Is that independent of any effect on weight loss? Source or graph if you mind? Just curious.
3 Likes
This is likely impossible to distinguish given that there’s always dramatic weight loss in the published studies. Since incretins don’t have any direct effect on lipids it has to be the loss of liver fat that does it (thus no effect on lipids if visceral fat is already low).
1 Like
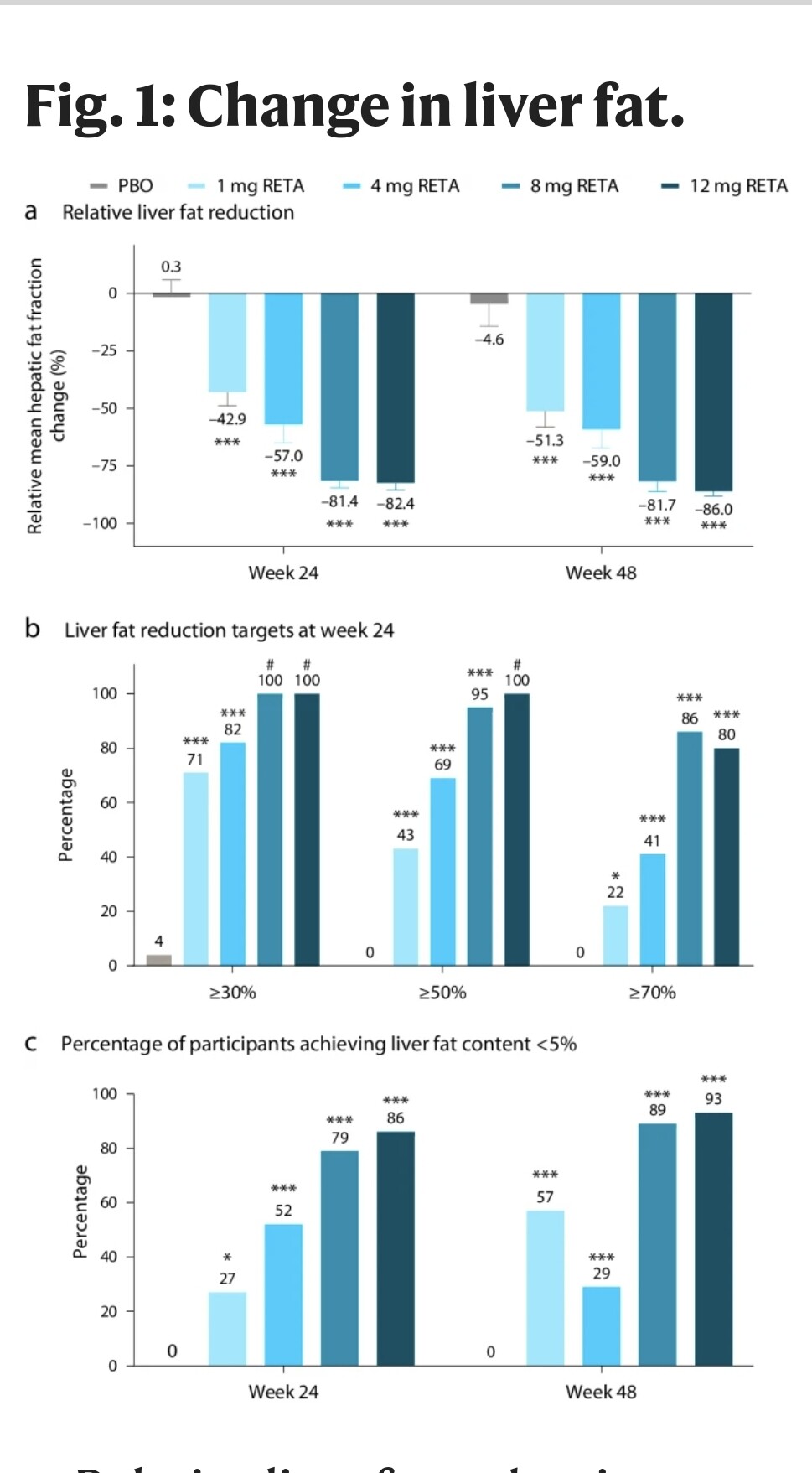
It may be indeed due to dramatic decreases in liver fat, here are several graphs detailing it:
- average liver fqat reduction of 50% after 48 weeks on those on 1mg and up
- liver fat reduction of 30% were achieved by at least 71% of patients, reduction of >50% was achieved by at least 43%, liver fat reduction of >70% by at least 22% of patients. 80% of patients on the highest dose achieved liver fat reduction of >70%
- by week 24, at least 27% had a liver fat content of <5%
4 Likes
Interesting, I’ve heard that the body protects the liver with increases in saturated fat intake by dumping LDL-C into the blood stream, which is why serum LDL-C increases with saturated fats. I don’t know how true this is. But SFA intake is related to liver fat, and LDL-C.
Here are the numbers for apob changes. It’s actually a 24% decrease of apob, not 40% (I was thinking of triglicerides)
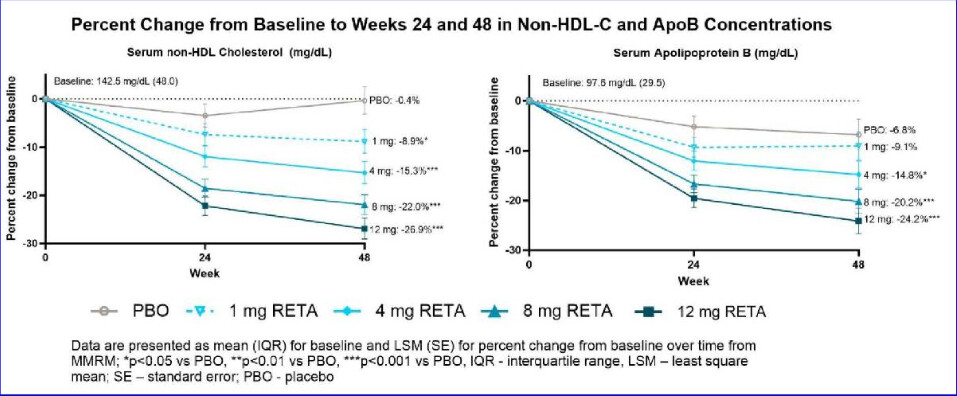
This is from a talk at EASD 2024: e-Science
4 Likes
UDCA might help for osteoarthritis: UDCA (ursodiol) / TUDCA for healthspan and lifespan? - #55 by adssx
5 Likes
What is the easiest, moderate cost way to get these drugs these days - anyone have any suggestions?
The cost of weight loss drugs is finally dropping. How low can prices go?
Self-pay options
In March, Novo Nordisk cut the price of all doses of Wegovy by 23% for people paying in cash, dropping it from $650 to $499 per month for uninsured patients or those without coverage. (The list price of $1,349 stayed the same.)
It follows a similar move from Eli Lilly, which reduced Zepbound’s starter dose to $349 and higher doses to $499 through its self-pay program, Lilly Direct. The discounted doses require patients to manually draw the medication from a vial with a syringe, adding an extra step compared to the prefilled injector pens.
…
Experts point to several forces driving the falling prices: mounting pressure from the public and Congress on drugmakers’ pricing practices; competition from pharmacies, med spas and weight loss clinics offering cheaper compounded versions of the drugs — although many of those are expected to be phased out this month; and the Food and Drug Administration’s recent approval of a generic version of Victoza, an older GLP-1 medication that can start at a cost of around $350 for a month’s supply. The generic, called liraglutide, is taken daily, unlike Wegovy and Zepbound, which are taken weekly.
Full story:
2 Likes
I’ll talk about tirzepatide since semaglutide is so old (relatively). Brand-name will run you up to 500$/month (prescription needed), compounded 170-350$/month (telehealth will write you a prescription after some screening), gray will be about 30-40$/month.
Compound is probably the most straightforward way for someone looking to get started.
1 Like
I’m working my way up to this 10k FU dose with this Nattokinase product. Claude.ai was very alarmed ![]() by the high dosage so am going up 1k per week to ensure no other impacts. With summer here, I enjoy working outside, so am very hopeful the osteo in my hands will cooperate.
by the high dosage so am going up 1k per week to ensure no other impacts. With summer here, I enjoy working outside, so am very hopeful the osteo in my hands will cooperate.
1 Like
One thing that is confusing though is that the package says “100mg is 5,000 FU (scant 1/16 tsp)”. But above you say you take 2 GRAMS. I am taking 1/8 tsp (200 mg) to get the 10,000 FU. Pure Organic Nattokinase Powder - Non-GMO, Gluten Free, Vegan (1 Pound, 454 grams) - Belle Chemical
2 Likes
I can see where there would be some confusion. Both sides (front and back) of the packaging indicate 5000FU/gm which = 5FU per mg.
On the back, they are recommending 100mg as the dose which would = 500FU / dose. A very safe dose that covers their potential liability issues.
I take about 1.5gm = 7500FU daily for the past 4 or 5 years. I still acquired osteo in my left little finger but I can really notice the pain difference if I miss my 1.5gm of Nattokinase.
2 Likes
The Nattokinase is working! I’ve been raking, digging, moving stones etc and way less pain in my osteoarthritic thumb joints. Have even been not bothering to wear the (uncomfortable) braces I got for each hand. Had the dose wrong at first (1/8 tsp) but with your kind correction, I now take a heaping tsp (don’t have a scale) and no side effects other than reducing the pain. Thanks so much. Have tried so many other things.
4 Likes
That’s super duper!!
1 Like
You can get a relatively accurate milligram scale on Amazon for less that $30 They come in handy for those of us who buy bulk powder ![]()
Or you can spend $700 for a lab grade mg scale with ± of 0.1mg accuracy. If you want to get super accurate ±0.01mg scale, a very nice lab scale will run you $2k+
1 Like
Things are looking good for GLP1s…
After adjustment for sex, BMI, hsCRP, and sCD163, semaglutide significantly decreased epigenetic aging: PCGrimAge (-3.1 years, P = 0.007), GrimAge V1 (-1.4 years, P = 0.02), GrimAge V2 (-2.3 years, P = 0.009), PhenoAge (-4.9 years, P = 0.004), and DunedinPACE (-0.09 units, ≈9 % slower pace, P = 0.01).
Semaglutide also lowered the multi-omic OMICmAge clock (-2.2 years, P = 0.009) and the transposable element-focused RetroAge clock (-2.2 years, P = 0.030).
Eleven organ-system clocks showed concordant decreased with semaglutide, most prominently inflammation, brain and heart, whereas an Intrinsic Capacity epigenetic clock was unchanged (P = 0.31). These findings provide, to our knowledge, the first clinical-trial evidence that semaglutide modulates validated epigenetic biomarkers of aging, justifying further evaluation of GLP-1 receptor agonists for health-span extension.
Presentation on this:
7 Likes
Good news on the GLP1 front:
- Some analysts say Eli Lilly’s daily obesity pill, if approved, could still be a viable competitor in the weight loss drug market despite late-stage trial data that disappointed investors.
- In the trial, orforglipron caused weight loss that missed Wall Street’s expectations and came below what Novo Nordisk reported for its oral drug in a separate study.
- But Eli Lilly’s drug could have a few advantages over Novo Nordisk’s pill, including a lack of dietary restrictions, easier manufacturing and a potentially lower price, according to some analysts.
5 Likes
I do think it could end up being extremely popular, depending on tolerability and cost/access, since so many people prefer pills to injections and being able to take it with food is a big bonus.
It also might have a place for long-term maintenance (lose weight fast with retatrutide, for instance, then switch to orfo to keep it off). Also for those who want a less aggressive therapy to lose 10 or 15 pounds of fat to look better and be healthier.
5 Likes
Semaglutide is going generic in India in a week. Has anyone had any success getting a quote for generic tablets? I asked Maulik but he said he hasn’t got any info yet.
1 Like
2 Likes
Sadly, these injection drugs like ozempic need to be refrigerated, so its not going to be very feasible to import these from India (shipping times frequently take a few weeks, so its going to degrade the product).
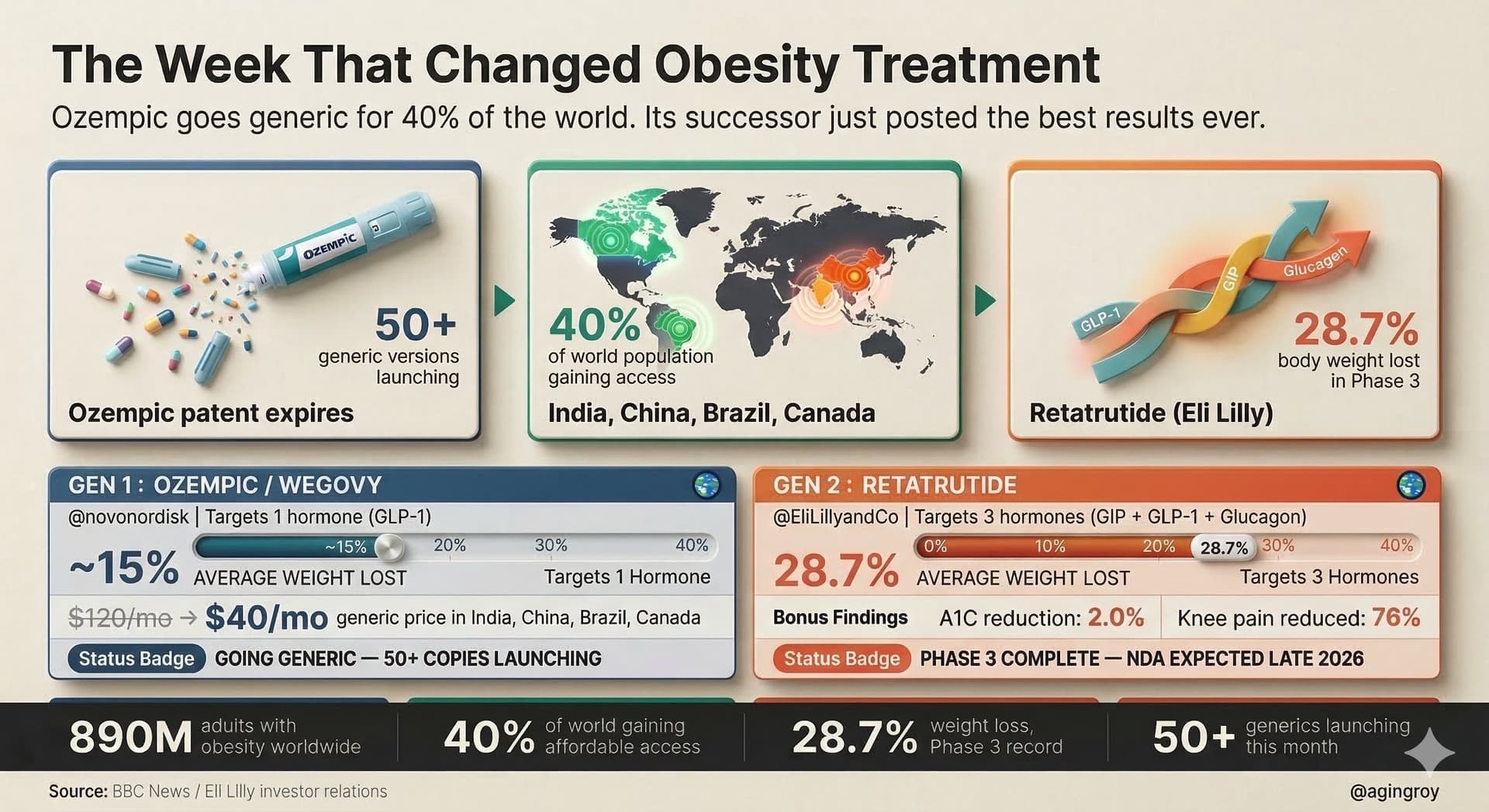
Source: https://x.com/agingroy/status/2034678277713920243?s=20
2 Likes