Dopamine paper
It was inserted by stereotactic neurosurgery, basically the same broad “needle-navigation into a deep brain target” universe as DBS, except instead of implanting an electrode, they injected a living cell suspension. Because apparently “put cells in the basal ganglia with GPS-for-brains” is where medicine is now. 

The short version
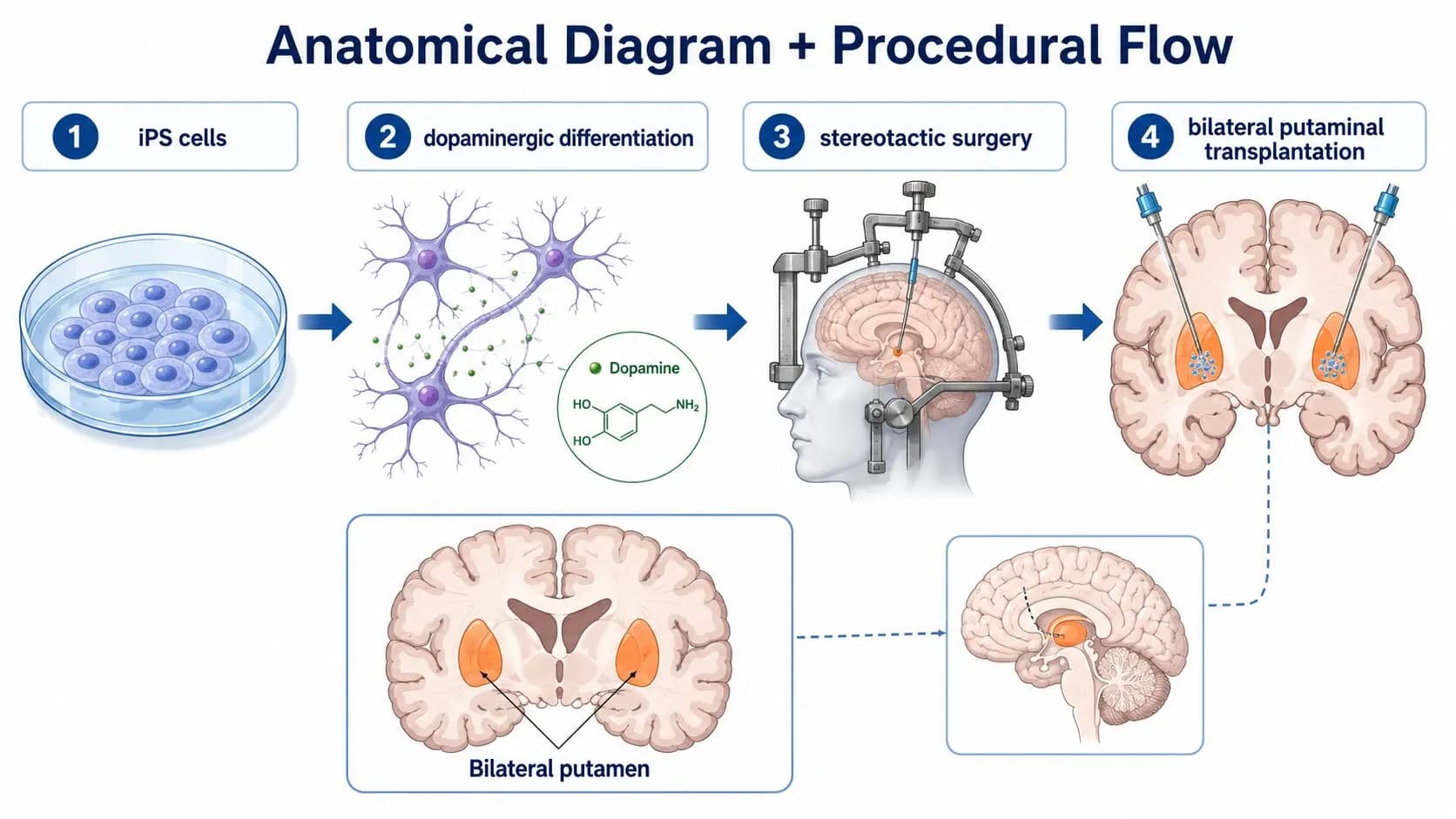
They did bilateral putaminal transplantation:
left putamen injection + right putamen injection
The putamen is deep inside the brain, so they did not open a huge flap and scoop around like medieval raccoons. They used a stereotactic frame/navigation system to guide a thin custom injection needle through planned paths into the putamen.
The Nature paper says the cells were transplanted into the putamen using the iPlan neurosurgical navigation system, with trajectories designed to hit the dorsal and caudal putamen while avoiding sulci and blood vessels. Surgery used a Leksell G stereotactic frame, a custom injection needle, and intraoperative cone-beam CT to confirm injection sites.
Step by step: what likely happened
1. They made the cell product fresh
Before surgery, they produced iPS-cell-derived dopamine progenitor cells. These were enriched using CORIN+ sorting, meaning they selected cells with a developmental marker associated with the ventral midbrain/floor-plate lineage. The final product was “fresh,” not frozen, and had to pass quality-control criteria before transplantation.
So they were not injecting raw iPS cells. Very important. Raw pluripotent cells would be a tumor-risk nightmare. They injected already-patterned dopamine progenitors / young dopamine neurons.
2. They mounted the patient in a stereotactic frame
The paper names the Leksell G frame. That is a rigid skull-mounted coordinate system. Barbaric-looking but extremely useful, because brains are soft wet maps and surgeons prefer not to freestyle their way through the caudate. 
The frame lets the team translate MRI/CT brain coordinates into real-world needle angles and depths.
3. They planned needle paths into the putamen
They used surgical navigation to plan trajectories into the putamen.
The target was not just “somewhere in the striatum.” They specifically aimed for the dorsal and caudal putamen, which is heavily involved in motor control and strongly affected in Parkinson’s.
They designed the paths to avoid:
sulci = grooves on the brain surface
blood vessels = obvious bad thing to spear
ventricles / risky tissue corridors = also best avoided, shockingly
4. They inserted a custom injection needle
A thin needle/cannula was advanced along each planned trajectory into the putamen.
The paper says they used three trajectories per hemisphere. Since it was bilateral, that means:
3 paths into left putamen
3 paths into right putamen
= 6 total needle trajectories
Each trajectory had four to eight injection deposits, so they distributed cells at multiple points instead of dumping one blob in one place like a confused baker piping frosting into the brain.
5. They injected multiple small deposits of cells
The dose was:
low dose: 2.1–2.6 million cells per hemisphere
high dose: 5.3–5.5 million cells per hemisphere
The methods section says they used 4–8 injections per trajectory, across 3 trajectories per hemisphere, to deliver 2.1–5.5 million cells per putamen.
So per side, roughly:
3 trajectories × 4–8 deposits each
= 12–24 little deposits per putamen
Bilateral total:
24–48 deposits across both putamina
That gives spatial coverage, letting the graft occupy a broader motor putamen region rather than forming one dense lump.
Why multiple tracks and deposits?
Because the putamen is not a tiny dot. It is a 3D structure.
If you inject one big bolus, you risk:
too dense a graft
poor diffusion of nutrients
uneven dopamine restoration
local pressure/injury
bad coverage of the motor territory
Multiple small deposits are trying to create a distributed graft field:
o o o
o o
o o o
Instead of:
O
That matters because dopamine is a local circuit modulator. You want dopamine-producing cells spread through the motor putamen, not one dopamine meatball sitting in the corner. Biology, tragically, has geometry.
Why the putamen, not the substantia nigra?
Because the original lost neurons live in the substantia nigra, but their axon terminals release dopamine in the putamen/striatum.
To fully rebuild the original system, you would need grafted neurons in the substantia nigra to send long, accurate axons into the putamen. That is much harder.
So the pragmatic hack is:
Do not rebuild the entire nigrostriatal cable.
Put dopamine-producing cells directly at the output terminal zone.
The grafted cells become something like a local dopamine island in the putamen.
Not perfect anatomy. But maybe enough functional dopamine release to help motor circuits.
How they checked placement
They confirmed injection sites during surgery using cone-beam CT with an angiography system.
So the flow was roughly:
pre-op MRI/CT planning
↓
stereotactic frame coordinates
↓
planned needle trajectories
↓
needle insertion
↓
intraoperative cone-beam CT confirmation
↓
cell deposits
↓
serial MRI/PET follow-up
Why “bilateral” matters
Parkinson’s can be asymmetric, but motor circuits exist on both sides. The left putamen influences the right side of the body, and the right putamen influences the left side.
So bilateral transplantation means they treated both sides:
left putamen → helps right-body motor control
right putamen → helps left-body motor control
In the trial, the first participant had the two sides done separately with an 8-month interval for safety. The efficacy group had simultaneous bilateral surgery.
What happens after insertion?
Immediately after injection, the cells are just living grafted progenitors sitting in the putamen. Over months, the hope is:
survive
↓
settle/spread
↓
mature into dopamine neurons
↓
express dopamine machinery, e.g. tyrosine hydroxylase / AADC
↓
take up DOPA
↓
make dopamine
↓
release dopamine locally
↓
improve basal ganglia motor signaling
This is why the 18F-DOPA PET increased later. The grafts were not expected to instantly function like mature adult dopamine neurons the second the needle came out. Cells need time to mature and integrate, because apparently even neurons have onboarding.
The cleanest picture
Imagine the putamen as a long, curved motor-control sponge that lost its dopamine input.
They inserted a needle into several carefully planned deep-brain paths and left little clusters of dopamine-progenitor cells along each path:
LEFT PUTAMEN RIGHT PUTAMEN
track 1: • • • • track 1: • • • •
track 2: • • • • track 2: • • • •
track 3: • • • • • track 3: • • • • •
Those dots are cell deposits. Over time, they are supposed to mature into dopamine-producing graft tissue.
So “inserted” means:
a stereotactically guided custom injection needle delivered many small deposits of fresh iPS-derived dopamine progenitor cells into both putamina, using 3 planned trajectories per side and 4–8 deposits per trajectory.