-
Graph with life expectancy per dollar spent, per capita, is not healthcare system related, otherwise they need a robust analysis showing that it is. It’s drug overdoses, obesity, and firearms related. What is modulated by the healthcare system the U.S is actually doing better (like cancer screening).
-
Disease increase can be because of changing criteria, more screening, less stigma, etc, which are artifacts and not real increases.The only organic increase in chronic disease is obesity and obesity-related. What’s artifacts are things like increases in autism, ADHD, and celiac.
-
The solutions the report present for artifacts or organic increases of disease are either not presented, quite poor, or take solutions off the table that will actually work.
-
We have solution for the real problem, which is obesity (food has become like crack), and not only has RFK Jr. taken it off the table, he has discouraged it.
-
40% having a chronic disease is an error, it’s 37.5% in the source they cited, it’s even explicit.
-
The increases in disease among children is not obesity adjusted.
-
Diabetes prevalence increases with increase in obesity over time, but asthma doesn’t.
-
It’s true childhood obesity is increasing and is a problem, and diabetes is also increasing, which is as expected because obesity is.
-
They are presenting a “crisis of autism”, and you might have some ideas why they have the inclination to want to present this, as an “organic crisis”…  cough “vaccine cause autism”
cough “vaccine cause autism”
-
Diagnosis are increasing, but as an organic increase, Avi disagrees.
-
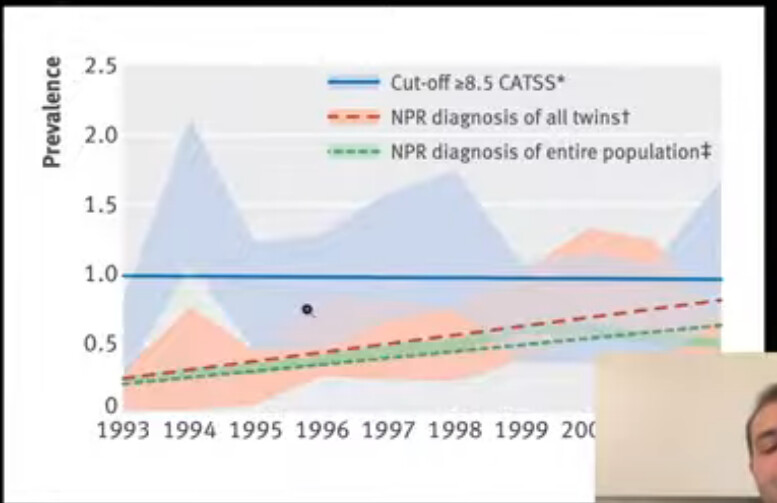
Graph shows that different diagnostic changes happen simultaneously as increase in prevalence over time occurs. It was very hard to receive an autism diagnosis in the past (behaviors associated with both low and high IQ were required). It was diagnosed as e.g schizophrenia instead. It was inappropriately strict in the past. Recent DSM-5 has decreased new diagnosis.
-
If the underlying criteria for a diagnosis stays the same over time, but the diagnosis prevalence increases, that means it’s an artifact. (e.g BMI staying the same, but obesity increasing). If there’s a corresponding increase for the underlying symptoms of autism with the prevalence of diagnosis the rates are increasing organically and is not an artifact.
-
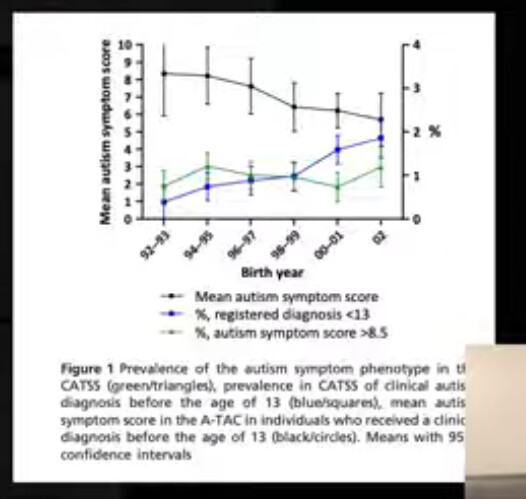
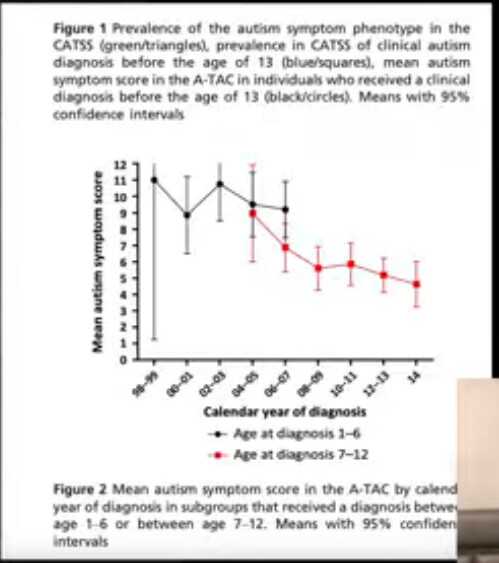
Data for the symptoms of autism over time doesn’t exist for the U.S, but for other countries it does, and the symptoms are flat over time from 1993-. It’s very strong evidence it’s an artifact.
-
Autism symptoms may have even decreased over time.
-
It does not mean that it’s overdiagnosed, it can be a good thing, but it does not need any solution.
-
Similar pattern for ADHD, there’s a counter hypothesis, plausible mechanisms, and evidence for it. The burden is on them to show that it’s not an artifact.
-
For cancer… we have become better at screening, detection, imaging, blood tests, diagnosis, technology overall. Childhood cancer all-cause mortality and and deaths have decreased over time.
-
It’s WILD that they are this incompetent and pushing this to the general public and policy.
-
Depression and anxiety increases are not artifacts, and Avi agrees, but RFK does not offer any good solutions, and might actually suggest viable solutions as problems (although not as bad as with obesity).
-
Some allergies are organic increases (not celiac), and not artifactual, and increase in atopic dermatitis is real because more severe AD is increasing.
-
It’s a success of the healthcare system to diagnose more celiac disease, there’s nothing here, we’re just doing a good job. This is a monstrosity of a report. Catching more cancer in stage 1 is a good thing. You can frame it like there’s more people getting cancer. Dangerously misleading.
-
So what’s causing the increase in childhood chronic disease? (Most of the increases aren’t real at all, and is evidence of things going well - us improving). Obesity we already knew we should talk about, but RFK’s solutions are trash.
-
Not the “CHEMICALS!”, and “MEDICATIONS!”
-
Interesting that saturated fat is presented in a negative connotation in the report, for all the KETO’s out there who worship RFK.
-
Yes UPF’s are designed to increase caloric intake, food companies do that to sell product. UPF’s as a heuristic are bad, not as a rule, protein powder is classified as UPF but it’s a healthy food. A better heuristic is hyperpalatable food, not UPF. Typically a combination of salt, sugar, and fat, which are added to make a food hyperpalatable and increase caloric intake. It overrides satiety mechanisms for whatever reason.
-
You can make something hyperpalatable without it being UPF, you can take a steak and put salt and sugar on it, and add a little fat, and make it hyperpalatable. It will induce overeating but not be UPF.
-
The chemicals argument (including microplastics), is unpersuasive and very weak.
-
Pervasive technology use argument is reasonable. But sloppy argumentation by moving from children to young adults, without a specific good inference.
-
MAHA report claims that effect of long term ADHD medication use converge without using it with behavioral modification, but they got to do whatever they wanted later in the study, and medication was used in the behavioral modification group.
-
The conclusion from the study they cited itself: “It would be incorrect to conclude from these results that treatment makes no difference or is not worth pursuing” They say it would only work long term if they actually took the medication.
-
Imagine how embarassing this is, if this was something Biden released, you would be losing your shit right now. You would rightfully call him sleepy joe, demented, and all of those things. That he can’t even read a citation.
-
This is a government report, that has been completely botched. The study is represented in the exact opposite way. The conclusion is that it works, if you stop taking it it doesn’t work, no shit, what is presented “that it doesn’t work long term”. Complete misrepresentation of the study.
-
I don’t know if they didn’t read it, if they had an AI read it, but this is really bad. This is gross incompetence.
-
Anti-depressant use vs. psychotherapy is a false dichotomy, they aren’t mutually exclusive, and anti-depressants aren’t off the table since depression rates are increasing. Some of these aren’t in-depth empirical debunks, just basic philosophy.
-
Off-label is not inappropriate use, including for antipsychotics in children, it could be because there wasn’t enough money to get FDA approved for that condition (e.g because it went generic). FDA approval requires RCT’s, and not e.g cohort studies showing benefits. We prescribe off-label medications all the time for good reason.
-
They made an error with the number with regards to “unnecessary” antibiotic use, was it an LLM that at the time couldn’t calculate the correct number? (They consistently make errors in favor of their position). It’s less than 30%, not 35%.
-
Yes there’s an association with antibiotic use and conditions, but it is also true that getting infected is also associated with different conditions. This needs to be addressed. For example, if someone had polio, and it was treated with antibiotics, then RFK comes along and say “wow, if you treat these people with antibiotics, they get paralyzed” Not adjusting for antibiotic indications which may cause the chronic health outcome.
-
If someone has sepsis, we treat them with antibiotic, and sometimes it is false positive. It is damaging to not treat, it is expected. You have to make the case that less than 30% unnecessary antibiotic use is bad. We don’t have the perfect knowledge to make it 0%. Stack that up against the risk of erroneously not treating an infection
-
The report is full of this: “increase by X”, big number, but not where numbers are coming from and if it’s bad or good.
-
Conflict of interest “corporate capture” is not a flat out reason to dismiss evidence, in fact, in many cases it’s the only way you’re going to get evidence. Motivated study design is good, it’s not inappropriate, because it allows for the statistical power design to find effects that a non-biased research might miss (their money is on the line). Lies, damn lies, and statistics and such are not good, however. Which is why you look at the methodology and the results. When research funded by industry is more positive to industry, it can be because of good reasons, like making sure to study something with adequate power to find effects, like some grant researcher might’ve overlooked. It’s not necessarily malicious.
-
RFK has not articulated whether the funding sourced results goes in alignment with them is malignant or benign. The same can be said for a food that RFK likes to defend which is red meat. Either industry will fund it or you need another solution, or that the research will not be done, will you socialize the research? Taxpayers pay it? All pharma research should be funded by taxpayers? At least $100 B/yr from taxes would be needed.
Next part of the debunk will start at “A Closer Look at Ultra-Processed foods” of the report.
")

")