I do Carlson’s Elite Omega-3 once a week, and Pharmepa Restore Pure EPA, twice a week, wild caught salmon from TJ’s once a week - FWIW, never noticed any effects of any kind. Peter Attia uses Carlson’s I believe.
I wonder if the issue for you is the omega-3, or some kind of interaction between the omega-3 and something else you’re taking. Perhaps googling for “omega-3 interactions” might be interesting?
I suffered from depression for years, on and off. I have no idea why, but it’s not attitude. It’s biochemical. My attitude has never changed. It stopped years ago when I got the my first sperti vitamin D lamp.
It’s hard to cover all your skin with one little lamp in 5 minutes, so I have 3 now and use them simultaneously after my shower when naked. I also use NIR photobiomodulation at the same time, which they say is the wrong time of day to do it but that’s when I’m available. I think if you use it you can probably use the DHA too.
By the way, some people suggest that DHA might be at best neutral and at worst detrimental and that for cardiovascular health only EPA matters:
Omega-3 fatty acids and cardiovascular prevention: is the jury still out? 2023: “The differences in these trial designs have led some to believe that combining EPA + DHA may down-modulate the beneficial clinical effects of EPA treatment alone; however, the differences in these trial findings may be explained by other reasons (below). The EPA monotherapy studies may show benefit, but there are concerns about adverse metabolic effects of the mineral oil comparator. The differences between the EPA and EPA + DHA trials may be attributable to (a) insufficient dose, (b) O3FA species, (c) the comparator, (d) the patient population and, most importantly, (e) the omega-3 index was not measured and thus the opportunity to determine treatment effect and adequacy of tissue dosing was lost.”
Effect of omega-3 fatty acids on cardiovascular outcomes: A systematic review and meta-analysis 2021 “The meta-analysis showed higher RR reductions with EPA monotherapy (0.82 [0.68–0.99]) than with EPA + DHA (0.94 [0.89–0.99]) for cardiovascular mortality, non-fatal MI (EPA: 0.72 [0.62–0.84]; EPA+DHA: 0.92 [0.85–1.00]), CHD events (EPA: 0.73 [0.62–0.85]; EPA+DHA: 0.94 [0.89–0.99]), as well for MACE and revascularization. Omega-3 FA increased incident AF (RR, 1.26 [1.08–1.48]). EPA monotherapy vs. control was associated with a higher risk of total bleeding (RR: 1.49 [1.20–1.84]) and AF (RR, 1.35 [1.10–1.66]).”
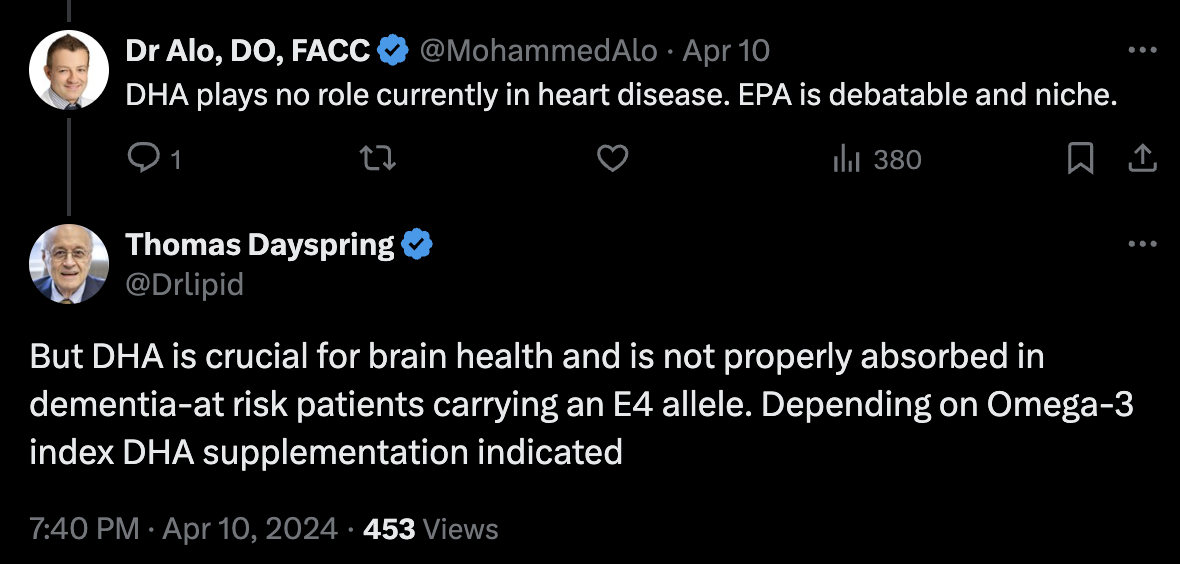
The evidence is unfortunately weak for DHA and brain health. Cardiovascular health is an important factor for brain health so if EPA is better for that, I’m team EPA until proven otherwise.
I guess it’s the usual “Everyone is different”. Have you ever measured your omega-3 index? If you go at the end of the report and calculate your DHA/EPA ratio, what is it? Mine is 4 (4 times more DHA than EPA). But I don’t know if this has any kind of clinical significance (most papers only focus on the omega-3 index and this 2022 OmegaQuant blog post says the jury is still out on EPA vs DHA)
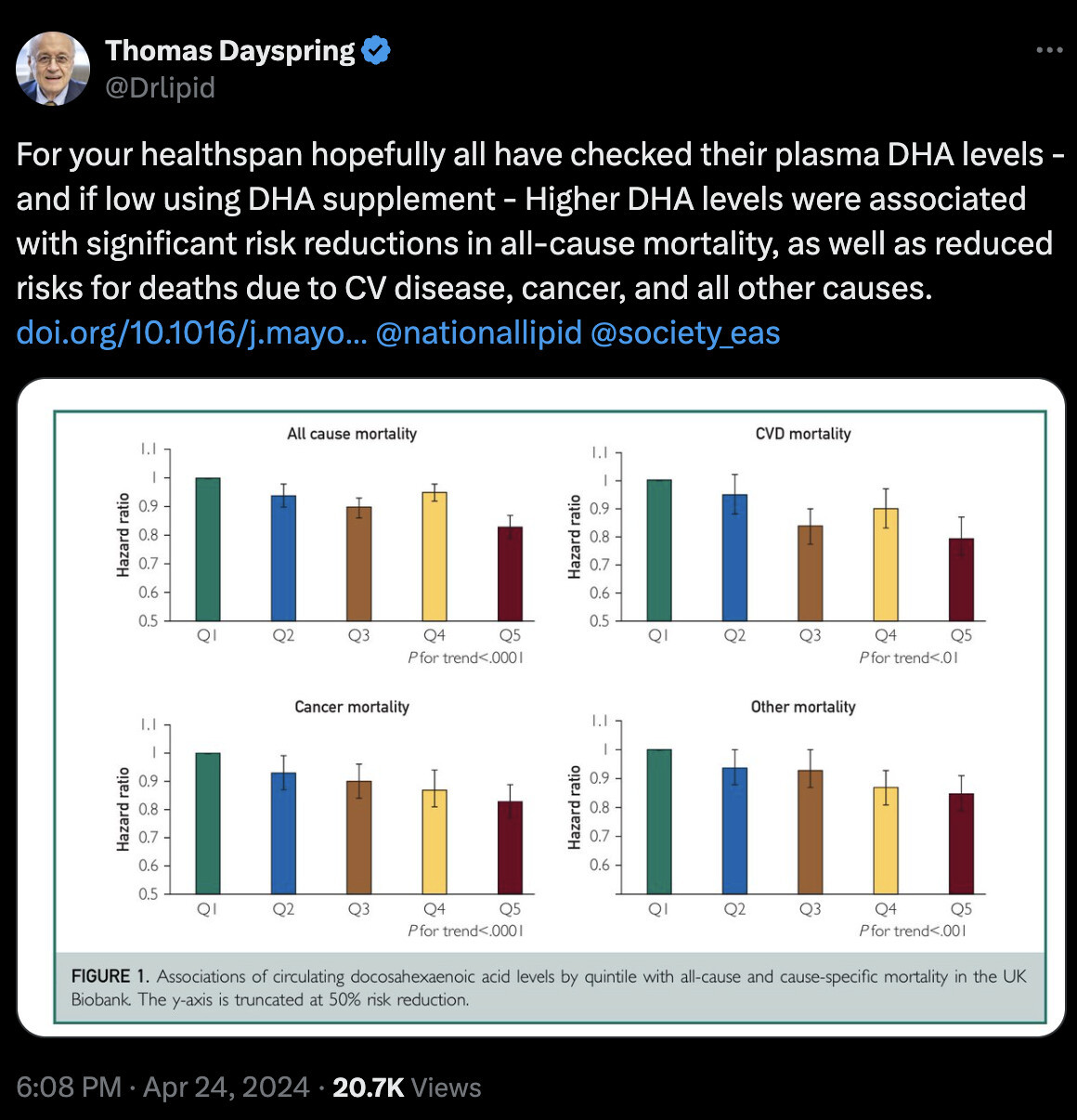
We focused on DHA in this meta-analysis as it was the only specific omega-3 fatty acid level available in the UKBB because nuclear magnetic resonance technology was not able to reliably measure plasma EPA in this population. Blood levels of DHA but not EPA show strong statistically significant inverse associations with risk of Alzheimer disease. On the other hand, EPA monotherapy has been shown to be effective in reducing risk for major adverse CV events. No similar trials of DHA monotherapy have been undertaken. Levels of EPA+DHA have been shown to be inversely associated with mortality; however, whether EPA or DHA is more strongly associated with improved life expectancy remains uncertain.
What’s interesting, here are my OmegaQuant results (before starting omega 3 supplementation):
Omega-3 index: 5.37%
EPA: 0.49%
DHA: 3.06%
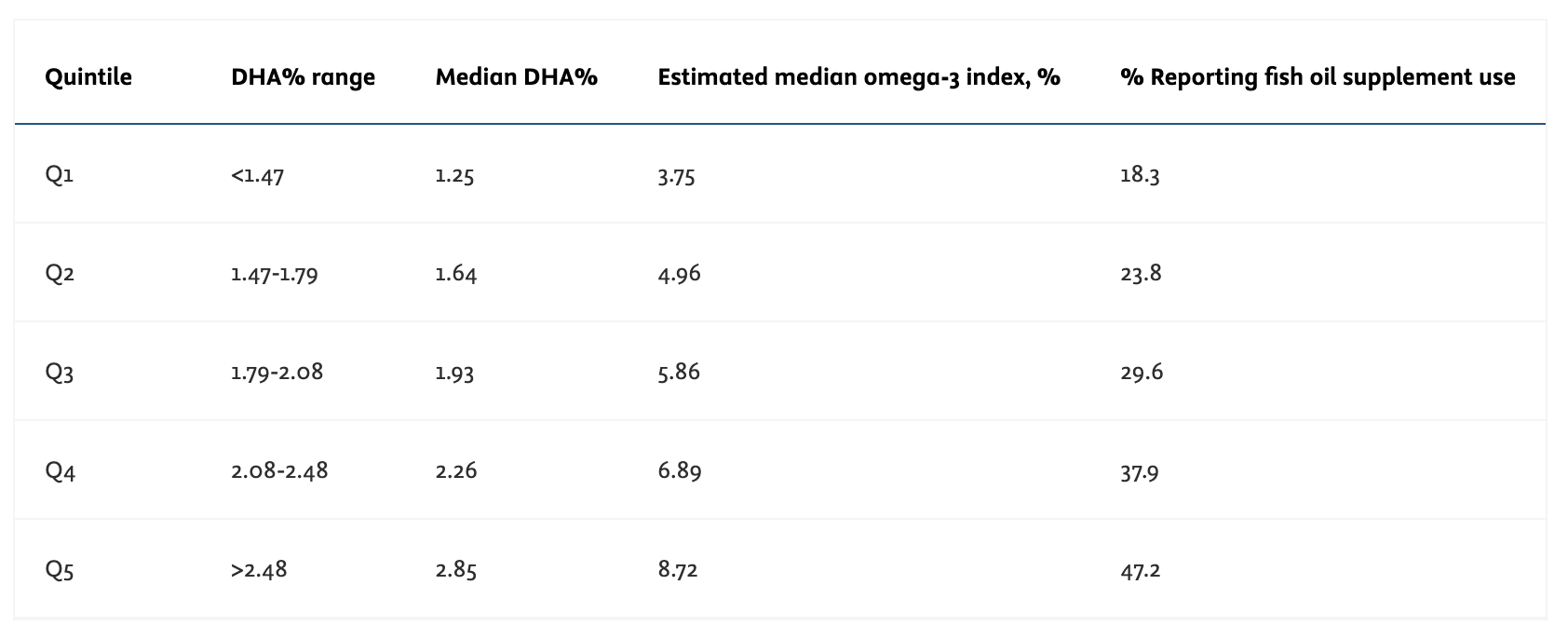
So if I understand correctly, I’m already well above the top quintile for DHA (2.48%) but my omega-3 index is average (“the mean intake of DHA+EPA in the United States is only approximately 100 mg/d and the mean omega-3 index is approximately 5.4%”). Could it be that people like us @Davin8r@hamida_abdenour who experienced depressive symptoms from DHA already have high DHA? Have you done the test? If true, then one should supplement in EPA and DHA according to the test results to reach DHA > 2.48% and omega-3 index > 8%? Wdyt @DrFraser?
I goal for 8% Omega 3 index in those with no ApoE4’s and 10% in those with an ApoE4.
AI’s review of does EPA convert to DHA, which is relevant - is very little. So it is important to do the OmegaQuant Plus rather than basic to see DHA and EPA. I usually am using the Omega Check through Lab Corp, which is $69 and goes to Cleveland Clinic, takes a month, but gets all the details on everything.
Eicosapentaenoic acid (EPA) can convert to docosahexaenoic acid (DHA) in the human body, but this conversion is generally limited and inefficient. The process involves a series of enzymatic reactions that elongate and desaturate EPA to form DHA. However, the conversion rate is typically low, often less than 5% in most individuals, and some studies suggest it may be even lower, around 0.1-1% 2.
Several factors can influence this conversion efficiency. Gender plays a role, with women generally having slightly higher conversion rates than men. Age can also affect conversion, as efficiency may decrease with age. Genetic variations can impact an individual’s ability to convert EPA to DHA, and dietary factors, such as a high intake of omega-6 fatty acids, can inhibit the conversion process. Additionally, certain health conditions may affect conversion efficiency.
Due to the low conversion rate, it is often recommended to obtain DHA directly from dietary sources or supplements, especially for individuals with increased needs, such as pregnant women or those with specific health conditions. Both EPA and DHA are found in fatty fish, algae, and some fortified foods. Supplements often contain both EPA and DHA in varying ratios.
While EPA has its own health benefits, DHA is particularly important for brain and eye development and function. The limited conversion of EPA to DHA underscores the importance of obtaining both fatty acids through diet or supplementation when indicated. Understanding these metabolic processes helps in making informed decisions regarding omega-3 fatty acid supplementation to achieve optimal health outcomes.
True but your body only converts what it needs… and everyone reacts differently and this might be a better path for you. I take hemp oil because I do not want any mercury from fish oil. That is why it is simple for me.
You can use algae based supplements to avoid mercury, but also brands like Nordic Naturals make sure there is no mercury in their product. The problem with hemp oil is that it is indeed rich in ALA, but very little of this gets converted to EPA/DHA, especially if you have significant omega 6 fatty acids in the diet.
It isn’t cheap, but I’d suggest an Omega 3 index would be in order and if >8% with Hemp awesome! However, my experience is that almost everyone will be suboptimal without direct supplementation or a diet very rich in fish.
I got this kind of depressing mode with a sensitivity to some emotional ideas on 2 occasions basically when i started taking omegas 3 (EPH+ DHA) and the second period was after retaking them after stopping for 21 days because i was on work mission and i forget to bring some omega3s with me and in both situations i noticed the effects were less if i take them at night so maybe it’s transient period when the brain get high levels after consumption?