Thank you for the tip on Marek Health! I had no trouble placing three orders (each about 12 hours apart), and while it said receiving the lab slip could take a couple of days each one was available within a few hours of my placing the order.
I’ll update this post if I can figure out a spreadsheet to share, or maybe someone else is better at Excel than I am and can create one. I did a series of blood draws over three days, each at about the same time (blood draws were within 10 minutes of each other - one day apart). My goal was to see how much of an impact eating a whole grapefruit might have on me and also how fast my clearance was. Here are the results:
Day zero, -2 hours: 2mg tablet of US prescribed/US pharmacy generic sirolimus followed immediately by eating a red grapefruit. I was otherwise in a fasted state - I’d done a set of routine safety labs (fasted) earlier in the day, so this was rapamycin on an empty stomach followed immediately by a whole ruby grapefruit.
Day zero: 8.1 ng/mL (I assume this is pretty close to peak)
Day one: 2.3 ng/mL (this is MUCH lower than I expected - presumably it should have been ~5.3)
Day two: 1.8 ng/mL (this seems more in line as a correct half life relative to day one’s value)
My BSA is just shy of 2m^2 (thanks @59vw for posting this link in another thread: BSA Calculator - Body Surface Area). Conveniently for me, it looks like I’m approximately the same “size” as all of the subjects in the Sirolimus Kinetics and Safety in Volunteers paper.
Any thoughts?
I’m interested in repeating the same round of tests in a couple of weeks, this time just consuming 2mg (no grapefruit) and also taking at least one additional draw (day three). From this thread (Rapamycin / Sirolimus Blood Test - My Results - #43 by RapAdmin), @RapAdmin mentions it may take 1-2 hours for grapefruit to reach its peak. So, one additional thing I could try is eating the grapefruit at t-4 hours, then having the rapamycin at t-2 hours, then doing the first blood test at 0 hours. Another thing I could do is skip the grapefruit variable, bring a book, and hang out at the phlebotomist for a couple of hours - maybe doing a draw at 30, 60, 90, and 120 mins.
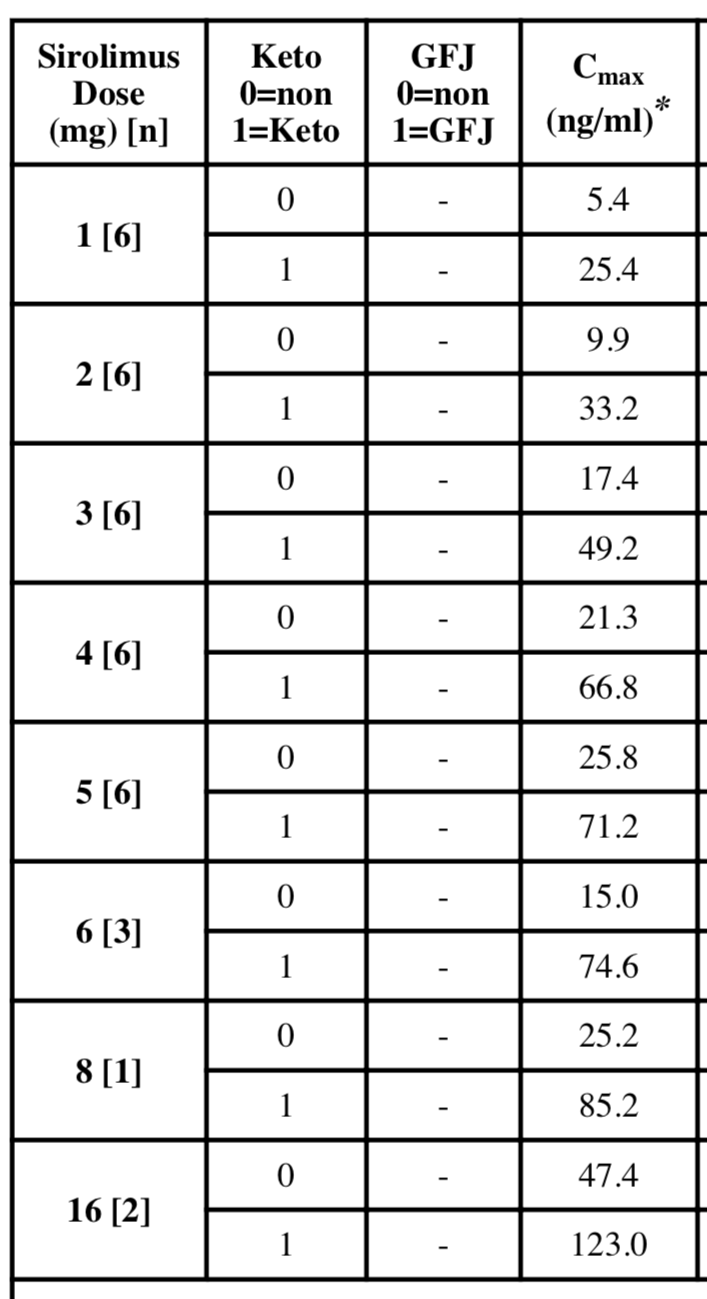
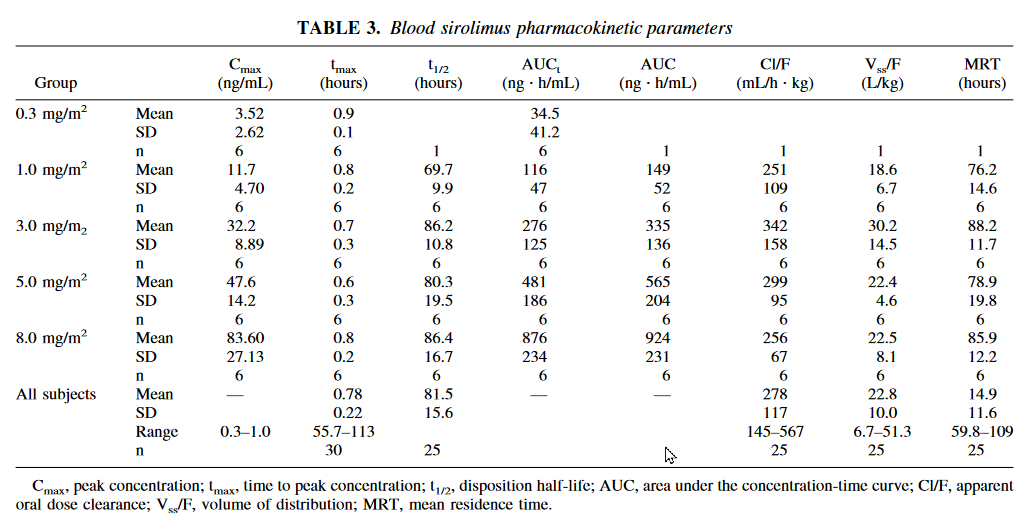
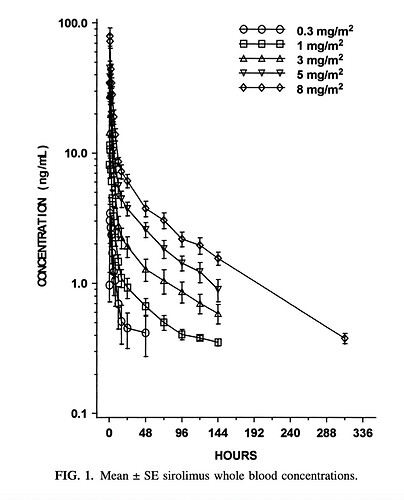
Also, in looking at the charts from the above paper (specifically Table 3 and Figure 1) it seems like my assumed/near peak at 2 hours more closely maps to a somewhere between a 0.3mg/m^2 (0.6mg dose equivalent) and 1mg/m^2 (2mg dose equivalent). I.e., either the whole grapefruit did nothing, or it did something but my body just doesn’t respond to rapamycin much. And, also from Table 3, it looks like tmax was reached at sub one hour across all subjects (roughly an average of 45 minutes). It’s hard to see from Figure 1 how fast the initial fall off is. I’ll see if I can find their underlying data.
{kind=link}
{kind=link}