30 year old paper but piracetam reverses hippocampal increases in lipofuscin caused bychronic alcohol and withdrawal in rats.
4 Likes
From Ora Biomedical:
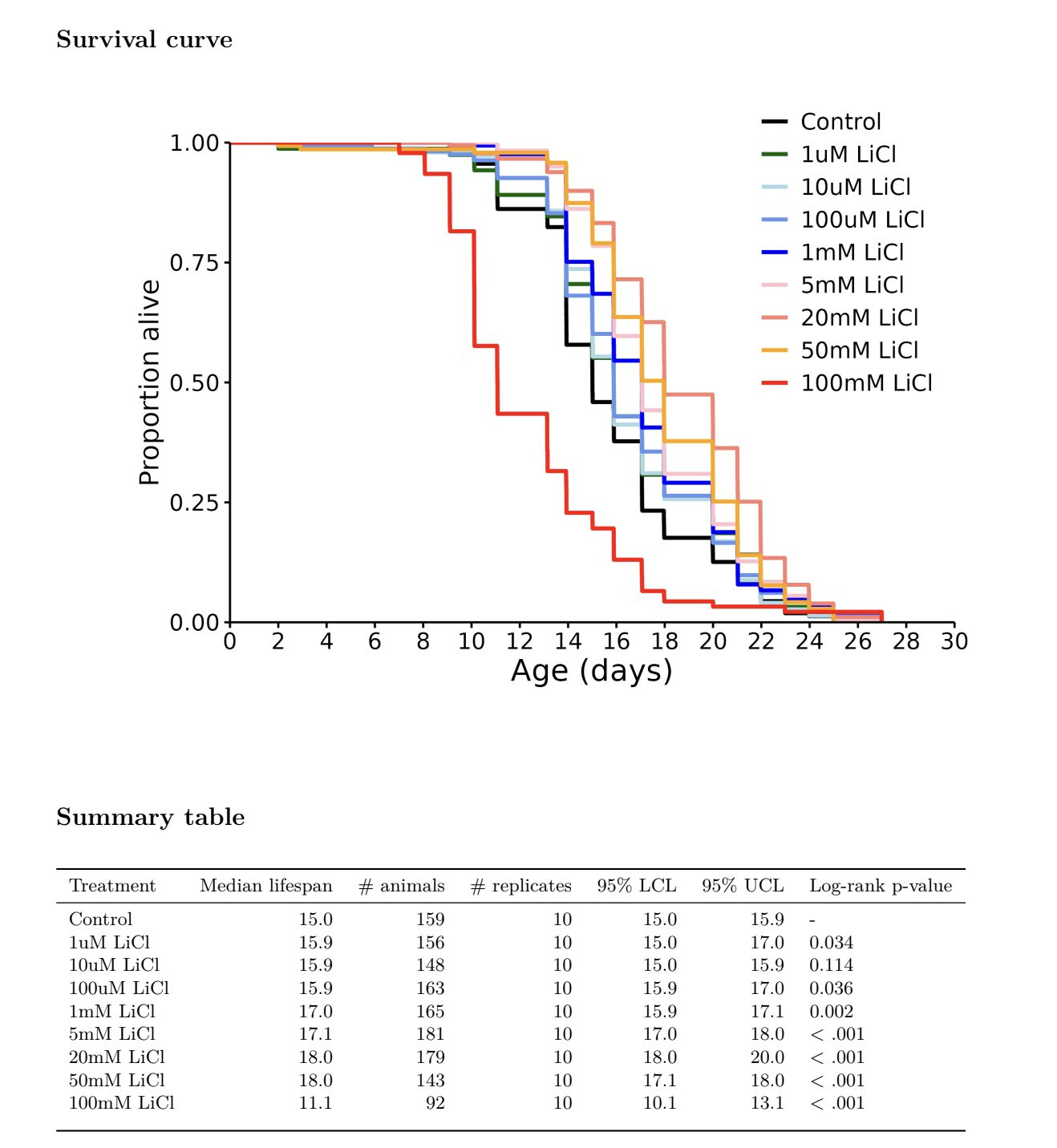
It confirms the “intuition” of many people here: lithium is bad at high doses, neutral at very low doses and great at some “low-medium” doses.
How does this translate to humans? ![]()
12 Likes
Personally I am for around 50 microMolar, but that is in serum not in foodstuffs. Thinking about it this is about 1-5mg (I am on 2 at the moment).
In terms of food people eat 1-2kg per day. Hence it is perhaps a millionth of that by elemental mass. Lithiums molecular weight is about 7. So if we only use that then we are talking about around 1 microMolar or less.
However, this is not really that good a system of comparison. I think the negatives of ltihium come from when SLC13A2 and A3 get inhibited particularly in the kidneys.
This result may argue for a higher lithium dose, but personally I want to stay well clear of inhibiting SLC13A2 and SLC13A3.
6 Likes
Maybe not neutral if we get a subjectively better state of mind. I find it takes the edge off. If I get a longevity benefit, that’s a bonus.
6 Likes
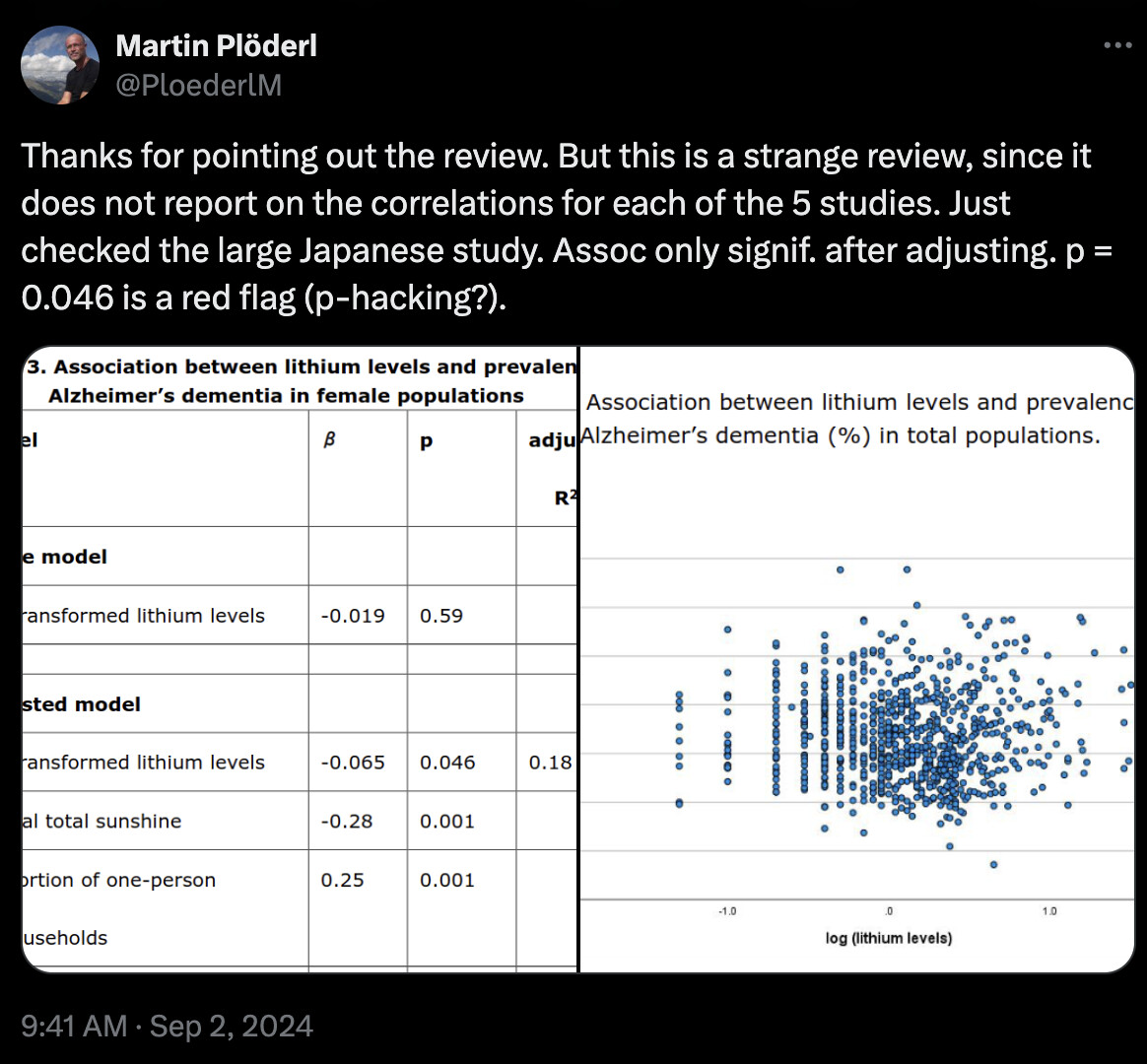
It looks like there was just a new study that found no result for lithium in water supply reducing suicides
https://x.com/PloederlM/status/1830155781330587904
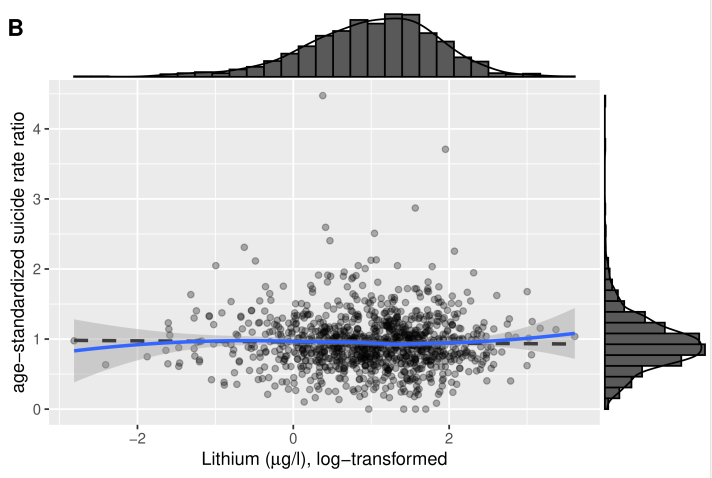
They seem to think it’s all because null results aren’t published so only the ones that find an effect get published
5 Likes
Its good that they publish null results. I am myself not persuaded that the longevity dosage has a measureable mental effect. I keep it really low myself because lithium inhibits the SLC13 series of citrate transporters.
2 Likes
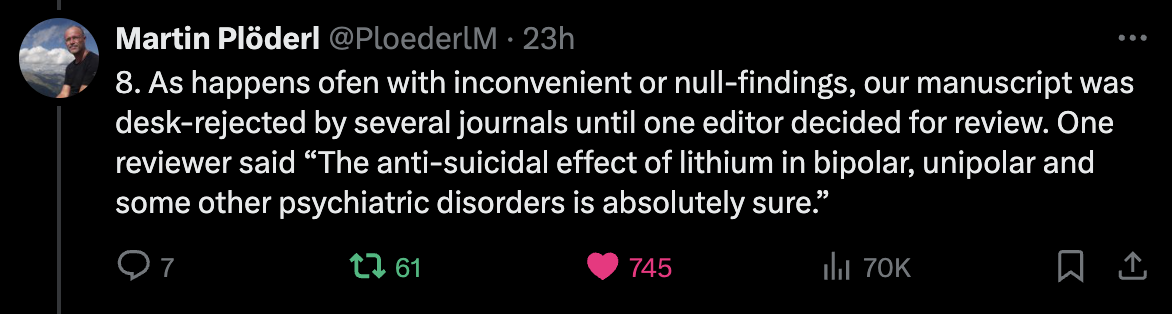
Thanks. This is very concerning (about scientific publishing in general):
Meanwhile we have this just published Brazilian–Saudi–Canadian paper: Trace lithium levels in drinking water and risk of dementia: a systematic review (looks like a bad paper, they used mg instead of µg at some point in the paper for instance…)
We systematically reviewed five available studies, which reported associations between trace-Li in water and incidence or mortality from dementia. Association between trace-Li levels and a lower risk or mortality from dementia were observed at concentrations of Li in drinking water as low as 0.002 mg/L and 0.056 mg/L. Meanwhile, levels below 0.002 mg/L did not elicit this effect. Although three of the five studies found dementia protective properties of Li in both sexes, a single study including lower Li levels (0.002 mg/l) found such association only in women.
If this paper is correct and if the neuroprotective level is 0.002–0.056 mg/L, given that the average adult drinks about 3.2 L per day (2.7 for women and 3.7 for men), this means >0.006–0.18 mg of lithium per day?
[EDIT: I asked the author on Twitter, it turns out Switzerland has one of the lowest lithium concentrations in water. Could it explain the null result?
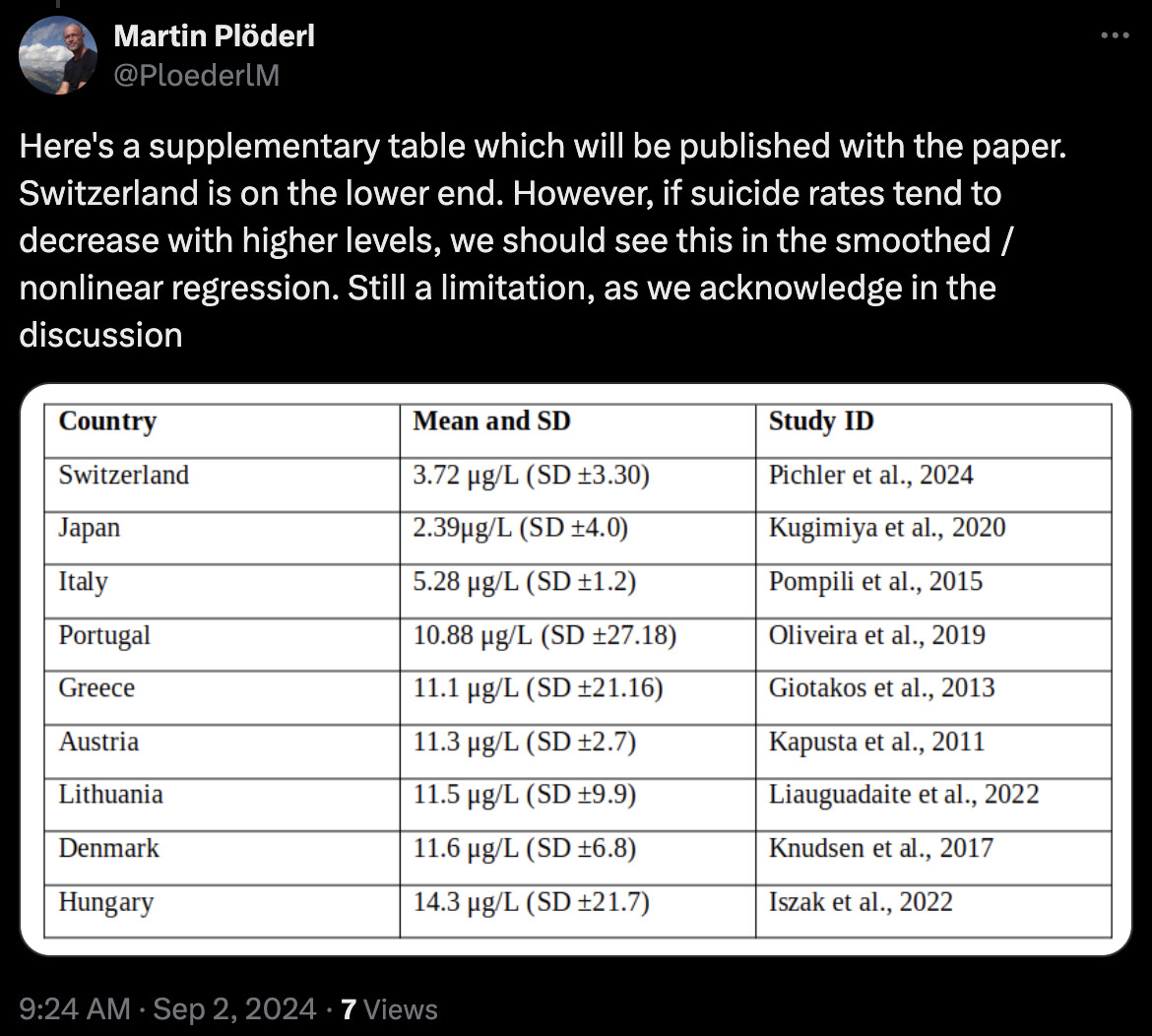
]
1 Like
Tell you what’s funny about this table of lithium water content by countries. Hungary has the highest level if lithium in their water… and also some of the very highest suicide rates in the world, a statistic that’s held for multiple decades. Whereas Switzerland and Italy which are toward the bottom of lithium water content are not known for high suicide rates. That’s why so many epi studies are garbage.
8 Likes
Seems that empagliflozin reduces serum lithium by 70%, not 50%.
4 Likes
@CronosTempi they would have to adjust for income and education and social freedom etc, which is very hard to do, which is why they normally just don’t compare across such different countries. If you try to adjust for all the differences you will just end up confirming your prior beliefs most likely since you will adjust until you get the result you expect.
4 Likes
Open question:
- There’s a growing body of evidence pointing to SGLT2 inhibitors being neuroprotective (longitudinal studies, animal models, and RCTs)
- SGLT2 inhibitors significantly lower serum lithium levels
- Some papers suggest that lithium, at levels as low as those found in tap water, might be neuroprotective
I can’t reconcile the above. I see a few possibilities:
- SGLT2i are not neuroprotective.
- Lithium is not neuroprotective.
- SGLT2i and lithium are both neuroprotective, but SGLT2i neuroprotection is so strong that it overcomes the lithium loss.
- SGLT2i lower serum lithium levels but serum lithiums do not matter for neuroprotection (maybe what matters is brain levels, or CSF, or absorption, or whatever)
- Lithium is neuroprotective but not at the levels seen in tap water so the addition of SGLT2i doesn’t change anything. On the other hand, someone taking a higher lithium dose should adjust it to continue to benefit from lithium’s neuroprotection.
Is there any other possibility? Or did I misunderstand something?
11 Likes
It is a good question.
Lithium inhibits the cell wall citrate carriers at a higher level. That may help with mental illness and depression, but is both known to be potentially nephrotoxic and I would think also undermines the genome more generally. At the longevity dose lithium won’t have any material effect on citrate levels, but potentially inhibits GSK3 which is thought to be helpful.
Personally I am not attracted to any of the weight loss drugs because of my concern about their potential effects on lean mass. I could do with taking my fat mass down a bit, but I took my BMI from 35 to 22 without using weight loss drugs (although I think melatonin helps with this).
3 Likes
Thanks for chiming in.
I don’t think you can qualify SGLT2i as “weight loss drugs”. From what I read, people who are not overweight don’t lose weight on it. I didn’t at least.
3 Likes
There are other examples of interventions that are net positive despite having some negative consequences. Endurance exercise is an example: more likely to have AFib, artery calcification but overall it has a significant life extension benefit.
I take a low lithium dose (5mg lithium orotate)and a sglt2 inhibitor (dapag). I’ll keep watching for clarity on adjusting the lithium dose which doesn’t seem to have a strong effect on anything.
Let us know what you figure out….
1 Like
Can this be tested in worms at ora? I know weve already tested lithium and empa and cana. Cant we just test the same lithium dose that extended lifespan with cana and see if life effect is reduced?
1 Like
Inhibition of SGLT2 enhances the renal excretion of lithium. Worms don’t have kidneys so it wouldn’t affect their lithium levels?
3 Likes
I suppose it could be that neuroprotection happens along many pathways. Imagine someone has 3 different bills to pay, A, B, C, each bill the same amount. If a grant comes along (SGLT2i) and pays bill A, the indebted individual will report that they were financially protected, even if B, C, were not paid, as we don’t know the extent of any neuroprotection from any drug, none are probably 100% anyway. If a different grant institution (lithium) pays bill B, then even if A and C are unpaid, the debtor will report that they were financially protected, same as in the case of the SGLT2i grantor. Now, if the SGLT2i grantor said, I’ll pay for A, but only if you don’t accept the grant from “lithium” (who pays B), and the debtor agrees, then the situation doesn’t change insofar as financial protection. In either case, one of the pathways is protected, therefore overall, neuroprotection is maintained under allthe scenarios I outlined.
Now imagine that there is only one bill to pay. It won’t matter whether SGLT2i pays it or Lithium pays it, it gets paid - protection is maintained. And if SGLT2i says: I’ll pay your bill as long as you don’t accept the grant from Lithium, the bill still gets paid, no difference (assuming both pay the same amount!).
To sum up:
-
Neuroprotection is likely acting along different axis and pathways. If lithium acts along one set of pathways and SGLT2i along a different set of pathways, you might be still protected by either interventions and it would take specific measurements to determine if SGLT2i protects more overall, or lithium more - we don’t know.
-
If both SGLT2i act along the same pathway(s) of protection as lithium, then if SGLT2i displaces lithium, and provides the same protection, then SGLT2i acts as a replacement and substitution, therefore any loss of lithium in the process is irrelevant insofar as neuroprotection.
The overlap of protection pathways need not even occur. Imagine that there’s a field that’s being flooded. We can put the dam downstream close to the field, or much further up the stream, but in either case, we no longer are flooded. It might not matter how you lower LDL, whether closer or further upstream (f.ex. LDL lowering by statins or by BA), what matters is that LDL is lowered, because the active damaging agent is LDL, and removing it by any means is what matters. We don’t care if it’s lithium or SGLT2i in this scenario, if both are addressing some mechanism through the same or different pathways.
And so on. The possibilities are many, it seems to me. But in general, I think the concept of “neuroprotection” is a bit fuzzy - how do we measure that, by specific outcomes or biomarkers or what. Knowing that, we could examine what SGLT2i and lithium do exactly and to see whether they’d be additive, mildly subtractive or what.
1 Like
Your message just refers to assumption 3 (“SGLT2i and lithium are both neuroprotective, but SGLT2i neuroprotection is so strong that it overcomes the lithium loss.”): right?
Neuroprotective means:
- Lower risk of AD or PD in longitudinal studies
- Improved symptoms or biomarkers in RCT (Ideally after a washout period)
- Improved symptoms or biomarkers in animal models (for what they’re worth)
1 Like
Well, it depends how one understands that statement. The questionable words here are “so strong”. Not strong or weak, just different. SGLT2i and lithium could just be ‘six of one, half a dozen of the other’. If they address the same pathway, but one displaces the other, the effect could be the same. If you hit a fish on the head with a green hammer or a red hammer, it’s just as dead. Nobody would say the “boy, the red hammer is so strong, it overcomes the need for the green hammer!”. It’s just a weird thing to say.
And if they address different pathways, it also doesn’t mean SGLT2i has to be “so strong to overcome the loss of lithium”, and the lithium works on a completely different pathway. Example, you want to go around the building into the back. Bob walks around from the left side and Dave from the right. Both are equally fast in reaching their destination, just along different pathways. Nobody would say, “boy, Dave is such a strong walker he can reach the back of the building even though Bob is not walking today!”
They both get the job done, the absence of one doesn’t affect the result. You don’t need one to be so strong as to “overcome” the other.
Maybe this is just a language thing? Because it’s just an odd way of conveying some idea.