Very informative article AgentSmith linked above. I wonder what the efficacy of low dose, say .25mg, oral finasteride would be compared to topical. Since, the topical would go systemic anyway to a degree, it would certainly be a lot cheaper to go that route since topicals are expensive compared to pills.
2 Likes
Another one falls victim to “Post Finasteride Syndrome Fear”.
Before:

After:

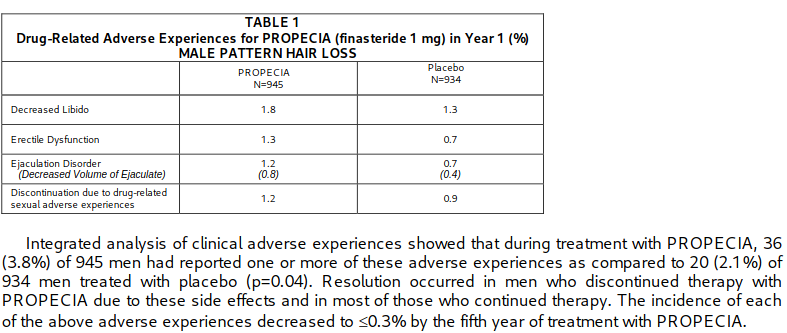
All because of a 2 → 4% risk of side effects (Propecia Randomized Controlled Trial).

5 Likes
With statins, if you fall for fearmongering you likely won’t face any repercussions for decades. With finasteride, if you fall for fearmongering you will lose most of your hair within just years and end up looking bald and 10-20 years older.
5 Likes
I have ordered a nocturnal erection tracking device because the PSYOP about finasteride got to me ![]() .
.
So I’ll be measuring nocturnal erection before and after finasteride. I’m unsure how long the baseline should be. It makes sense to care about erectile function, I guess from an evolutionary perspective as well. It’s pretty childish to not do so on the preventative side of things I guess.
@ AmyK any suggestions on how long is needed to establish a baseline before initiating a treatment with for example ED as a possible side effect? Anything else I should know?
4 Likes
I’d measure a baseline for two weeks and that should be enough to get a good idea about frequency and firmness of erections.
And, remember that topical finasteride or dutasteride are also options for hair growth. There’s still some systemic absorption but we see higher DHT concentrations at the scalp with topical - and fewer systemic side effects. Good luck.
5 Likes
I just take tadalafil 5mg 2-3 times a week for good measure, though even off them for a few weeks I don’t feel any difference.
2 Likes
@ AmyK - Thanks
@ Virilius The very small risk for priapism from tadalafil scares me like @Dr.Bart, especially if used in people with otherwise normal erectile function increases the risk. Tail risks basically. But of course nothing is risk free and there is risk vs. reward trade off.
1 Like
How did it go? Did you do your experiment?
1 Like
I would love to analyze that 2%, my gut tells me that they were not athletic types.
There is so much political correctness in medicine regarding obesity it’s hampering the progress.
My middle eastern neighbor who happens to be pulmonary/critical care doctor did not mince words when I asked him about the COVID patients in his ICU during worst time of the pandemic circa early 2021 - “they are all obese” he said.
5-ARIs, such as finasteride and dutasteride, reduce the amount of dihydrotestosterone (DHT) in the body by blocking the enzyme that converts testosterone to DHT. This results in higher testosterone levels
Adipose tissue is the primary source of estrogen production in the body after menopause. In men, obesity can lead to a decrease in testosterone levels and an increase in estradiol levels. This can create a cycle where more fat is deposited in the abdomen, which leads to more testosterone being converted to estradiol, and so on
5 Likes
At my worst weight, I had erection issues years before even knowing what finasteride was or even being on any supplement/medication. Maybe finasteride retrocausally caused those lol
3 Likes
I had dermatitis from the topical version, common side effect. This is why often they will add hydrocortisone 1%, which I don’t think it’s a good idea long term.
Systemic 5-alpha reductase inhibitors also effective against BPH and reduce chances of prostate cancer. They also may actually reduce chance of heart disease.
Anyone with existing obesity and/or significant vascular disease should stay away from 5-alpha reductase inhibitors IMO unless there is a clear indication as directed by an urologist.
4 Likes
The FirmTech TechRing constrain venous return so I waited for the Bryan Johnson Adam Health one instead, and then I didn’t care so much about hair loss since it is not imminent for me. I don’t think I’ve lost hair.
Either way we can already now fully simulate 3D environments with Google Veo 2, etc, soon appending to mixed reality filmed by for example a Quest 3 headset available now, and in two years we’ll have full photorealistic holographic AI partners with a LLM since curve is exponential. If someone needs to satisfy their desires which seems to be wanting to get rid of negative valence.
So balding doesn’t matter that much with a hyperoptimized virtual partner. For evolutionary continuation can just use artificial wombs or surrogate, but I dunno when lifespans are infinite.
It looks mostly interesting to me for immortality reasons, maybe a connection with the eunuch longevity. I didn’t know people didn’t like balding. I never thought about it much before.

1 Like
Got a couple of data points for balding and intelligence - Joe Rogan and Albert Einstein.
3 Likes
Sounds like a lot of fun ![]()
5 Likes
It’s obviously not enough, but just as a rough guess, if you look at bodybuilders who are taking high levels of androgens (in many cases, DHT derived steroids) and note the strong prevalence of heart conditions (out of control lipids, LVH, etc.), to me it wouldn’t be a surprise if inhibiting androgens promoted heart health.
1 Like
I believe the opposite is closer to truth.
1 Like
So balding doesn’t matter that much with a hyperoptimized virtual partner.
It would deal serious mental damage to me if I saw my bald self in a bathroom mirror.
1 Like
Why would that be? We already know that low testosterone and high estrogen protects women from ASCVD until menopause. Additionally, there is a strong association between balding in men and ASCVD and other various diseases. Animal studies such as Finasteride may cut heart disease risk further point to a potential causal relationship between high DHT levels and artherosclerosis.
The mice in the ITP who took 17a-estradiol but were not castrated had a significantly higher lifespan than the control mice or the castrated mice which lead the researchers to speculate that 17a-estradiol’s 5ar inhibitory effects may have caused this effect because mice without sufficient testosterone did not, in fact, have their lifespan increased.
I don’t believe testosterone in the absence of DHT is harmful (rather I believe it is highly beneficial to prevent frailty) and it is unknown whether it is sufficient to block only 5ar type 2 or if 5ar type 1 also needs to be inhibited to get a possible lifespan-increasing effect.
6 Likes
Older men with lower T levels have higher risk of ASCVD and ACM. Meanwhile, men in the “mid-range” for T tend to do better. Low DHT was also linked to greater mortality, suggesting that balanced androgens overall might help keep the heart healthy. But like you confirm if your T is too low, you might miss out on benefits like better muscle strength, energy, and potentially healthier blood vessels. In short there probably is a “sweet spot” for T and DHT, rather than letting them fall too low (or go too high).
3 Likes
Could also be a reverse causality cause of sedentary and overweight men having lower testosterone levels while having more risk factors for ASCVD. We really need some rcts regarding TRT (+5ari) vs placebo incidence of heart attacks and strokes.
Low DHT was also linked to greater mortality, suggesting that balanced androgens overall might help keep the heart healthy.
Was it low DHT in particular or low DHT AND low testosterone?
In short there probably is a “sweet spot” for T and DHT, rather than letting them fall too low (or go too high).
T should be on the higher end while DHT can be a reasonably low levels imo.
5 Likes