–9 mmHg on average, with each doubling of dose conferring only a 1–2 mmHg incremental SBP reduction
They completed the trials. I can’t wait to see the results.
[Update: actually, indapamide might be better than HCTZ as it has a longer half-life and might cause less insulin resistance. Telmisartan is the longest-acting ARB and amlodipine is the longest-acting CCB and long-acting drugs are preferred to reduce BPV per this source. So Telmisartan/Amlodipine/Indapamide might be the best combo out there.]
I agree that 115/75 mm Hg should be the ideal BP (if not lower). Unfortunately, the 2023 European guidelines still give 130/80 as the 24h ABPM threshold for hypertension while the American guidelines have been lowered to 125/80 since 2017:
I did a 24-hour ABPM in 2015 in France (130/69) and in 2022 in the UK (132/73), and in both cases the cardiologists concluded that I was “normotensive”. (To their defense, “Isolated systolic hypertension of the young” [ISHY] is apparently common and not associated with an increased risk for non-smoking and physically active tall men.) I tried to argue a bit (it seemed stupid to me to have an arbitrary threshold set in stone versus seeing things as a continuum) but I didn’t know much back then (and I had other things to focus on…).
I thought this might help you make your decision: Aktiia has 4 ongoing trials. Omron: none? So, at least Aktiia seems quite confident about its product and serious about proving its accuracy. And we might get the results of the first trial by the end of this year:
(Still think there incentives are different - so when they are behaving consistent with just following those incentives it does not give us a strong signal of their products accuracy in isolation, just more about what they think the Return on Investment (RoI) of their actions are
For example, say hypotheticallythat omrom actually is 40% more accurate. Since their device is clumsy snd invasive, not “Apple” experience, sexy, trendy”, streamlines and not invasive at all - they would have a low RoI on more trials vs just US FDA clearance.
For Aktia, where in this example things are the reverse and they can go after a much larger consumer, health focused market and having more trial data (as long as it is good enough to cherry pick from) for similar type of marketing to eg a Mitopure likely has a much higher RoI than for Omrom)
(Also could be that Aktia is aggressive startup culture and VC demands for massive growth while Omrom is older, more entrenched, where this watch is just a tiny part of their product offering).
For Aktiia users: on which hand do you wear it? I feel like the default is the “strong” hand (right for right-handed people) because you wear your watch on your “weak” hand (left for right handed people) but I realize that my strong hand moves more than my weak hand so I wonder whether I could get more frequent data points on that hand. I say this as I noticed I had 6h without any data point today. I guess I moved too much?
I never get that much time without data. Check the fit, it really needs to not be too tight and not too loose. I noticed that I have to adjust few times during the day, since my wrist size fluctuates that much. I complained already several times about it here so I might do it another time. I really hate the bracelet design.
I noticed that Aktiia won’t measure when I am walking, but sometimes takes measurement when I am biking. If I move a lot, the minute I sit down it takes measurement. If not successful it will repeat measurement in few minutes later. I usually get 28-32 daily measurements. If I spend the day mostly not moving (I was recently in hospital few days) it takes full 48 measurements.
Once my phone did not have internet connection when it was syncing the data and I closed app before getting online and I lost those measurements. Now after few months I sync the data every few days. At the beginning I was obsessive and did it every few hours.
I wear it on my right wrist (dominant hand) as I wear my watch on my left wrist.
It was 4h during the night and 2h around lunch. Never happened in the previous 3d (27 to 34 measurements). I’ll see… Or I might put it on the other wrist.
I’m currently obsessive and checking every few hours indeed They recommend to open it once a day apparently.
How comfortable is it, in terms of wearing it to bed and sleeping with it? Does it bother you much? Is it fine and easily tolerated?
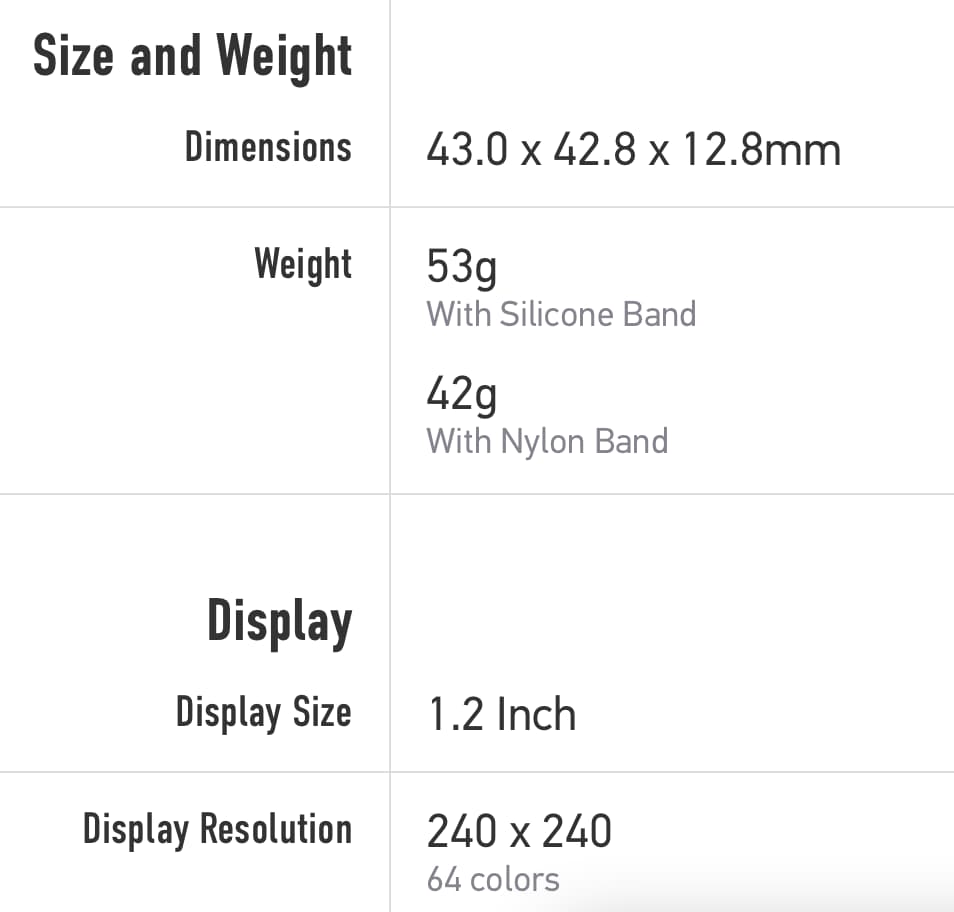
I have a large Corus Apex 2 sports watch with heart monitoring, etc. and its just a little too large and heavy to want to leave it on all night… here are its specs: (and the specs of the Aktiia, which is much lighter, less than half the weight of my watch).