Not that you want to take it this far, but…
2 Likes
Thank you for the clarification
2 Likes
Libido is mostly formed by the effect of testosterone. So I think that lowering DHT should not affect libido too much, maybe it may have a psychological effect. But finasteride 1mg once a week can significantly reduce the 5 alpha reductase enzyme activity in the hairy tissue, which is enough to solve baldness. Also DHT is important for the development of external genital organs in the fetus, child and during puberty, but it does not seem to have much of a function after maturity, because testosterone already does its job. From this point of view, DHT, like mTOR, is an unnecessary legacy after maturity.
4 Likes
The only way 5 alpha reductase inhibitors could cause issues with libido if the resulting increase in testosterone is converted to estrogen, which seems to be more of an issue in obese people.
Of note, I remember when I first tried finasteride 1 mg PO QD in my 30s my libido shot up so much to a point of being uncomfortable (like being 17 again), I had to reduce my dose to 0.25 mg.
Now at 50 I have a full set of hair with few grays and I piss like a race horse. If it also reduces my chance of prostatic cancer, this it the best healthspan intervention known to men IMO.
7 Likes
This is happening to me. ![]() increase in libido and my testosterone serum levels seemed to double on finasteride 1mg daily. Have been taking it for 1 year (29 years old).
increase in libido and my testosterone serum levels seemed to double on finasteride 1mg daily. Have been taking it for 1 year (29 years old).
Am taking it for prostate cancer prevention and of course hair loss prevention.
8 Likes
Exactly…
Stay the course Jensen. I started at 32 years… and like me and Dr. Bart … you retain your hair, have a small prostate… a god send if you are older… might prevent prostate cancer and recent research, helps to control cholesterol in your blood preventing arthrocleurosis. WIN… WIN… WIN… and WIN!
8 Likes
the efficacy for hair loss prevention doesn’t change all that much with lower dose, you could probably get same effect for hair with 1/4 or 1/2 with less side effects… unless you enjoy them
4 Likes
Here’s why you want to take finasteride and keep your prostate small.
The prostate tends to grow larger as a man ages. When men are in their 20s, the normal prostate is about the size of a walnut. By the time a man is 40 the prostate may have grown slightly larger, and by age 60, the prostate is often the size of a lemon. Age increases the risk of prostate problems, such as [BPH]… Benign prostatic hyperplasia (BPH), also known as prostate enlargement, is a noncancerous condition that causes the prostate gland to increase in size. It’s the most common benign tumor in men and the most common prostate condition in men over 50
A large prostate can affect one’s ability to pee.
Being on finasteride for 33 years.
My prostate’s size, according to my urologist, is the size of a walnut. The same as a twenty year old male. Feeling great.
No issues!
Jason
11 Likes
Plasma half life of finasteride is 6-8 hours and tissue binding is 4-5 days. Does it make sense to consider intermittent dosing: every other or 3rd day, considering that? Any opinion on that?
3 Likes
Hormone can be pulsed dosed but finasteride is a testosterone reductase inhibitor so by pulse dosing the blocker you will allow DHT to act on your hair follicles or prostate on the off days - which will undermine your goals.
So short answer is better to take it daily… the way it was studied.
However you can try using lower doses down to 0.25 mg daily.
5 Likes
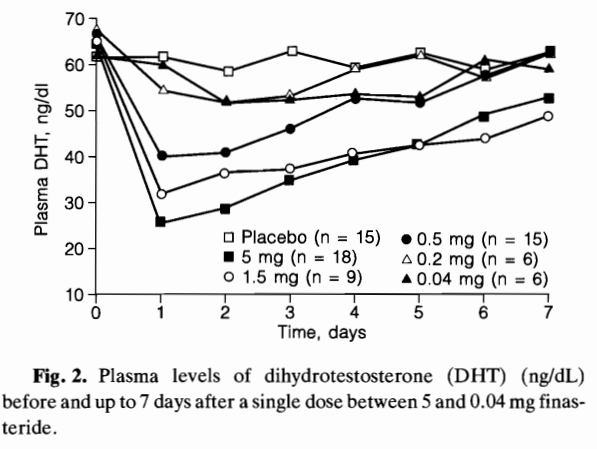
I am still tending to intermittent dosing. While finasteride has a short plasma half-life, DHT primarily acts locally (paracrine signaling) in tissues like the scalp and prostate. The graph below shows plasma DHT recovery after a single dose, but tissue DHT suppression lasts longer due to finasteride’s persistent binding in local tissues. This suggests that intermittent dosing (every 2-3 days) can effectively maintain DHT suppression in target tissues, potentially reducing the need for daily dosing while minimizing side effects.
5 Likes
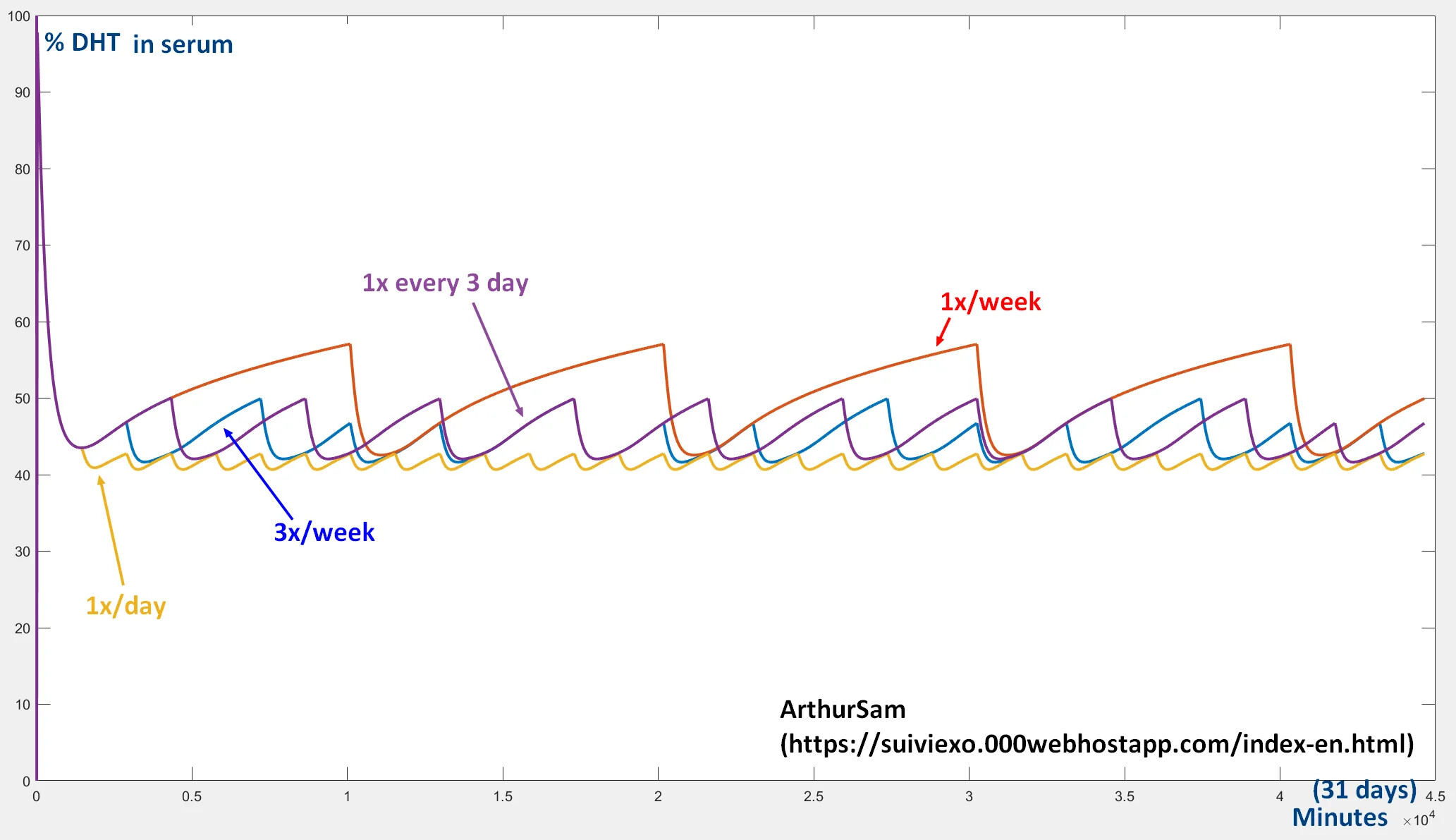
According to graph above you are still in the game and have ±57%-±43% decrease in DHT… (also found this simulation - in line with study results → link)…
5 Likes
Graphs are nice, but do you have human studies that show clinical efficacy of scalp hair regrowth or maintenance at intermittent dosing? From what I remember most studies were done with daily dosing.
2 Likes
It depends on what you’re trying to achieve. If you’re aiming for perfect DHT suppression 24/7, sure, daily dosing might seem like the gold standard. But there’s a study PubMed link where they used 2.5 mg of finasteride every 3 days in women with hirsutism and saw great results. Sure, it’s not exactly our case, but it shows that intermittent dosing isn’t just wishful thinking. If it works for hirsutism, why not for other androgen-driven conditions?
Now, back to me. My risk of prostate cancer is high due to my DNA and family history, so I need DHT suppression. But I’m also concerned about the neurosteroid disruption that finasteride causes in the brain. That study Advances in Knowledge of Androgens: How Intentional and Accidental Neurosteroid Changes Inform Us of Their Action and Role paints a grim picture of how finasteride crosses the blood-brain barrier and messes with allopregnanolone and other neurosteroids. This could be related to the effects that @DeStrider and others have experienced (+estrogen).
So, here’s where I get a little creative. Beta-sitosterol and saw palmetto can reduce DHT by 30-40%, which helps relieve some BPH symptoms (with little / no side effects). By adding 1 mg of finasteride every 3 days, we can amplify that effect, reducing DHT by around 50-60%.
The real question is: Does intermittent dosing give neurosteroids enough time to recover? That’s where it gets interesting. On the off-days, you’re giving the brain a chance to reset its neurosteroid levels (at least partially). Will it fully bounce back? Maybe not. But the risk of long-term dysregulation could be lower than with daily dosing.
So yeah, no free lunch here, but with a 50-60% DHT reduction from intermittent finasteride, along with support from natural DHT blockers, I think I can still enjoy a decent lunch — without serving my brain up for dessert.
Comments and pointing to mistakes in my thinking are highly welcome ![]()
4 Likes
Is anyone familiar with the variance of DHT suppression of topical vs. oral finasteride or Dutasteride? I tried Oral but they both killed my libido, so wasn’t worth it. But I’m thinking of trying topical versions of these drugs.
4 Likes
I take finasteride 1mg twice a week and I see great clinical benefits. It keeps my hair very strong. I have never had an erection problem. Intermittent dosing seems reasonable.
6 Likes
I think I’ll give twice a week a shot. Thanks, guys. ![]()
3 Likes
An additional concern with long-term finasteride use is androgen receptor (AR) upregulation. Studies, such as Immunohistochemical Evaluation of Androgen Receptor and Nerve Structure Density in Human Prepuce from Patients with Persistent Sexual Side Effects after Finasteride Use for Androgenetic Alopecia or Finasteride upregulates expression of androgen receptor in hyperplastic prostate and LNCaP cells: implications for chemoprevention of prostate cancer, show that finasteride can significantly upregulate AR expression in prostate tissue and cancer cell lines. This upregulation may reduce the long-term effectiveness of androgen suppression and could even contribute to higher-grade malignancies in prostate cancer.
One potential strategy to mitigate this is intermittent androgen suppression, a method used in prostate cancer management. By cycling on and off finasteride (or other 5α-reductase inhibitors), we may prevent the adaptive AR upregulation caused by constant low DHT levels. In prostate cancer treatment, cycles typically involve 6-9 months of suppression followed by several months to over a year off-treatment, based on PSA levels.
Adapting this approach from prostate cancer therapy could be an interesting option to explore for BPH management, balancing DHT suppression while potentially reducing the risk of long-term side effects. However, the exact timing and intervals for intermittent dosing remain open and require further research to determine the optimal approach.
![]()
3 Likes
I edited my question to make it more specific.
Finasteride is far too weak of an 5ar type 1 inhibitor to actually affect neurosteroid production, unlike dutasteride.
The doses of finasteride used clinically are in the range of 1 to 5 mg per day, which is far less than the doses of 30 to 100 mg/kg used in rats in the study by Lawrence et al. Furthermore, in humans, finasteride is selective for the type 2 5α-reductase isoform and less active on the type 1 enzyme that is the isoform predominantly present in the brain. This selectivity is not observed with the rat enzymes. In sum, finasteride, as administered clinically in humans, probably does not block neurosteroidogenesis sufficiently to influence seizure susceptibility under most circumstances.
Neurosteroids on the Epilepsy Chessboard—Keeping Seizures in Check - PMC (nih.gov)
Beta-sitosterol and saw palmetto can reduce DHT by 30-40%, which helps relieve some BPH symptoms (with little / no side effects). By adding 1 mg of finasteride every 3 days, we can amplify that effect, reducing DHT by around 50-60%.
Which type of 5ar do those supplements mainly affect? It would be ironic if they turn out to be stronger 5ar type 1 inhibitors than finasteride. After all, their effect on hair growth is very, very weak.
3 Likes