@DrFraser do you use bisphosphonates in your practice?
They call a 10-day fast “short term fasting”. What would a long fast look like? I’m not participating in any of their concentration camps!
3 Likes
Right now these agents aren’t on my list of things for longevity. In regard to their indications they are approved for, I’m not impressed on outcomes, as they don’t seem to do much for the life threatening outcomes (hip fractures), have excess osteonecrosis of the mandible … among other outcomes.
With the gerotherapeutics part of this - I’ve not done the deep dive yet and I’ve seen some items come across that look favorable.
I guess the reviews are in isolation, and I think there are a host of drugs/interventions I’d put up first and then is there a benefit to adding these to other agents that I have a preference for? We probably won’t know this for decades, if ever.
Anyway - I must do my research on these, and eventually there will be a blog on these. I may have a favorable or unfavorable disposition on them for aging. For osteoporosis, they get a neutral or thumbs down right now from me.
5 Likes
Wow. I have no idea…?
Thanks for all this color!
Do only do diet and resistance exercise - or any other meds you consider in an osteoporosis reversal strategy?
?
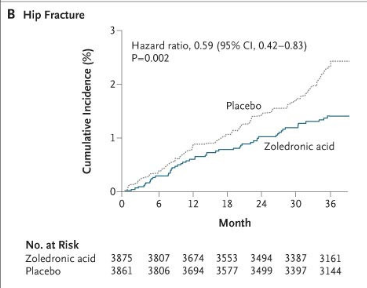
Treatment with zoledronic acid reduced the risk of morphometric vertebral fracture by 70% during a 3-year period, as compared with placebo (3.3% in the zoledronic-acid group vs. 10.9% in the placebo group; relative risk, 0.30; 95% confidence interval [CI], 0.24 to 0.38) and reduced the risk of hip fracture by 41% (1.4% in the zoledronic-acid group vs. 2.5% in the placebo group; hazard ratio, 0.59; 95% CI, 0.42 to 0.83). Nonvertebral fractures, clinical fractures, and clinical vertebral fractures were reduced by 25%, 33%, and 77%, respectively (P<0.001 for all comparisons). Zoledronic acid was also associated with a significant improvement in bone mineral density and bone metabolism markers. Adverse events, including change in renal function, were similar in the two study groups. However, serious atrial fibrillation occurred more frequently in the zoledronic acid group (in 50 vs. 20 patients, P<0.001).
There were no spontaneous reports of osteonecrosis of the jaw. From a search of the trial database of adverse events, which was followed by expert adjudication, two cases of potential osteonecrosis of the jaw were identified (one in the placebo group and one in the zoledronic-acid group). In both patients, delayed healing followed surgical manipulation, and both cases subsequently resolved with antibiotic therapy and débridement. A similar search for and review of osteonecrosis of the hip or knee revealed seven cases (three in the placebo group and four in the zoledronic-acid group).
4 Likes
@Neo My first line choices are weight bearing exercise with impact, and hormone normalization, appropriate vitamin D/K2. There will be individuals who have severe disease and a decision down this route or monoclonal agents like Prolia (denosumab).
@A_User You make the points that I was taught in my traditional training. It is important to look at NNT also. This is a fairly balanced article on this topic here.
The real-world benefits of reducing vertebral fracture risk, especially radiographic fractures, remain uncertain. Vertebral fractures are associated with future fracture risk, chronic pain, and functional decline; reducing the risk of these factures is assumed to reduce risk of associated complications. However, the range of clinical trajectories of vertebral fractures is wide: some fractures cause severe pain and disability, others cause no symptoms at all. Some clinical trials distinguished between symptomatic and asymptomatic fractures, but adjudication of symptoms was usually a one-time binary determination without additional data about severity of pain, disability, or need for clinical intervention. In the Fracture Intervention Trial, a randomized placebo-controlled trial of alendronate in postmenopausal women with low bone mass, one arm of the trial examined outcomes among women with new vertebral fractures. The frequency of back pain and back-related disability were not significantly different between women treated with alendronate and placebo.
Perceptions of the benefits of bisphosphonates depend on how risk reduction is presented. In general, use of relative risk reduction leads to more favorable views of treatment benefits compared with other risk-based statistics like absolute risk reduction. When the baseline risk is low, use of relative risk alone is likely misleading.
According to the review conducted by the ACP, the relative risk reduction of hip fractures with bisphosphonate treatment for at least 3 years is 36%; however, the absolute risk reduction is only 0.6%. Framed as number needed to treat, 167 patients need to be treated for 3 years to prevent one hip fracture. One study of patients attending an osteoporosis clinic found that presentation of treatment benefits as absolute risk reduction significantly decreased the number of patients who would consider treatment compared with use of relative risk reduction.
I thought Dr. Greger did a reasonable job discussing this topic here.
Overall, I’ve not come to a firm opinion yet in regard to longevity with these drugs. Clearly osteroporosis, frailty and sarcopenia are predictors of premature death … naturally if you can work on all of these the outcomes would seem better. Some people won’t follow a plan to improve, and you have the options to use these drugs or not, and with various thoughtful reviews not being as glowing, as we need to look at actual quality of life changing fractures. For example, having to treat 170 people for years to have 169 of them not necessarily benefit and 1 benefit - but then there are side effects. That would probably be the harshest review and the benefits are overstated - and possibly the harms/side effects can also be overplayed.
5 Likes
I think RR is the best we got so we can extrapolate beyond short trials for compounding gains, and for every risk category and treat causes of disease for prevention. Statin denialists use the same argumentation to persuade people to not treat LDL with absolute risk and NNT.
I don’t trust everything Greger says, he keeps people away from pharmaceuticals despite adherence being high, and mention they can try his low adherence, low evidence, protocols. Adherence for zoledronic acid is 80% for three full years and evidence is high quality. I have not done any research on this topic, but my prior is that Greger is wrong.
3 Likes
He says “In other words, taking these drugs has not been convincingly shown to prevent fracturing your hip in the first place.”, when he is referencing this.

A meta analytic summation of 1 RCT and 5 observational trials.
Basically he decided to ruin a RCT although it was only trending towards significance, by adding a bunch of relative garbage studies, and create the equivalent of a mortgage-backed security.
For the part of prior hip facture, he decides to cite the RR for the meta-analytic summation with 7 RCT’s and 9 observational trials:
![]()
Rather than the summation of the RCT’s which any evidence based practitioner would prioritize, and which decreases the RR more than the summation with the relatively garbage studies.
![]()
He is not doing a good job. He is extremely biased, as shown in the “mistakes” he is making.
This is one example and it’s tiring Greger is such a quack.
3 Likes
Why do vegans take Dr. Greger seriously again? At least carnivores have the excuse that Dr. Salad Dino looks fit and healthy while he spouts bs.
2 Likes
I took Fosamax (bisphosphenate) for many years, to my regret. These drugs work by stopping osteoclasts from removing old non functional bone cells. The non functional cells remain and so then the DXA scan looks like there is more density, but the quality of the bone is, as one endocrinologist I spoke to said, more like saltines. In some women, the rate of resorption increases greatly after menopause and therefore these women might benefit from slowing that resorption. But this is not true for all women. They only way to know whether you are resorbing too much bone is by taking bone marker (simple blood) tests. Many years after having taken and stopped Fosamax I finally was given these tests and found that my rate of resorption was not too low. But, the real issue is that the osteoblasts are not making sufficient new bone as we age. The parathyroid analogs such as Forteo and Tymlos goose the osteoblasts into making new bone, but these positive impacts disappear shortly after stopping the drugs (you can only take them for two years). After that the bones return to the state they were in before starting the parathyroid drugs – unless-- you take a bisphosphenate or a monoclonal drug such as Prolia, pretty much for the rest of your life.
There really are no good osteoporosis meds. I decided to take raloxifene, a SERM (Selective estrogen reuptake modulator) because it is both protective against breast cancer and is effective at preventing vertebral fractures. But it has no impact on hip fractures.
7 Likes
Thanks very much for posting this.
I saw something on youtube which said basically this (obviously the most reliable source possible ![]() but it does make sense). I’m glad to find out there are bone marker tests, though without a way to treat the situation it’s not as useful as one could wish. I have my ears twitched for therapies that improve osteoclast activity.
but it does make sense). I’m glad to find out there are bone marker tests, though without a way to treat the situation it’s not as useful as one could wish. I have my ears twitched for therapies that improve osteoclast activity.
1 Like
Deborah - you properly articulate the concerns of many here. Working as an ER physician, the Orthopedists that take care of hip fractures … my chats with them are that the one on bisphosphonates have abnormal bone structure. It is a long standing change is my understanding. As this isn’t my number one area of interest - but is important, I’ve not yet dug in to sort out what I’m going to do outside of standard guidelines. Luckily, I have no patients currently on these drugs, because we are choosing other options, and few of my patients have osteoporosis. There has to be a place where these are sensible.
@A_User There is a problem with RR reduction. Let’s say I have an awesome drug that decreases your rate of Acute Myeloid Leukemia a condition that affects 4/100,000 per year. So my drug has a 50% rate reduction. So we treat 100,000 people with my drug for a year to prevent 2 cases. Who knows the toxicity and cost of my drug … but the RR reduction is 50%. Number Needed to Treat however is 50,000 people treated to prevent 1 case. Not a good statistic.
Regardless, I’ve not got a horse in this race right now, and will follow guidelines for the most part … but there is certainly reason for pause, and I need to dig in and spend the 10-15 hours to really look at the data to have a more nuanced approach.
I however think it isn’t as clear cut as the data might have one think.
2 Likes
This does not include compounding effects, meaning taking a drug for a year prevents prevents 2 cases in the first year, then 5 in the next and so on. Or for example lowering lipids for 15 years early in life to prevent cardiovascular disease in late life.
The NNT in the study I posted was 11 for vertebral fractures and 48 for hip fractures, within the study context. If it’s the same as for lipids the absolute risk reduction will be the same as the RR reduction on future lifetime risk.
I used to work as a medical statistician before medical school … the incidence of the disease is critically important, a high incidence serious disease with an intervention that only makes a 10% rate reduction has a markedly bigger impact on all cause mortality than a low incidence less serious disease with an intervention that has a much bigger rate reduction. NNT is pretty important in any decision made to decide to treat. We also need to look at what outcome we are avoiding in the NNT and how this balances with the number of people needing to take the drug who don’t end up with benefit, but end up with risk/cost/side effects.
The extent of costs, side effects, alternatives must be factored before looking at whether Rx.
Naturally picking patients at high incidence of the given adverse outcome is important, and one’s ability to correctly pick those patients so that we treat patients at highest risk (which unfortunately we don’t do that great of a job predicting who will get spinal or hip fractures).
Irrespective, the decision to prescribe lipid medication is a more simple one than this - and I have very few patients who would meet any criteria to consider giving these medications.
3 Likes
Come on, this is just nit-picking. Neither the results of the RCT or the OS trials were statistically significant, per the diagrams you just noted. His statement “taking these drugs has not been convincingly shown to prevent fracturing your hip in the first place” remains true, per the data presented.
Wait, now you’re expecting him to selectively dismiss the RR for the summation of the RCT+OS studies and just present the RR for the RCTs alone because that suits your pro-pharmacy narrative marginally better? And HE is the one who is biased?
“The RCTs were strictly designed, conducted, and
reported, and the OSs employed multivariate statistical
analysis to minimize potential confounding. The quality of
all included studies was regarded as high.”
Is your strategy here to just get so far into the weeds that nobody will actually get in there to check your work? Actually reading through the review paper (which took some doing to find the full text), re-listening to Dr. Greger’s video, and taking into account Dr. Fraser’s comments above, I think Greger has it right.
2 Likes
Because a RCT is a better study design and doesn’t have confounding to a similar extent, so it is better able to detect causality.
Greger is wrong and knowingly so on so many topics, so it’s likely he is wrong on this one too.
1 Like
Sure, but there’s also the “totality of evidence”. Even if RCTs (if done well) are weighted more heavily than observational trials, it doesn’t mean one has to completely throw out the results of well-done observational trials, especially when both showed significant results in secondary prevention of hip fractures.
We’ll have to agree to disagree, then. Nobody’s perfect, but I think he’s right on the vast, vast majority of topics. And the statement “knowingly” implies that you have psychic powers.
4 Likes
I love that you are on the board! You challenge me to think and evaluate what I do and recommend. Your points are well made. I’ll continue to refine my approach.
5 Likes
Novel formulations of oral bisphosphonates in the treatment of osteoporosis
“The cardiovascular effects of bisphosphonates are debated, with data from animal studies (using higher dosages than used in human studies) suggesting potential cardiovascular protective effects due to reduced atherosclerosis in response to bisphosphonate therapy [27–30]. This is supported by a limited signal from a trial of risedronate which showed a protective effect of 2.5 mg dose for cardiovascular mortality (RR 0.69, 95% CI 0.49–0.99) and stroke mortality (RR 0.36, 95% CI 0.17–0.78), though this effect is caveated by the fact that there was no significant effect at the 5 mg dose or on the incidence of coronary artery disease [31]. Indeed, meta-analyses have shown no significant associations (either protective or adverse) between bisphosphonates and cardiovascular death, adverse cardiovascular outcomes, myocardial infarction or stroke [32] and this is echoed by long term, prospective database studies [33].”
“Oral bisphosphonates play a key role in the treatment of osteoporosis and the amelioration of fracture risk. They are, however, hampered by adverse events, particularly affecting the upper gastro-intestinal tract, which reduce patient adherence and persistence. Effervescent alendronate and gastro-resistant risedronate seek to improve adherence by simplifying the complex dosing rigmarole and reducing upper gastro-intestinal adverse events. Data from trials and real-world data are encouraging with regard to the benefits of these medications both clinically and from a health economic perspective.”
2 Likes