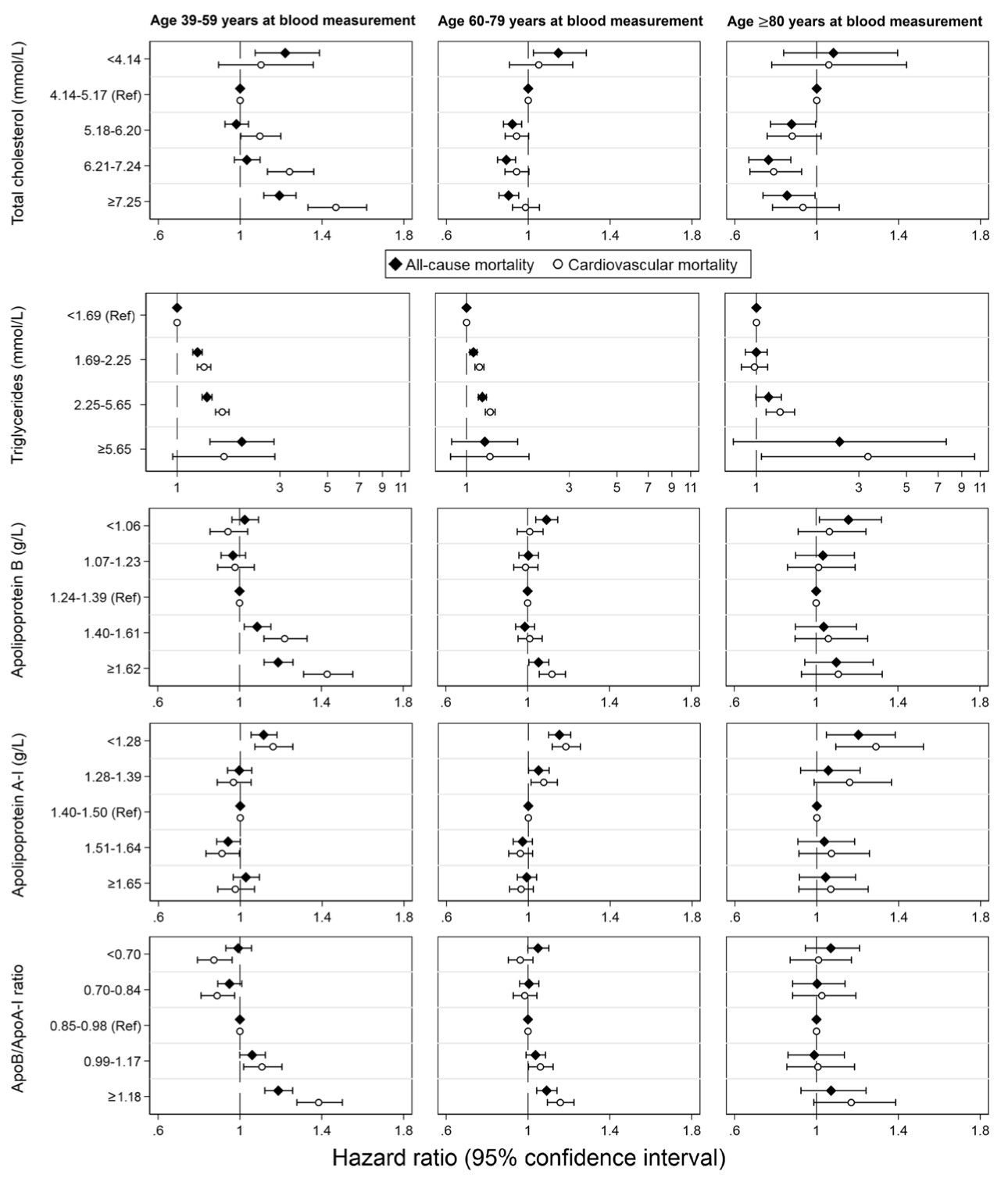
it’s not what the plots show.
Very low TC is always bad for all cause mortality for all age groups.
Very low TC is trending bad for CVD mortality for all age groups though not statistically significant.
So if you have a too low TC you die sooner.
For APOB there is no significant effect for very low, low or medium levels.
Very low APOB is trending bad though not statistically significant.
High and very high APOB is bad.
So keep your APOB low of medium. Extremes are bad.
In all cases TG is bad and low HDL (APOA1) is bad.
I believe that what matters most is the process of reverse cholesterol transport. It’s not just about the composition of HDL-C or quantity of apoA-1 particles, but rather the effectiveness of removing cholesterol from tissues. Unfortunately, this process cannot be easily measured and is not fully understood yet. Once we find a medical intervention to address this issue, then we can consider the end of ASCVD IMO.
While researching CETP inhibition, I came to listen to John Kastelein’s interview with Petter Attia and he talks about this. And it makes sense since studies show poor correlation between LDL-C and ASCVD, meaning you can get ASCVD at both high and low levels and avoid it at high levels. So yes, there are all other risk factors, but still sometimes does not male sense. In some people there must be another protective mechanism that protects them from getting ASCVD and reverse cholesterol transport makes perfect sense to look at as lowering of LDL-C has just as much power as we know from RTCs. Even drastic lowering reduces absolute ASCVD mortality only marginally and data from prevention trials on healthy people is even more puzzling.
The death from any cause graphic (bottom right) sure doesn’t look particularly compelling. And I say this as a person who is currently taking Rosuvastatin.
Author Affiliations: Laboratoire Cœur and Nutrition, Faculty of Medicine, Université Joseph Fourier and Centre National de la Recherche Scientifique, Grenoble, France (Dr de Lorgeril and Ms Salen); Harvard Medical School, Boston, Massachusetts (Dr Abramson); Department of Obstetrics and Gynaecology, Laval University, Quebec City, Quebec, Canada (Dr Dodin); Department of Clinical Sciences, Institute of Natural Medicine, University of Toyama, Japan (Dr Hamazaki); Cardiology Department, Clinique Antoine Depage, Brussels, Belgium (Dr Kostucki); Open Research Center for Lipid Nutrition, Kinjo Gakuin University, Nagoya, Japan (Dr Okuyama); Réadaptation Cardiovasculaire, Centre Hospitalier de Machecoul, Machecoul, France (Dr Pavy); and Cardiology Department, Clinique de Genolier, Genolier, Switzerland (Dr Rabaeus).
Who me? (what me worry?) I wouldn’t mute anybody…I rejoice in the whole spectrum of human idiosyncrasies. (and believe me you see 'em all here…not you, of course!)
P.S. I am just starting a charity tho.