Do you also use topical retinoids?
Tried the lowest strength tretinoin and tazarotene on and off. My skin is too sensitive to them… I can tolerate the tazarotene lotion (Arazlo) though, but it’s not available as a generic.
What dose are you thinking about?
I’ve had 5 boxes of 10 mg isotretinoin sitting at home since last year and still can’t bring myself to start a low-dose regimen. I’ve done a lot of reading, and it really might do wonders for skin at low doses, but I just can’t justify the risk for myself.
I really don’t see how low-dose isotretinoin could be beneficial for longevity. There are some hints it may help at the cellular level in certain ways, but overall it seems net negative long term.
For context, I’ve been using 0.05% topical tretinoin for 15+ years and my skin (in terms of aging) looks more or less the same as when I started. So I’m wondering: why would you consider oral isotretinoin? What’s your reasoning behind it?
I see a lot of Gen Z taking low-dose iso for “porcelain skin” and prevention… but is it really worth it in the long run? And if you’re using it as an anti-aging strategy, wouldn’t you need to stay on it continuously?
2 Likes
I ended up changing my mind. I’m just going to use topical retinoids. I keep seeing compelling evidence for low dose oral isotretinoin but then I see a lot of negative health effects long term. Why add another complication?
To answer the question of what dose I was thinking about it would have been 5-10mg a night.
I’ve got a lot of topical things to try out: microsphere tretinoin, tazarotene, estriol and estrogen creams. I also just recently purchased the Derminator 2 microneedle device. I’ve not used it yet, I’m waiting until I have a few days off work and any social obligations before I use it just in case it looks kind of brutal.
With all of this, why would I even need oral isotretinoin?
1 Like
@PrimarchLongevity I always found a lot of sensitivity with tubes of tret, but then I tried Dermatica and then Curology tret. There is something about their formulas that are much less sensitizing for me. If you wanted to try them, they usually offer great intro deals… if you can’t find one, I’ll look up my discount code for you, but I don’t think you’ll need it.
1 Like
I’ve posted about the potential of facial fat loss from devices, so I’m sharing a video from insta by a respected plastic surgeon on the topic.
1 Like
Another new company doing a topical Rapamycin-type cream for prevention of skin aging:
in addition to this earlier announcement: A New Rapalog for Skin Aging: Rapalogix Health RLX-201
2 Likes
My simple tips for better skin:
- Vitamin supplements (esp C, D, E). You should probably take these anyway, but yes, it’s also beneficial for the skin.
- Topical vitamins, i.e., ascorbic acid (C) and niacinamide (B3). I use only serums and don’t bother with all the fancy pants brand creams you can get. For both I use 10% concentrations. If you can get higher, fine, but this is what’s readily available to me and it barely costs me anything. For vit C, I just use the stablised form. Much easier to deal with and honestly I think it works fine. But if you can get the pure form ( L-ascorbic acid), that should be better in theory, but don’t worry about it too much.
- Hyaluronic acid, another serum. I use 2% and I combine this with the other products all the time for better absorption and just better hydration. Again, go for the basic cheap serum, not the fancy stuff.
- Retinoids, of course. Tretinoin or Tazarotene. If your skin can’t handle it, at least try Adapalene. Start with a lower strength (e.g., 0.025) and optionally increase it over time (0.05, 0.1). Retinols are pretty much a waste of time and money, so I don’t even bother with those.
- Azelaic acid. It is important it is at least 15% (personally I use 20%). Great product to add for soft and evenly toned skin.
- Hydroquinone. This is a great product that addresses imperfections like sunspots. Only thing is, you shouldn’t use it too often. Personally, I use only one tube (4%, 30g) per year. Just use it daily, and when you run out, wait a year or so.
- SPF, basic stuff, just use it even if it’s not very sunny.
Personally, I have strong skin and it’s been ‘retinised’ by now, so I don’t really have to worry about much, but at first you will have to get used to it and will peel a bit. And don’t combine everything at first. I use .05% tretinoin, mix it with some azelaic acid and moisturiser, then apply it to a damp face with hyaluronic acid already applied. This I do every night without issue (use a cleanser beforehand if you didn’t just shower). In the mornings, I alternate between vit c and niacinamide, together with hyalurinic acid and, again, moisturiser.
Any stuff that is not otc, I just buy online. Why even deal with Rx and all that just to still end up paying more? These are basic ingredients that cost pennies to produce and are easy to buy online nowadays.
Hope this helps anyone. I am a guy and when you look into this sort of stuff you quickly find we are generally leaps behind women in this domain, but I’m trying to catch up a bit. At first I was skeptical b/c my view was it was all marketing bs. And basically, it turns out that most of it is. But there are some things that truly work and if you stick with those, you can get good results.
Also, I wanted to share with you this trial I came across:
Phase 1 Study of KB304 for Moderate to Severe Wrinkles
Looks promising. The start of this thread discussed how there is loss of elastin in the body over time (and no reproduction). This study seeks to address that. The results may also be found as a pdf here.
AI Summary of linked article
Jeune Aesthetics announced positive Phase 1 results from the PEARL-2 trial of KB304, an investigational injectable gene therapy for moderate to severe décolleté wrinkles. The randomized, double-blind, placebo-controlled study showed statistically and clinically meaningful improvements in skin appearance and quality, favoring KB304 over placebo.
Key findings
-
Efficacy:
- Investigator-rated GAIS showed 100% of KB304-treated subjects achieved at least a one-point improvement in wrinkles at 1, 2, and 3 months, versus 14–28.6% with placebo.
- Subject-rated GAIS similarly favored KB304, with 72.7–90.9% reporting improvement across timepoints (vs 14.3% placebo).
- 81.8% of KB304 recipients reported improved satisfaction with wrinkles at 3 months (SSQ), compared with 14.3% on placebo.
- Broader skin benefits: Investigators reported universal (100%) improvements in elasticity, crepiness, hydration, and radiance among KB304-treated subjects at all assessed timepoints.
- Safety: The safety profile was favorable , with mostly mild-to-moderate adverse events that diminished after initial dosing; no severe or drug-related serious adverse events occurred.
Study details
- Participants: 19 enrolled (12 KB304, 7 placebo); 18 completed assessments.
- Mechanism: KB304 uses a non-integrating HSV-1–based vector to deliver genes encoding type III collagen (COL3) and elastin, aiming to restore the extracellular matrix by inducing endogenous production in skin cells.
Next steps
- Based on the results, Jeune plans to advance KB304 to Phase 2, meet with the FDA, and submit a newly developed décolleté-specific wrinkle scale (JDWS). Phase 2 initiation is targeted for first half of 2026.
Significance
- KB304 is positioned as a first-in-class approach that directly addresses elastin (and collagen) loss and targets the décolleté, an area with no FDA-approved injectable treatments, aiming for natural-looking rejuvenation.
9 Likes
KB304 looks very promising.
Where do you source your Hydroquinone?
The regular suspects (India Pharmacies) all sell it… some of the brands I’ve tried (they all work):
Hydroquinone 4% Abbott Melalite Forte Cream30 g
Hydroquinone 2%, Kojic acid 2%, Ascorbic acid 0.5%, Lactic acid 2%
Dr Reddy’s Depiwhite Cream15 mL Tube
Hydroquinone 2% + Mometasone furoate 0.1% + Tretinoin 0.025%
ZydusSkinlite cream25 g
Some old pricing examples:

2 Likes
Or… eat kiwi fruit.
Eating a common Vitamin-C packed fruit might totally transform skin, study finds
2 Likes
Has anyone explored oral photoprotection? I live in Scandinavia and am not diligent with sunscreen usage. I looked into carotenoids like beta carotene, lycopene, astaxhantin, lutein as well as nicotinamide and hyaloronic acid. Does anybody have experience with using carotenoids to create a tan-like colouring of the skin? It’s difficult to ascertain just how much one needs for it to look natural rather than outright orange looking.
2 Likes
Astaxanthin probably does something at moderate doses (12-24mg) but it’s nowhere near as good as actual sunscreen.
3 Likes
You really should become dilligent with sunscreen usage. I used to be like you.
This image inspired me to always put sunscreen on before going out in the sun for more than a 1-2 minutes:
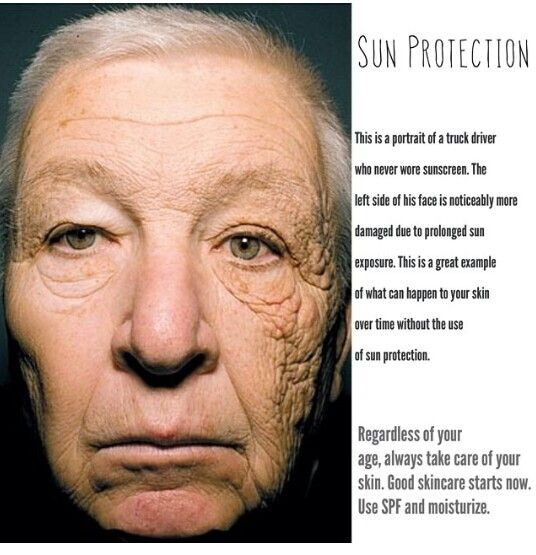
6 Likes
It’s so true. I have more blemishes on the side that faces the sun when I drive.
3 Likes
I’ve heard azelaic acid can remove those. I presume you’re still using sunscreen and getting these blemishes on those spots in spite of that?
3 Likes
I also have the light from my office windom and car Window hitting my face from the same side. I also see a difference on my skin.
3 Likes
Farm boy waiting for spring to roll down the window in the pickup, hang his arm out, looking cool.
There is a difference in my right arm vs left as well as right side of my face vs left. The right side has significantly fewer issues.
2 Likes