I have come to believe that there are very very “free lunches” in biology - i.e. where you can get some sort of benefits without any corresponding harm.
Most things are trade-offs. Inflammation is bad, except for all the times when it’s actually important. Oxidative stress is bad, except for the functioning of your immune system. Living in a city is bad (pollution etc) except when it’s good (rapid access to hospitals).
So with fish oil, just looking from principles and not even thinking about studies, I can’t really see strong logic supporting mega-dosing in healthy people as some sort of preventative measure. To believe that means you believe that fish oil/omega-3/DHA/EPA is some sort of “super fuel” where you provide more and it’s beneficial. Or that everybody is somehow deficient and it needs to be corrected. However, we have documented harms of high doses, such as atrial fibrillation.
On the other hand, there are studies out there showing positive data. The PISCES trial reports results that would seem like total bullshit if they weren’t published in NEJM (Hazard ratios in the 0.5 to 0.6 range). So clearly, DHA+EPA supplementation is at least bioactive and does something.
Lastly, there are huge conflicts of interest in this field. Bill Harris is one of the main guys, and the whole omega-3 index thing is his baby. So Rhonda and others are his disciples and help spread his message.
So for me personally (and otherwise healthy person, some CVD risk, and very very low baseline fish consumption), I take 1g per day. I go for a high-quality supplement (Nordic Naturals), and I store it in the freezer. This is basically a “cover the bases” logic so that, in theory, I do not end up deficient. However, I don’t expect this dose to provide any measurable benefit, but I also don’t expect it will cause harm. I would feel uncomfortable not taking any fish oil, since I would be consuming very little marine omega 3 (seafood allergy), but I also wouldn’t increase the dose due to the known risks.
With the current evidence, that’s pretty much the best I can do.
PISCES is interesting, I didn’t know about it, thanks for sharing: Fish-Oil Supplementation and Cardiovascular Events in Patients Receiving Hemodialysis 2025:
- “daily supplementation with fish oil (4 g of n−3 polyunsaturated fatty acids [1.6 g of EPA and 0.8 g of DHA])”
- “The rate of the extended primary end point that included noncardiac causes of death appeared to be lower in the fish-oil group than in the placebo group, with a hazard ratio of 0.77 (95% CI, 0.65 to 0.90).”
It’s among “adult patients receiving maintenance hemodialysis”, though. That’s a very specific population. Can we generalize to the overall healthy population?
Also, see: Interpreting the PISCES trial on fish oil in hemodialysis patients: lessons on trial design, biological exposure, and outcome measurement 2026, which concludes: “If omega-3 therapy is contemplated in such contexts, several principles may help guide its use: Prefer formulations achieving substantial EPA exposure (≥1.6 g/day or EPA: DHA ≥ 2:1).”
1g per day of EPA? DHA? Mix?
What are your thoughts on the papers below?
- VITAL-DEP (18 353 participants, 5.3 years): Effect of Long-term Supplementation With Marine Omega-3 Fatty Acids vs Placebo on Risk of Depression or Clinically Relevant Depressive Symptoms and on Change in Mood Scores: A Randomized Clinical Trial: “Depression risk was significantly higher comparing omega-3 (651 events, 13.9 per 1000 person-years) with placebo (583 events, 12.3 per 1000 person-years; hazard ratio [HR], 1.13; 95% CI, 1.01-1.26; P = .03).”
- “fish oil had an insignificant and in some cases negative effect on mice in the ITP”: Omega 3 makes me depressed: why? - #32 by matthost
- The shift in the fatty acid composition of the circulating lipidome in Alzheimer’s disease 2024: “Higher levels of docosahexaenoic acid in plasma were associated with a greater rate of MCI-to-AD progression.” (of course, could only be due to disruption in the transport of DHA from plasma to CSF / deficiency in DHA transporters across the BBB but still a risk)
- Dietary docosahexaenoic acid (DHA) downregulates liver DHA synthesis by inhibiting eicosapentaenoic acid elongation 2024
- Higher docosahexaenoic acid levels lower the protective impact of eicosapentaenoic acid on long-term major cardiovascular events 2023: “Higher levels of EPA, but not DHA, are associated with a lower risk of MACE. When combined with EPA, higher DHA blunts the benefit of EPA and is associated with a higher risk of MACE in the presence of low EPA.”
- Eicosapentaenoic acid reprograms cerebrovascular metabolism and impairs repair after brain injury, with relevance to chronic traumatic encephalopathy 2026: “EPA reprograms endothelial metabolism, impairing vascular repair and remodeling. EPA-driven neurovascular instability promotes tauopathy and cognitive decline.”
Actions speak louder than words: he hasn’t published papers on DHA supplementation for 12+ months and seems to now be looking at ALA supplementation instead: α-Linolenic acid-rich diet boosts docosahexaenoic acid levels and restores lipid balance in the brain parenchyma and vasculature of APOE4 mice
His latest paper on omega-3 supplementation concluded: Designing Newer Omega-3 Supplementation Trials for Cognitive Outcomes: A Systematic Review Guided Analysis 2024
A total of 24 articles met the inclusion criteria. In 5 of the 24 studies reviewed, supplementation with n-3 PUFAs improved cognition. All four trials in persons with AD reported null outcomes. Most of the n-3 PUFA studies in cognitively normal individuals or participants with mild cognitive impairment were null, not powered to detect small effect sizes, or selected participants without dementia risk factors.
We recommend that newer n-3 PUFA supplement trials targeting AD prevention be personalized. For the general population, the null hypothesis appears to be correct, and future interventions are needed to identify and test dietary patterns that include PUFA-rich food rather than supplements.
On Twitter/X as of Dec 2024, he was still recommending 1 mg/day of a mix of EPA + DHA + DPA (interestingly, not DHA only!) but he did not answer my questions and left Twitter altogether: https://x.com/ADssx/status/1904659149750702156
- VITAL-DEP is a 5.3y study and found an increased risk of depression (HR 1.13): Omega-3 Supplements May Increase Risk of Cognitive Decline, Scientists Warn - #81 by adssx
- 2y is long for a trial. And even imaging did not find anything.
- What kind of evidence would be needed for you to change your mind? For me, it’s easy: Mendelian randomization + high-quality RCT showing benefits. We kind of have that for EPA-only supplementation for depression + in people with high Tg.
Crazy results, right? Often with supplements, one of my first questions is whether it actually does anything. But at least for fish oil, we do have these very high quality trials showing biological effects at doses that are feasible for us to take.
But you’re right, I don’t think the PISCES findings can generalise to the otherwise healthy population who is trying to prevent disease. (That was kind of my point that most of these trials are in sick people, not healthy people trying to "optimise). I work closely with a nephrologist, and we chatted about the PISCES trial and he said the results are incredibly impressive, but you have to remember that these are very sick people. We also both noted the curve for serious cardiovascular events (Figure 1A) start to diverge almost immediately after commencing treatment. After only 3 months you can see the two lines and confidence limits clearly separate. That’s pretty interesting, telling us that there is some sort of potent effect which happens very quickly. If you look at Fig 1B, the event-free survival curves also separate relatively quickly, with the biggest uptick between 1.0 and 1.5 years.
And hey, at least the placebo wasn’t literally harmful like in some previous studies haha!
1g per day of EPA? DHA? Mix?
The exact product I take is Nordic Natural ProOmega 2000. But I take 1 capsule, which would mean:
1,075mg total
562mg EPA
438mg DHA
In triglyceride form, which supposedly is better.
I was aware of all of them, thanks to your previous posts. However, I just can’t really make any sensible evidence-based decisions here, based on how I can interpret these studies and relate them to my own circumstances. So I come to my personal viewpoint which is that I don’t eat any seafood and I do believe that omega-3s are something we should consume. I do have some CVD risk, thanks to genetic factors and high Lp(a). However, I am not mega dosing or going for 'optimisation" etc. I reckon 1g per day is enough to do something, but not too much to do too much, haha. Not very scientific I fully admit. My aim is to cover bases and try to avoid any sort of deficiency. I also take my fat-soluble astaxanthin and vitamin D at the same time.
That’s a very good point: we do have trials showing massive benefits in some populations (PISCES EPA-dominant in hemodialysis, and REDUCE-IT, JELIS, and EVAPORATE for EPA-only in high Tg).
I agree with your reasoning. My only question is: why DHA? I dug a bit more and can’t see any benefits to DHA supplementation. Here are more recent papers, all of relatively good quality, and they all point to DHA being useless or even detrimental (as adding DHA to EPA blunts the benefits, and the plasma EPA/DHA ratio seems to matter):
Both dietary and blood levels of n-3 FAs are negatively associated with RDW in individuals with prior MI. The findings are consistent with the hypothesis that RDW may play a potential mediating role in the association between n-3 FAs and mortality risk. Given that a high RDW signifies an inflammatory state and abnormal erythrocyte function, the observed association between higher blood levels of n-3 FAs and improved prognosis after MI aligns with potential underlying mechanisms: attenuated inflammation and enhanced erythrocyte function.
Our findings suggest that n-3 FAs may confer cardiovascular protection, although recent large-scale trials have yielded conflicting results [9,10,11]. Notably, unlike EPA, DHA has been hypothesized to lack cardiovascular benefits—or even to attenuate the protective effects of EPA [38]. Consistent with this hypothesis, our mediation analyses indicated that EPA-specific biomarker (eEPAp) accounted for a larger proportion of the association with clinical outcomes than DHA-related biomarkers, potentially explaining the inconsistent evidence across studies, which often differ in their EPA-to-DHA ratios. Although the EPA-to-DHA ratio (EDR)—a measure of their relative abundance—was not statistically significant in our analysis, it showed a consistent inverse association with mortality. This aligns with emerging evidence suggesting that the EPA:DHA balance, rather than absolute levels alone, may influence cardiovascular risk. Intriguingly, all participants exhibited low EDR values, indicating a population-level relative deficiency of EPA compared with DHA. Whether selectively increasing EDR through EPA-predominant supplementation confers additional clinical benefit remains an open question warranting focused investigation.
(poke @John_Hemming, above paper on RDW, you might be interested)
EPA showed a significant inverse association (OR 0·907, 95 % CI 0·824, 0·998, P = 0·045); ALA, DPA and DHA were NS. […] Dietary n-3 intake, particularly EPA, was modestly and inversely associated with depression severity.
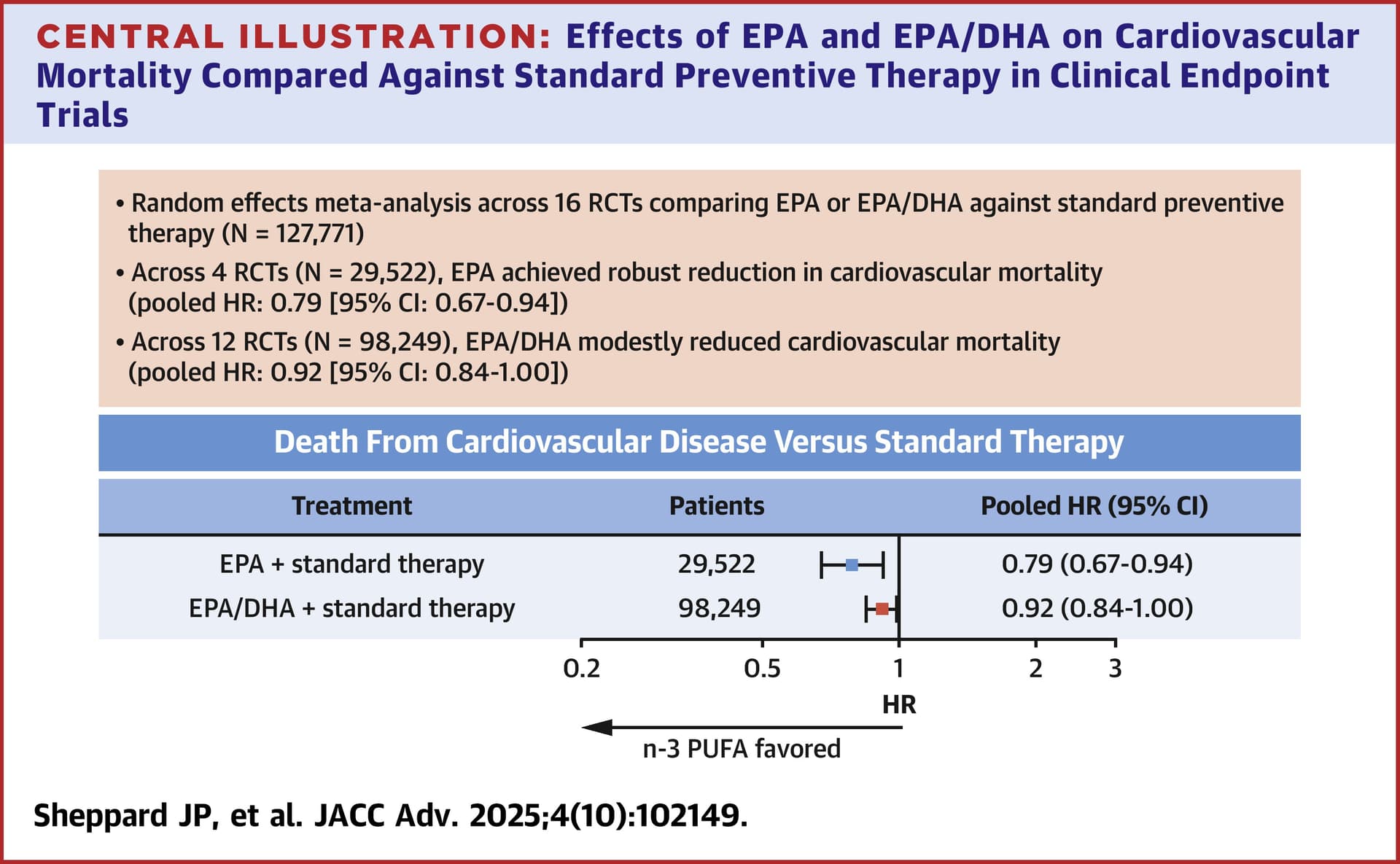
EPA lowered incident CVD-attributable mortality in RCTs investigating its use for primary or secondary CVD prevention. Relative to EPA, benefits reported with EPA/DHA were attenuated. Although more work is needed to understand these differences, EPA should preferentially be used in cardiovascular conditions for which it is indicated.
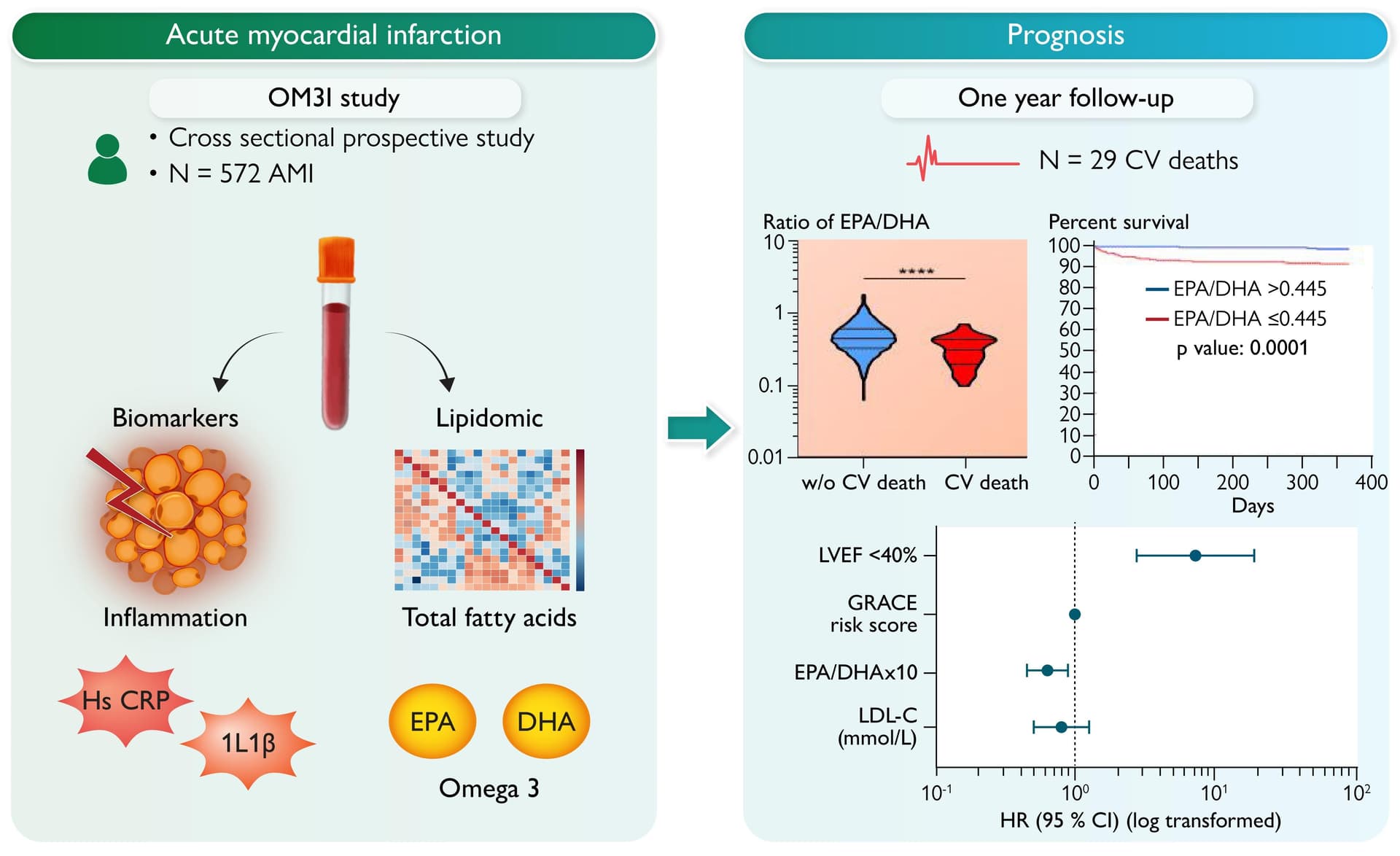
Patients who died had lower relative levels of EPA [0.47% (0.28–0.73) vs. 0.73% (0.52–1.02), P < 0.001], a lower EPA/DHA ratio [0.33 (0.22–0.43) vs. 0.44 (0.33–0.61), P < 0.001], and more elevated levels of inflammatory biomarkers, including hs-CRP and interleukin-1β. In contrast, DHA levels were not associated with CV mortality. In multivariate analysis, the EPA/DHA ratio was associated with lower CV mortality, even after adjustment for confounding factors including GRACE risk score, left ventricular ejection fraction, and inflammatory biomarkers.
So, is there a case for supplementing with DHA in 2026? For depression, the answer is a clear no to me (VITAL-DEP EPA+DHA showed increased depression, while EPA-only showed benefits). For CVD, EPA-only seems better. Even PISCES was 2:1; maybe EPA-only would find even better outcomes! And, for cognitive health, after PreventE4, it’s very hard to make a case for DHA supplementation as PreventE4 was the perfect trial design recommended by “pro fish oil” people: DHA only, high dose, long duration, fairly large trial, with vitamin B, in a population with low baseline, with imaging + cognitive measurements, etc.
Thank you for all of your analysis. I have decided to switch from 2:1 EPA/DHA to EPA only. The main reason I take it is to reduce triglycerides, which I have found to have a noticeable effect.
Any thoughts on this brand?
https://hk.iherb.com/pr/carlson-elite-epa-gems-1-000-mg-120-soft-gels/13839
https://alz-journals.onlinelibrary.wiley.com/doi/10.1016/j.jalz.2010.01.013
https://www.sciencedirect.com/science/article/pii/S0022316622029467?via%3Dihub
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(21)00185-1/fulltext
There are too many to count.
Beneficial effects of docosahexaenoic acid on cognition in age-related cognitive decline 2010
- Effect was small and borderline: statistically significant but not clinically suggestive.
- Benefits only in episodic/recognition memory tests, but not working memory or executive function => not a global cognition effect
- Only 24 weeks => PreventE4 over 2y used the exact same algal DHA (from Martek Biosciences, now DSM) and the exact same placebo (50% corn oil / 50% soy oil blend) and found nothing.
- A more recent trial tried to reproduce the findings and could not (and EPA better): Supplementation with oil rich in eicosapentaenoic acid, but not in docosahexaenoic acid, improves global cognitive function in healthy, young adults: results from randomized controlled trials 2021
- Note: Not fish-oil DHA but algae.
A Meta-Analysis Shows That Docosahexaenoic Acid from Algal Oil Reduces Serum Triglycerides and Increases HDL-Cholesterol and LDL-Cholesterol in Persons without Coronary Heart Disease 2012
- Meta-analysis from 1996–2011: 11 RCTs, only 485 healthy participants, old evidence, mostly short-term, no hard cardiovascular outcomes. Garbage in, garbage out.
- Note: DHA from algal oil, not fish oil.
- All they found “The pooled estimate for the change in TG concentration was −0.20 mmol/L (95% CI: −0.27 to −0.14), 0.23 mmol/L (95% CI: 0.16–0.30) for LDL-C, and 0.07 mmol/L (95% CI: 0.05–0.10) for HDL-C.”: LDL increasing by +9 mg/dL (that’s bad), TG −18 mg/dL (not clinically significant for someone with high TG), HDL +2.7 mg/dL (irrelevant) => If anything, that confirms that DHA supplementation is a net negative.
- EPA is still better: lowers TG too, but tends not to raise LDL-C. And improves outcomes (the above paper says nothing about outcomes)
- How do you explain that JELIS and REDUCE-IT found that EPA-only reduced major CV event, while STRENGTH, which was EPA+DHA, was stopped for futility (no significant MACE benefit and more AF)?
Higher dose docosahexaenoic acid supplementation during pregnancy and early preterm birth: A randomised, double-blind, adaptive-design superiority trial 2021
Yes, there’s a stronger case during pregnancy. But I don’t think @relaxedmeatball is pregnant?
So if the above are the strongest evidence in favor of DHA supplementation, then is DHA still going to the trash (unless you’re pregnant).
Bro, I’ve told you, there are countless studies on DHA. This single paper alone is reason enough for APOE-ε4 carriers to supplement with it. There’s honestly too much research to even list.
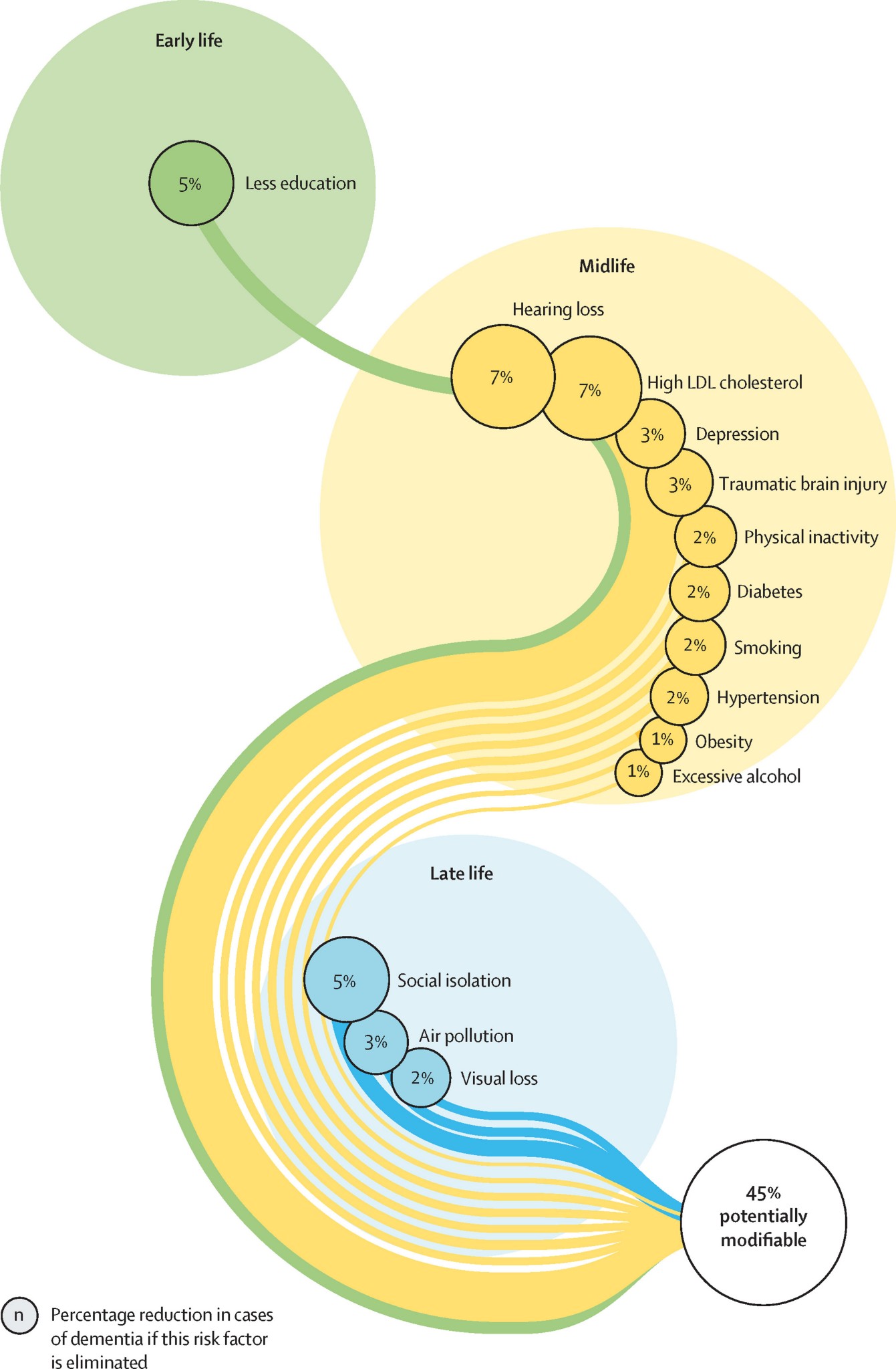
Depression is one of the causes of dementia (Lancet Commission):
DHA supplementation causes depression.
So of course APOE-e4 carriers shouldn’t supplement with DHA.
Also it’s a paper published in MDPI Nutrients which is a low-quality borderline predatory journal: Nutrients (journal) - Wikipedia
Until September 2018, the editor-in-chief was Jonathan Buckley of the University of South Australia. In 2018, Buckley and the other nine senior editorial board members resigned, claiming that MDPI “pressured them to accept manuscripts of mediocre quality and importance.”[1] The current editors-in-chief are Maria Luz Fernandez (University of Connecticut) and Lluis Serra-Majem (University of Las Palmas de Gran Canaria).[2]
Also: when the editor-in-chief in from a shitty university in Spain it’s never a good sign.
So another paper that can go to the trash. If the research were good it would have been published in a better journal.
That’s not really the scientific consensus.
Damned the more I dig into that paper the worse it gets… It’s authored by William Harris, President and CEO of OmegaQuant, which sells the Omega Index test… ![]()
![]()
![]()
In any case even if that paper were good and correct: it’s longitudinal not causal. High RBC DHA may be a marker for eating fish, healthier diet, higher socioeconomic status, better vascular health, supplement use, or other confounders. They did not adjust for income or wealth (but education which is of course linked).
Similarly we know that exercise can increase RBC DHA while smoking and alcohol can decrease it. So RBC DHA might just measure healthy habits. They did not adjust for that either.
https://onlinelibrary.wiley.com/doi/10.1002/gps.5707
Several recent clinical trials have shown that docosahexaenoic acid (DHA) supplements have a significant effect on cognition in cognitively impaired older adults.
There’s a reason the scientific community is conducting so much research on DHA and APOE-ε4. The only reason these clinical trials exist in the first place is because a mountain of evidence suggests DHA is beneficial. Your claim that APOE-ε4 carriers shouldn’t take DHA is absolutely not the consensus. More importantly, your logic that ‘DHA causes depression, depression causes Alzheimer’s, therefore APOE-ε4 carriers shouldn’t take DHA’ is deeply flawed, and you probably don’t even realize it.
DHA dose and timing also matter. ApoE4 carriers may need higher DHA doses because they β-oxidize DHA at greater rates than non-carriers
Effects of DHA on cognitive dysfunction in aging and Alzheimer’s disease: The mediating roles of ApoE 2024
That’s a Chinese narrative review: so what?
Do you realize that this is the protocol of the failed PreventE4 trial?! https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5456486
The main author, Hussein Yassine, has since then published what is indeed the “scientific consensus”: Designing Newer Omega-3 Supplementation Trials for Cognitive Outcomes: A Systematic Review Guided Analysis 2024
A total of 24 articles met the inclusion criteria. In 5 of the 24 studies reviewed, supplementation with n-3 PUFAs improved cognition. All four trials in persons with AD reported null outcomes. Most of the n-3 PUFA studies in cognitively normal individuals or participants with mild cognitive impairment were null, not powered to detect small effect sizes, or selected participants without dementia risk factors.
We recommend that newer n-3 PUFA supplement trials targeting AD prevention be personalized. For the general population, the null hypothesis appears to be correct, and future interventions are needed to identify and test dietary patterns that include PUFA-rich food rather than supplements.
Nutrients, MDPI, published by “ingridestrada1113@hotmail.com” and “nwitz99@gmail.com” (Nick Norwitz) => LOL
CONCLUSIONS AND RELEVANCE
High-dose DHA supplementation in APOE4 carriers before the onset of AD dementia can be a promising approach to decrease the incidence of AD. Given the safety profile, availability, and affordability of DHA supplements, refining an ω-3 intervention in APOE4 carriers is warranted.
I don’t know if you’re serious and I’ll give you the benefit of the doubt but you really need to learn how to read papers chronologically and check the authors. This was submitted in 2016 by Hussein Yassine. Yassine indeed wrote in this paper:
High-dose DHA supplementation in APOE4 carriers before the onset of AD dementia can be a promising approach to decrease the incidence of AD. Given the safety profile, availability, and affordability of DHA supplements, refining an ω-3 intervention in APOE4 carriers is warranted.
Then he went on to conduct the PreventE4 trial to confirm the above promising approach.
This promising approach failed: PreventE4: A Double-Blind Placebo Controlled Clinical Trial Testing High Dose DHA in APOE ε4 Carriers Before the Onset of Dementia (Lancet! and Yassine as well of course)
This led the exact same Yassine to rightly conclude what is the current scientific consensus: Designing Newer Omega-3 Supplementation Trials for Cognitive Outcomes: A Systematic Review Guided Analysis 2024
For the general population, the null hypothesis appears to be correct.
Of course in 2016 DHA supplementation looked like the very promising approach. That’s why I supplemented with it. But a decade is a long time in academia! And the evidence is now that DHA supplementation is either futile (dementia, CVD) or detrimental (depression, LDL).