The patients took doxycycline for thirteen months, not five weeks.
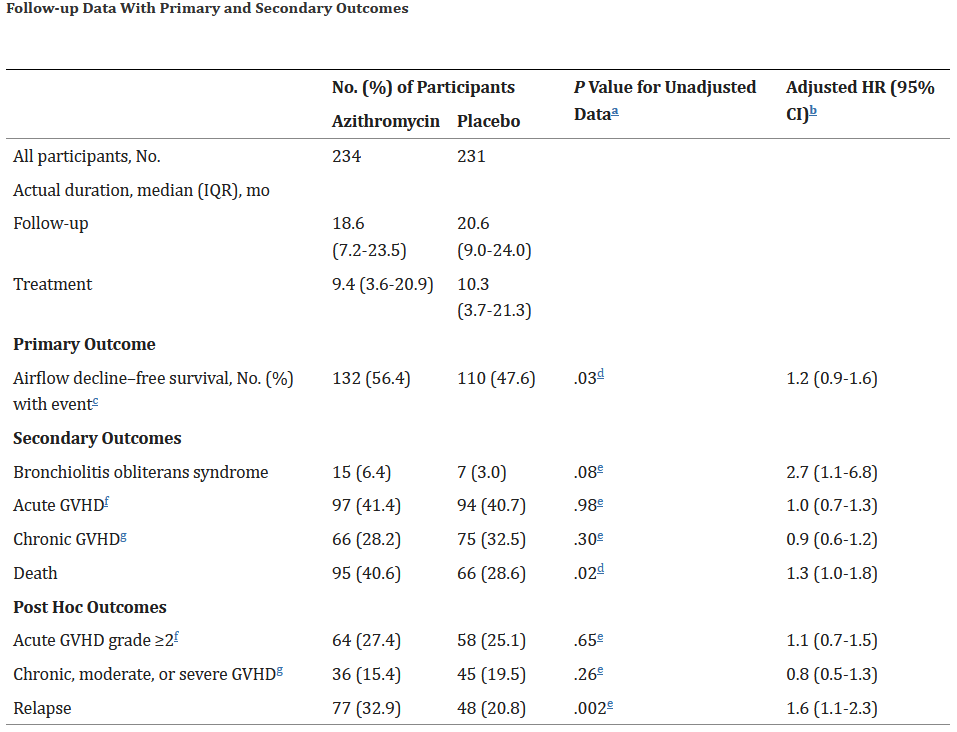
243 patients were to receive > > azithromycin (250 mg) 3 times weekly for 2 years; 237 patients were to receive placebo for two > years, starting at the time of conditioning regimen. The immunomodulating effects of > azithromycin therapy were evaluated when used for the long term prevention of BOS.
Results: The ALLOZITHRO study treatments (azithromycin/placebo) were terminated on the > 26th December 2016 i.e. at thirteen months after completing recruitment
" One of the best-characterized and simplified methods to measure senescence in vitro and in vivo is the β -galactosidase (β -Gal) assay, which measures β -Gal activity expressed by senescent cells that can be detectable at pH 6.0 by immunohistochemistry.118,119 This marker was shown to be present in senescent cells only, and not in presenescent or quiescent fibroblasts or keratinocytes, and is a reliable marker for senescent cell detection in several organisms and conditions.92,120–125 Demonstrating the correlation between senescence and aging, senescence-associated β -Gal (SA-β -Gal) was shown to increase in an age-dependent manner in skin samples of human donors.118 Despite being (together with cellular morphology) one of the most common marks of senescence, β -Gal activity has shown background reaction to senescent-independent conditions such cell contact inhibition or high cellular confluence.126"
If you are worried about senescent cells, I recommend you try the best two anti-senescent senomorphics available to PREVENT senescent cell formation.
These are:
Rapamycin
Taurine
It is much easier to prevent stem cells from forming than to remove them later.
As for senolytics, the gold standard is still Dasatanib + Quercetin.
If you take Rapa and Taurine as well as Dastanib + Quercetin every 2 months, you shouldn’t have to worry about senescent cells at all. I feel that this is already overkill.
Sometimes doing too much is worse than doing nothing at all.
I suppose if I were to do this, such a test would be a really good idea and it is good to know what to test for. Thanks.
The thing that concerns me is how much does this cost? And I assume we would at least need a before and after test. I suppose that is the real cost of doing this.
Review the long video interview of Michael Lisanti.{it is posted on this thread] He speaks of comparing “Dasatanib + Quercetin” to just Azithromycin and the
Azithromycin by itself out preformed the “Dasatanib + Quercetin”
On top of Dasatanib cost more and is a chemotherapy agent.
Azithromycin is much safer and cost a fraction of Dasatanib.
One of the paper published,
Azithromycin and Roxithromycin define a new family of “senolytic” drugs that target senescent human fibroblasts
…“we see that Azithromycin preferentially targets senescent cells, removing approximately 97% of them with great efficiency. This represents a near 25-fold reduction in senescent cells. Finally, we also discuss our current results in the context of previous clinical findings that specifically document the anti-inflammatory activity of Azithromycin in patients with cystic fibrosis - a genetic lung disorder that results in protein mis-folding mutations that cause protein aggregation.”…
Here’s a paper done in vivo by the NIH on the effects of dasatanib on senescent cells in adipose tissue. D+Q targets senescent cells in adipose tissue which is where most senescent cells are found. They are also likely the most damaging of all senescent cells.
The study you reference is in vitro and funded by a company with a financial stake. I’ll take an in vivo study by an unbiased entity any day over one with a conflict of interest.
Azithromycin may work well, but there’s only so many senescent cells you can destroy. At one point, it may become overkill.
Because senescent cells can take weeks to months to develop and do not divide, and because even eliminating only 30% of senescent cells can be sufficient to alleviate dysfunction in preclinical studies [3,5,7,9,23,24,28,[32], [33], [34], [35], [36], [37]], D + Q is as effective in mice if administered intermittently, for example every 2 weeks to a month, as continuously, even though D and Q have elimination half-lives of only 4 and 11 h, respectively [38,39]. This is consistent with the point that, since the target of senolytics is senescent cells, these drugs do not need to be continuously present in the circulation in the same way as drugs whose mechanism of action is to occupy a receptor, modulate an enzyme, or act on a particular biochemical pathway, at least in mice. Intermittently administering D + Q effectively circumvents any potential off-target effects due to continuous receptor occupancy or modulation of an enzyme or biochemical pathway.
Here is another paper that talks about azithromycin, dasatanib + quercetin and other senolytics:
Although there is a lot to recommend it, there are several papers that show that Azithromycin, in some cases, interferes with cardiac rhythm. As someone who has had cardiac arrhythmia (atrial fibrillation) I’m very skittish about using it, which is a pity as I’ve already bought it. Looks like it will be put on the back burner for a while. Maybe a safer alternative will be found. (Sigh…)
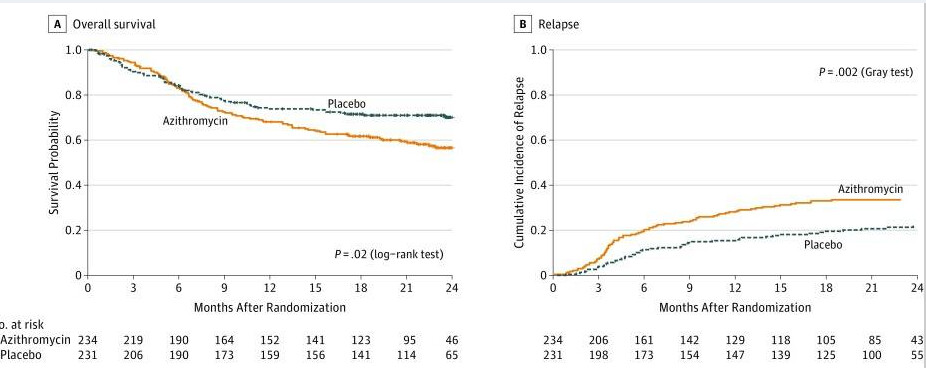
What about that study showing azithromycin use associated with significantly higher relapse of cancer, posted earlier by AnUser in this thread, is that not a cause of concern? (Maybe only relevant for those with cancer in remission like me…?)
I was quoting the study they referenced. Not everybody is anti DAV. I do support its trial by members. But as I indicated above, I am leaning towards the approach of Rmun and bslm for subdosing.
If you are removing senescent cells, you probably won’t notice much. The only thing I have heard you may be able to notice is any adipose tissue may become softer.