Thanks. Nothing new? Lithium Supplementation - #386 by adssx
We now know that they should have tried lithium orotate: Lithium Supplementation - #333 by adssx
Thanks. Nothing new? Lithium Supplementation - #386 by adssx
We now know that they should have tried lithium orotate: Lithium Supplementation - #333 by adssx
They’re actually citing the Nature paper in their conclusion:
Alternative formulations of lithium, such as lithium orotate, also warrant further investigation in human RCTs since lithium orotate may be effective at concentrations orders of magnitude less than lithium carbonate with much less toxicity.
FWIW, there’s also some limited but continuing research into lithium aspartate.
Yes, but if the Nature paper is correct, then aspartate (which falls between acetate and citrate per ChatGPT and Gemini) will be less effective than orotate: Lithium Supplementation - #333 by adssx
The PACC score is the “money maker” and the results weren’t available so far. But given the direction of some sub-metrics and long radio silence, it seemed likely, that is was inconclusive.
The previous trials all used Li-carbonate, as did the observational data. So it was the most reasonable version to design the LATTICE trial with in the year 2017. But given that the results are below expectations, chances are slim to find a sponsor for a larger clinical trial.
They were (number 3 on clinicaltrials.gov if you click on the link I posted back then).
Those RCTs are in progress:
Hopefully aspartate in PD will be positive and someone will try orotate…
I discovered Matt Kaeberlein takes 10mg of Lithum per day.
In his podcast thread, someone shared they are taking 5mg and sometimes 10mg per day.
I’ve been conservative in my advice to family by telling them 1mg, but perhaps I should raise that number to 5mg because we have a history of neurodegenerative diseases
That leads me here to take a poll to see what the hivemind is taking.
I also learned from some of you that SGLT2s reduce your effective dose by approximately 50%-isy, so for that reason, I personally take 6mg per day. (I assume Matt also takes an SGLT2).
Is this the sort of supplement where we should take our body weight into account? If so, it would make sense Matt take more than I do.
I’d appreciate any responses!!!
Dosage for longevity and NDD prevention is unknown. Subsequent to the lithium orotate/AD mouse AD model paper, a bunch of researchers surmised that pretty low doses would be equivalent in humans, as low as 1mg per day or even lower (elemental). Might more (say 10mg per MK) give you a better efficacy margin, nobody knows. Many things affect lithium levels including SGLT2i (which decrease levels), and telmisartan (which increases levels by conserving it). But at the levels discussed in this context (1-20 mg), there are few side effects - some people report positive effects on mood etc. - and it seems safe unless perhaps you have severely compromised kidney function.
But here’s a bit of idle speculation. What ultimately matters is outcomes. Outcomes - this is thin on the ground for humans. The epi studies of lithium unfortunately are so confounded as to be virtually useless. But look at SGLT2i. We know they severely deplete lithium. Yet there is no evidence at all that they shorten lifespan or lower healthspan or increase NDD risk. In fact there is evidence for the contrary, especially for NDDs, kidney and CVD health. The evidence for SGLT2i being health promoting is far more robust than for Li, where it’s practically absent. Yet SGLT2i get rid of lithium - if Li was so important for health, especially NDDs, you’d expect negative effects here, yet the exact opposite is true. We’ve discussed this paradox previously without resolution. And my additional wrinkle in this - hence the idle speculation - is that we know how dangerous it is to mechanistically speculate in ascribing cause and effect: what if far from the Li lowering by SGLT2i being some irrelevant side effect, it is in fact partially what is responsible for the health promoting effect of SGLT2i on kidney function? Why? Because high dose (again, we’re talking high dose here) Li is kidney damaging. And - speculation - SGLT2i is kidney protective partially because it gets rid of Li, and adding Li back in is counterproductive by obviating that benefit of SGLT2i. The SGLT2i Li lowering effect is very prominent - and it strikes me as rather bold to dismiss it as playing zero part in any health effects of SGLT2i. Is it possible that it’s irrelevant despite such an extravagant effect? I suppose so. But is it likely to be so? Hmm. Think about it. Li can be kidney damaging. SGLT2i gets rid of Li - and is kidney protective. Coincidence? Idle speculation. Meanwhile, SGLT2i health promoting effects have been robustly and repeatedly demonstrated in humans. There are no such robust demonstrations in humans for Li. So does it make sense to put back in the Li that SGLT2i is trying so hard to get rid of? When the benefits of SGLT2i are so well documented and Li not, with the additional wrinkle of negative effects of Li on kidneys (dose dependent). You may say, oh well that’s at high doses - but are you sure low doses don’t have a subclinically negative effects which are then countered by SGLT2i getting massively rid of lithium? Inquiring minds want to know. YMMV.
Of course, I am only an N=1 experience. But on the other hand, that experience is decades long.
I don’t remember exactly when I started taking lithium orotate, but it was somewhere in the mid-nineties, so I have been taking lithium orotate in dosages of 10-30 mg for ~30 years.
My experience has been positive, even life-changing. The main reason I use lithium orotate isn’t for life extension but for its mood-altering qualities. It makes me slow to anger and definitely reduces such things as “road rage”. Things that used to upset me no longer do. Perhaps best described as reducing stress and making me a more mellow person. It also reduces excess cortisol. Lithium orotate, perhaps, is better at controlling mood than life extension. If lithium orotate also has life-extension properties, that is a plus. Lithium orotate has had zero effect, as far as I can tell, on my kidney function.
For those just starting lithium orotate, it takes about 2 to 3 months for it to have any effect on mood. Lithium orotate is one of the last supplements that I would quit taking. As I have previously posted, it is in my top five supplements.
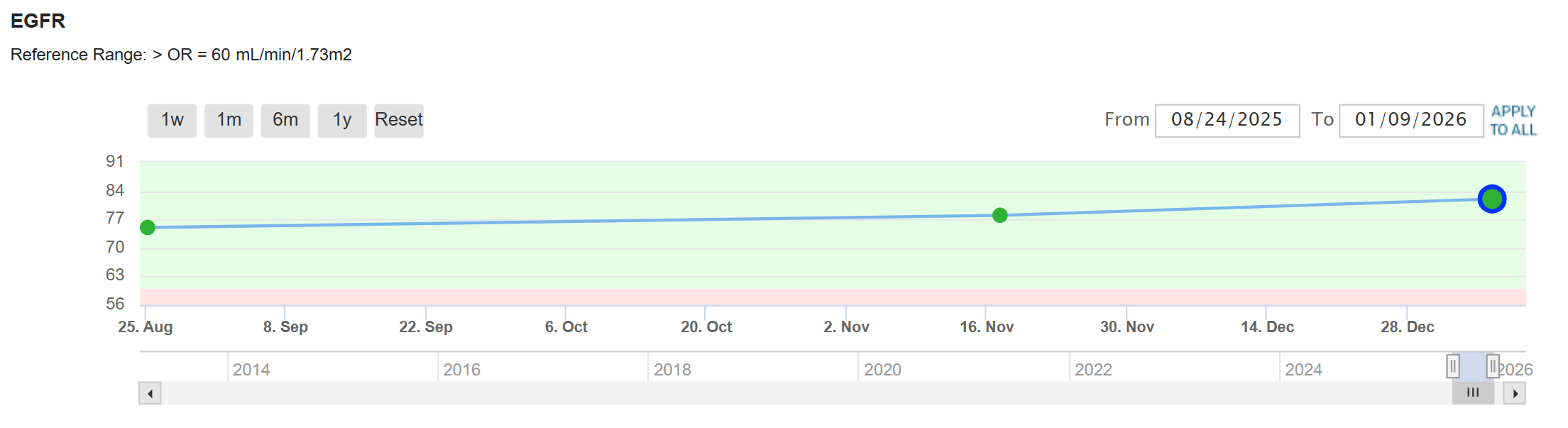
My latest eGFR was 82 mL/min, which my primary physician, a geriatric specialist, says is exceptional for someone my age.
Lithium inhibits the transport proteins for citrate into kidneys. As a citrate obssesive I think that is part of the reasons why lithium at high doses can be nephrotoxic. However, at lower levels it inibits gsk3 where I think there is value. Hence I aim for the lower than 50 mcmolar range. Hard to measure cheaply.
We know why/how SGLT2i are kidney-protective, and none of the mechanisms have anything to do with lithium, so there’s no reason to believe that lithium is involved.
Yes, of course, it’s the expected answer. I too have read the studies. My whole point here is that in medicine (and biology) we have especially good reasons to practice epistemic humility. There are literally thousands of examples of when we thought we understood the MOA of something only to later discover that it’s far more complicated, sometimes to the opposite effect. This is why in medicine we put so much emphasis on outcomes. Because it tells us “what” the outcome is in a measurable way, whereas the “why” is the mechanism, which we are far more prone to be wrong about. It’s very common to say “this medication works, though we don’t fully understand why”. Which is why I try to adopt the black box paradigm to medicine. We have inputs (the intervention), and we have the output (the outcomes), but how you get from input to output is through a black box of MOA which is opaque. Yes, in many cases we can speculate accurately as to what happens inside of the black box. But very often we don’t - we make a small change in inputs (in that we think the change is irrelevant based on what happens inside to black box), only to be surprised when the output changes too.
What are the situations when our spidey sense tells us to be careful in asserting we understand the full MOA? It’s when the effects are complex. For example SGLT2i effects are extremely pleiotropic. They affect not just kidneys, but brain and heart among other tissues. And we really do not have a full explanation of the MOA of SGLT2i positive effects on CVD for example. When it comes to kidney health, we have a whole bunch of mechanisms by which we think SGLT2i manage their good effects: glomelular hypertension, diuretic anithypertensive effects, antifibrotic, tubular hypoxia, metabolic efficiency, anti-inflammatory effects etc., and so on down the line. And that is exactly when our spidey sense should kick in. When the MOA is simple or unitary, odds are it’s correct. We see that in elegant experiments, for example with infectious agents, where the presence or absence of the agent gives the precise outcomes we observe. There is no ambiguity. That’s true of many molecules. But when it comes to many others, where the effects are diffuse and pleiotropic, all bets are off. The more ways a drug acts and along more pathways, the less confident we can be about the MOA - some of these we call “dirty” drugs, because they have such scattershot effects where we are not sure at all about the MOA or the weight of impact we can assign to any particular aspect of a multi-effect drug - which precise mechanism is more important than another.
And that’s the situation with SGLT2i. Yes, we think we understand many MOA of how SGT2i achieve their health benefits in the kidneys, but it’s actually along many pathways and we can’t be sure we’ve mapped out all of them. In such a scenario, how do we know we have not missed one, including - pure speculation - lithium disposal? Epistemic humility.
My point is not to assert that lithium disposal is part of the MOA in kidney benefits of SGLT2i. That would be the opposite of epistemic humility, lol! My point is simply to say - epistemic humility compells me to point out that the causality chain is not transparent here, and not complete. I don’t know. In that I’m not just pronouncing simple ignorance, but a more socratic one of consciously thought through skepticism, “I know that I don’t know” precisely because I have read so much of the relevant literature. More knowledge alerts you to how much more knowledge gaps there are.
To bring it back to brass tacks. I’m not saying Li is not the bee’s knees. I’m saying that settling on a good dose of LiO is dependent on an understanding of the effects. And there is a ton we don’t know about lithium in the context of longevity and health effects. Meanwhile SGLT2i are a class of medications that tell us something about lithium levels and health - even if exclusively “low levels are not necessarily deleterious to health”. But the fact that we are faced with such a paradox when it comes to Li and NDDs with SGLT2i impact tells us unequivocally that there is A LOT we do not understand here. The idea here is that we should take LiO for NDDs and brain health. Shouldn’t we understand the effects more before we can select the appropriate dose? And shouldn’t we be troubled by the existence of that paradox of SGLT2i being good against dementia in people while drastically lowering Li that in turn is also supposedly good against dementia? So which is it? Low levels, or high levels? Isn’t that relevant when trying to settle on a dose?
That was the context of my idle speculation - to say that there is too little information and that the disparate effects, including on the kidney might alert us that “that way danger lay”, and angels fear to tread - should we rush in? Again - like I said it’s pure speculation, not assertion. I don’t know. YMMV.
I would agree with that. However, I dont think it varies that much for Lithium.
I can appreciate the skepticism and epistemic humility. At this point, I’m choosing not to wait since it appears that most likely the potential benefits of SGLT2i are independent of lithium excretion. We also have to remember that the dose makes the poison. There’s no evidence in the literature that micro-doses of 5 to 10mg of lithium are at all harmful to the kidneys. The toxicity kicks in with therapeutic doses for bipolar disorder (600 to 1800mg per day).
I have the exact same experience. Lithium orotate 1 mg has been life-changing. I tried before gluconate (sold as “Oligosol” in France) and citrate (sold in France as “Granions”), and their effect was 10x milder than orotate. I haven’t tried higher doses of orotate because I don’t feel the need to. But if my stress levels were to increase I would definitely give a try to lithium 2, 5 or 10 mg.
0 negative effects on my eGFR of course. There’s no evidence that lithium at these low doses is nephrotoxic. Toxicity is only seen in bipolar disorder patients who use very high doses.
I think the reason it hits the kidneys at higher level is inhibiting the citrate transport which needs a lot more lithium to be material.
Another new study on Lithium with positive results:
A two-year pilot clinical trial published in JAMA Neurology evaluated low-dose lithium carbonate as a neuroprotective agent in 80 older adults with Mild Cognitive Impairment (MCI). The mechanistic rationale centers on lithium’s capacity to inhibit GSK-3—an enzyme implicated in tau tangle formation—and modulate neuroinflammation, pathways relevant to preserving brain integrity and extending cognitive longevity.
Clinical Findings
Knowledge Gaps and Required Data The study was restricted by a small sample size and a failure to stratify initial enrollment by amyloid status, which likely diluted efficacy signals. Consequently, the cognitive benefits remain informed speculation rather than verified clinical fact. To definitively establish efficacy, researchers require adequately powered trials utilizing modern blood-based biomarkers to pre-select amyloid-positive participants.
Actionable Insights While lithium modulates biological pathways critical to neurodegeneration, current empirical data do not support prophylactic off-label supplementation for memory loss. Lithium acts only as a potential decelerator, not a restorative cure. Continuous medical monitoring remains mandatory due to potential renal and thyroid toxicity. Until larger trials provide verified facts, optimizing known longevity pathways should rely on validated interventions.
https://jamanetwork.com/journals/jamaneurology/fullarticle/2845746
“Participants who entered the RCT received either a 150-mg or 300-mg dose of lithium carbonate or placebo in identical over-encapsulated pills. Participants started 1 pill daily or every other day, based on general medical status and concomitant medications. Doses were adjusted weekly to the maximum tolerated dose and decreased if needed to achieve tolerability. All participants underwent lithium blood level monitoring.”
Clinical Update
Lithium Orotate
“Lithium salts are dosed by the total weight of the salt, of which lithium makes up only a small portion. To convert from lithium carbonate to orotate in terms of mg of elemental lithium, multiply by 4.9 (eg, 300 mg lithium carbonate = 1,960 mg lithium orotate). Keep in mind that bioavailability may differ and that what’s on the label of the orotate product may not be accurate or standardized, given these products are unregulated. Most lithium orotate products are sold as a daily dose of 120 mg (equal to 24 mg lithium carbonate), but some list the amount of pure lithium instead (5 mg).”
Its a bit sad they don’t actually quote the Elemental lithium dose. The doses are still not “low dose” although they are still quite high.
Li2CO3 molecular weight, 73.891, Li2 = 13.882 hence 18.5% of mass is lithium. 150mg =28.18mg Lithium 300=56.36
I think Li should be kept below 50 micromolar and my own test results would imply this is above this level.
I think the mechanism that causes nephrotoxicity in high dose lithium is inhibition of the SLC13 series of citrate carriers and this obviously will happen at a lower level. Hence I would personally think this dosing has the ability to be harmful although not necessarily noticeably so.