@Radiata and @Deborah_Hall - somewhat related there is evidence that aspirin can help in Lp(a) cases (though depending on age, etc there may be other risks with that)
2 Likes
I did not know this.
“Aspirin lowered serum Lp(a) concentrations to approximately 80% of the baseline values in patients with high Lp(a) concentrations (>300 mg/L).”
“aspirin use was associated with a significant reduction in cardiovascular events in carriers of genetic polymorphisms associated with elevated Lp(a) levels. Further studies are needed, however, as these studies focused on narrower subsets of the overall population and genetic markers.”
6 Likes
Thanks, interesting. Aspirin is an anti-inflammatory.
Thank you. I was not aware that aspirin can reduce Lp(a). I have yet to test my Lp(a) for the first time, putting it off because my CRP is in the area of 0.31.
Possible related and purely anecdotal, my wife has been experiencing what she is diagnosing broadly as connective tissue inflammation following relatively light dumbbell workouts and even some yoga routines. She does each three times a week on alternate days. The pain typically occurs with a one-day delay and can be severe enough to sap her energy. She has tried conventional nutritional interventions including curcumin and ginger, along with her already generally low inflammation diet. After six months, she added ibuprofen 200 mg, 2/day and got partial relief. A friend suggested substituting whole turmeric for the refined cucrumin. She added 1/2 to 1 tsp to her morning smoothie and the same amount in the evening in cup of hot water with a little honey. Within 48 hours, the pain was completely gone and has not returned unless her routine pushes a new boundary. She has considered the known variables in her routine and unrefined tumeric is the only plausible candidate at this point. Time will tell but I thought her observation worth sharing.
3 Likes
No side effects from bempedoic acid here after a couple of months.
2 Likes
Are you still used PCSK9i also? What have you Apo B (or LDL) effects been?
Yes, taking Repatha and ezetimibe as well as the BA. Haven’t had my lipids checked since the last time I mentioned it (ApoB and LDL very low, Lp(a) high)
3 Likes
Update in case anyone is interested:
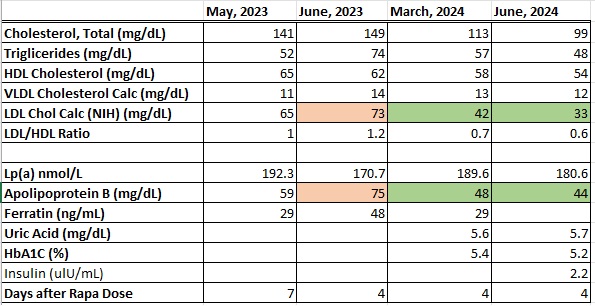
After increasing my rosuvastatin dose for 3 months from 5 to 20 mg, I saw a decrease in my LDLc of 9 points down to 33 mg/dL, but my ApoB stayed relatively constant at 44 compared to 48 mg/dL. Since statins have been reported to increase Lp(a), I figured I’d test it again, but as you can see it’s stable over time. I feel like I’ve hit a wall trying to lower it, even with Bempa-EZ + max statin. I tried niacin at low doses of only 100 mg, but got bad stomach pains so stopped.
I was glad that my HbA1C didn’t increase at the higher dose. I tested insulin at the suggestion of @A_User, and found it to be a little on the low side, 2.2 uIU/mL compared to the reference range on the paperwork of 2.6-24.9. I haven’t done any glucose checks lately, but fasting and post-meal levels were always in the 75-120 range while taking a flozin.
2 Likes
It looks like only a PCSK9 inhibitor would decrease your Lp(a) and apoB. You’ve already max on impacting LDL via synthesis and absorption. With a PCSK9 inhibitor I don’t think you need to use higher dose statin and bempedoic acid, but not medical advice.
1 Like
This de facto race to the bottom we are observing makes me wonder if we will not later learn of adverse consequences from having excessively low levels of various blood lipids. How certain are we, for example, that ultra low LDL levels are beneficial in all cases, especially with respect to levels that can only be reached with medication? If this turns out to be the case, then mother nature has committed a giant screwup. Given that almost all of the medical research in the last 50 to 75 years has been on the consequences of elevated blood lipids, we know very little about life at the other end of the scales.
2 Likes
Not the first time and certainly not the last. See: balding, aging, cancer, alzheimers disease, …
The leading hypothesis for why humans suffer from cardiovascular disease at such high rates is that higher LDL could be beneficial in famines of which there were many in the past. Nowadays, the average person could not eat anything for 3 months and still be at the upper end of normal weight.
8 Likes
True enough on mother nature but when compared with the screw-ups on human medical advocacy over any 25 year period, the screw-ups are much more likely to be the result of errors in human judgment. It remains true that we possess scant data on the mid-and long term effects of ultra low TC, LDL-C, Apo(b), etc. We have growing data suggesting that lower is better but we don’t know what that benefit curve looks like from the low normal level on down.
4 Likes
what about animal studies? are they of any use?
Nothing is beneficial in “all cases” I suspect. There are always outliers. But we have to make decisions based on the data and averages, and there the information is quite clear and the cardiologists seem to be consistent in their messaging:
Mother Nature herself runs a permanent, double-blind trial: people born with loss-of-function variants in PCSK9 or ANGPTL3 cruise through life with LDLs in the 20–40 mg/dL range and enjoy 30-plus-percent cuts in coronary risk without obvious downside (1, 2, 3, 4).
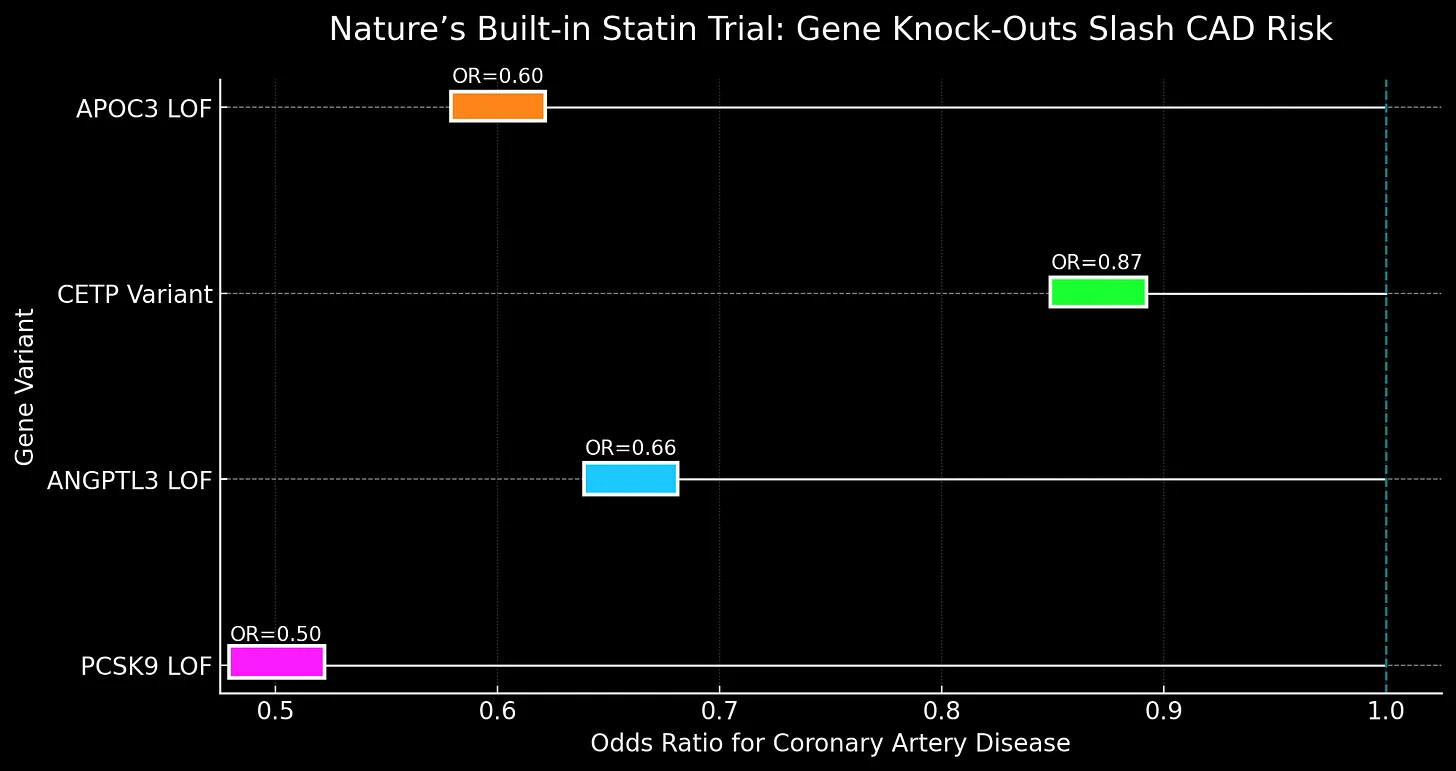
When biology, randomized evidence, and genetics all hum the same tune… policy should probably dance.
Article from @invivo
Great piece!
1 Like
That piece was from @invivo , and yes, great article Alex. You are right on the money with it.
1 Like
I wasn’t clear. Taking Apo(b) as the model case, the evidence for reducing it to 70 mg/dL is strong and broadly based; some find adequate support for further reductions down to 50 mg/dL or even lower. Evidence supporting a target of 20 or even zero is not strong and is largely based on extrapolations and inferences. Perhaps strong randomized clinical studies have been performed and I have not seen them
Additional considerations include limitations in the magnitude of effect when comparing lifelong genetically determined low Apo(b) and LDL-C (especially due to loss-of-function mutations in key genes like PCSK9, APOB, and LDLR) with individuals who lower their levels with pharmaceuticals, especially at an advanced age. Again, to be clear, the available evidence still suggests benefit if initiating reductions at 75 years but there is no evidence suggesting a marginal beneficial contribution for an Apo(b) reduction from, say, 70 mg/dL down to 50 mg/dL for a 75 year old. It also seems worth examining whether such ultra low reductions are universally beneficial across all genotypes.
1 Like
I tried bempedoic acid. The first night – bad leg cramps. Could not believe that it was the BE. Took it again – second night --horrific leg cramps. Third night – no BE, no leg cramps.
I do acknowledge that I am quite prone to leg cramps, and can avoid getting them if I use magnesium foam cream every single night and also take magnesium.
1 Like
It sounds like taking Bempedoic Acid exacerbates a magnesium deficiency you might have. Therefore, you may want to cure that deficiency first and then take Bempedoic Acid afterwards.
3 Likes
But don’t SGLT2i retain magnesium? Seems like a good combo, if you can tolerate them.
2 Likes