Not sure the mechanism but my psoriasis and urticaria (10+yrs) disappeared within 7 days of adding BPC157 /TB 500 to my CJC 1295/Ipamorelin at night. I can only conjecture that it might be similar to the Thymus rejuvenation protocol? It is not why I am taking them, but I will take a beneficial side effect! I can now tolerate medications/foods that I have never been able to take (ezetimibe, nuts) without a breakout.
5 Likes
@RapAdmin not sure if ChatGPT will distinguish between short term health vs healthspan vs longevity without that being explicitly included in the prompt (and its answer above seems to address the question in a bit of mixed together way).
@LukeMV from a longevity optimization perspective one might want to also consider T / Free T / Bio available T not being too high
1 Like

1 Like
Thanks for a very detailed report on the main forms of Testosterone. It is very interesting to notice how the quantity of bioavailable T in your case is at the opposite of the lab range with respect to total T. Unfortunately, this suggests to us the poor usefulness of the total T parameter since it doesn’t reflect the amount directly available for the body, which governs biological signaling.
A similar situation unfolds with IGF-1. It binds strongly to IFGBP-3, so total IGF-1 may not be representative of the amount available to its receptors in the various cells of the body.
I asked deepseek to elaborate, it goes into detail but that’s the basic rationale.
My concern now is that the quantities of total T and total IGF-1 we rely upon may be a very poor indicator of their actual biological action.
The relationships among total IGF-1, free IGF-1, and bioavailable IGF-1 revolve around how IGF-1 (Insulin-like Growth Factor 1) is distributed in the bloodstream and its accessibility to tissues. Here’s a structured breakdown:
1. Total IGF-1
- Definition: The entirety of IGF-1 in circulation, including all bound and unbound forms.
-
Binding:
- ~95–99% is bound to IGF-binding proteins (IGFBPs), primarily IGFBP-3 in a stable ternary complex with an acid-labile subunit (ALS). This complex acts as a reservoir, prolonging IGF-1’s half-life.
- Smaller fractions bind to other IGFBPs (e.g., IGFBP-1, -2, -5).
- Measurement: Routinely measured in clinical settings via immunoassays, reflecting overall IGF-1 production (largely driven by growth hormone).
2. Free IGF-1
- Definition: The unbound, biologically active fraction (~1% of total IGF-1) that can directly interact with IGF-1 receptors.
- Significance: Represents the immediately available pool for cellular activity. However, its low concentration makes precise measurement challenging.
3. Bioavailable IGF-1
- Definition: Includes free IGF-1 plus IGF-1 bound to low-affinity IGFBPs (e.g., IGFBP-1, -2) that can readily release IGF-1 for tissue uptake.
- Exclusion: Excludes IGF-1 in the stable ternary complex (IGFBP-3 + ALS), which is less accessible.
- Dynamic Regulation: Influenced by factors like nutrition, stress, or proteases that modify IGFBP levels or cleavage (e.g., fasting ↑ IGFBP-1, altering bioavailability).
Key Relationships
- Total IGF-1 = Free IGF-1 + IGF-1 bound to all IGFBPs (including ternary complex).
- Bioavailable IGF-1 ≈ Free IGF-1 + IGF-1 loosely bound to low-affinity IGFBPs (e.g., IGFBP-1, -2).
Functional Implications
- Activity: Free IGF-1 is the most active form, while bioavailable IGF-1 reflects the “dynamic pool” accessible to tissues.
-
Clinical Relevance:
- Total IGF-1 levels indicate systemic GH activity (e.g., elevated in acromegaly, low in GH deficiency).
- Bioavailable IGF-1 better correlates with physiological effects (e.g., growth, metabolism) but is harder to measure directly.
- Conditions altering IGFBPs (e.g., liver disease, malnutrition) may disrupt bioavailable IGF-1 without affecting total levels.
Regulatory Factors
- Growth Hormone (GH): Stimulates hepatic IGF-1 and IGFBP-3 production.
- Nutrition: Fasting ↑ IGFBP-1, which may paradoxically ↓ bioavailable IGF-1 by sequestering it.
- Proteases: Cleave IGFBPs (e.g., in inflammation), releasing IGF-1 into the bioavailable pool.
In summary, total IGF-1 reflects overall production, free IGF-1 is the active fraction, and bioavailable IGF-1 encompasses the dynamic, tissue-accessible pool. Their interplay determines IGF-1’s biological impact, with clinical assessments often focusing on total IGF-1 due to measurement practicality.
3 Likes
Can we test these at normal labs?
Actually, I don’t know. Maybe IGFBP. I’ll have to ask the local lab. Interpreting the results would be another issue. The ratio IGF-1/IGFBP3 has been used in studies by Luigi Fontana.
2 Likes
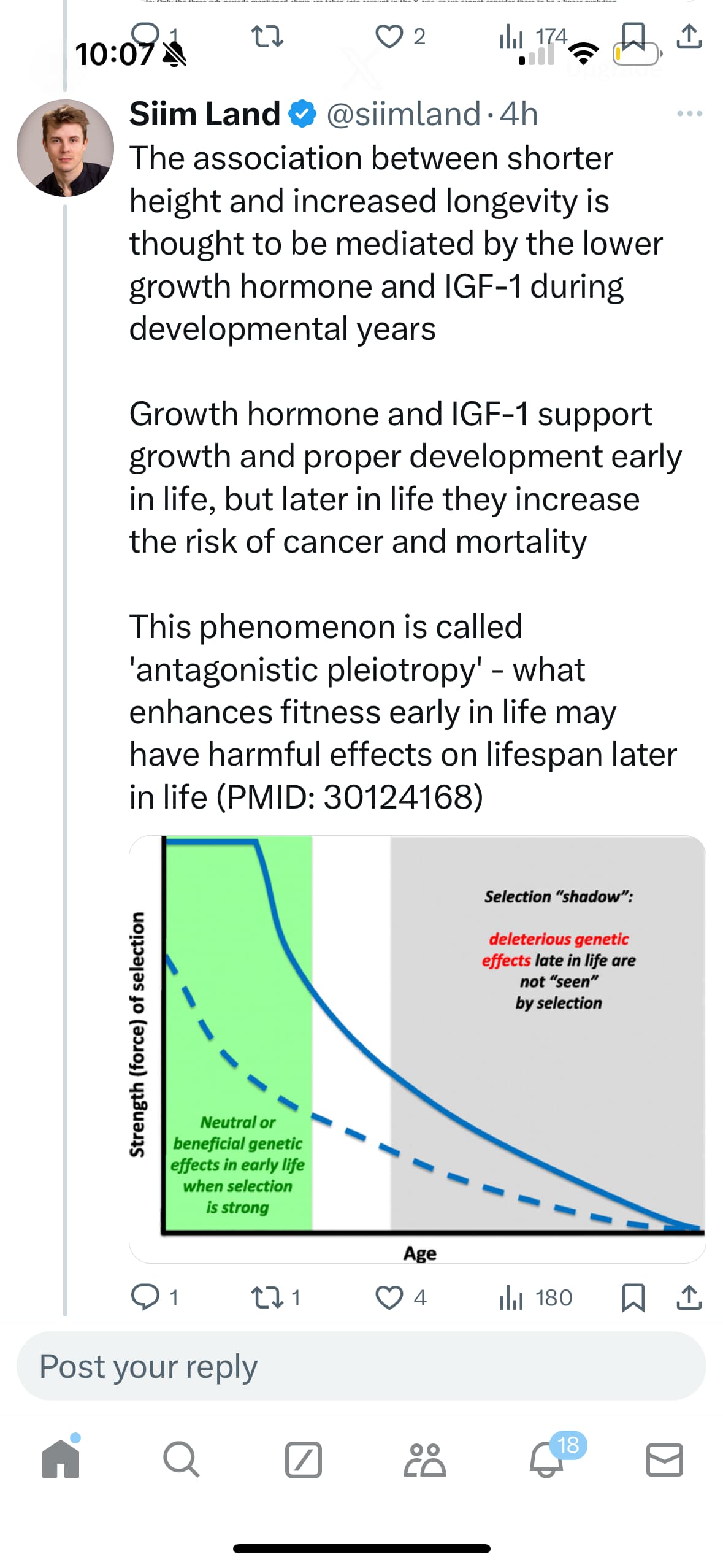
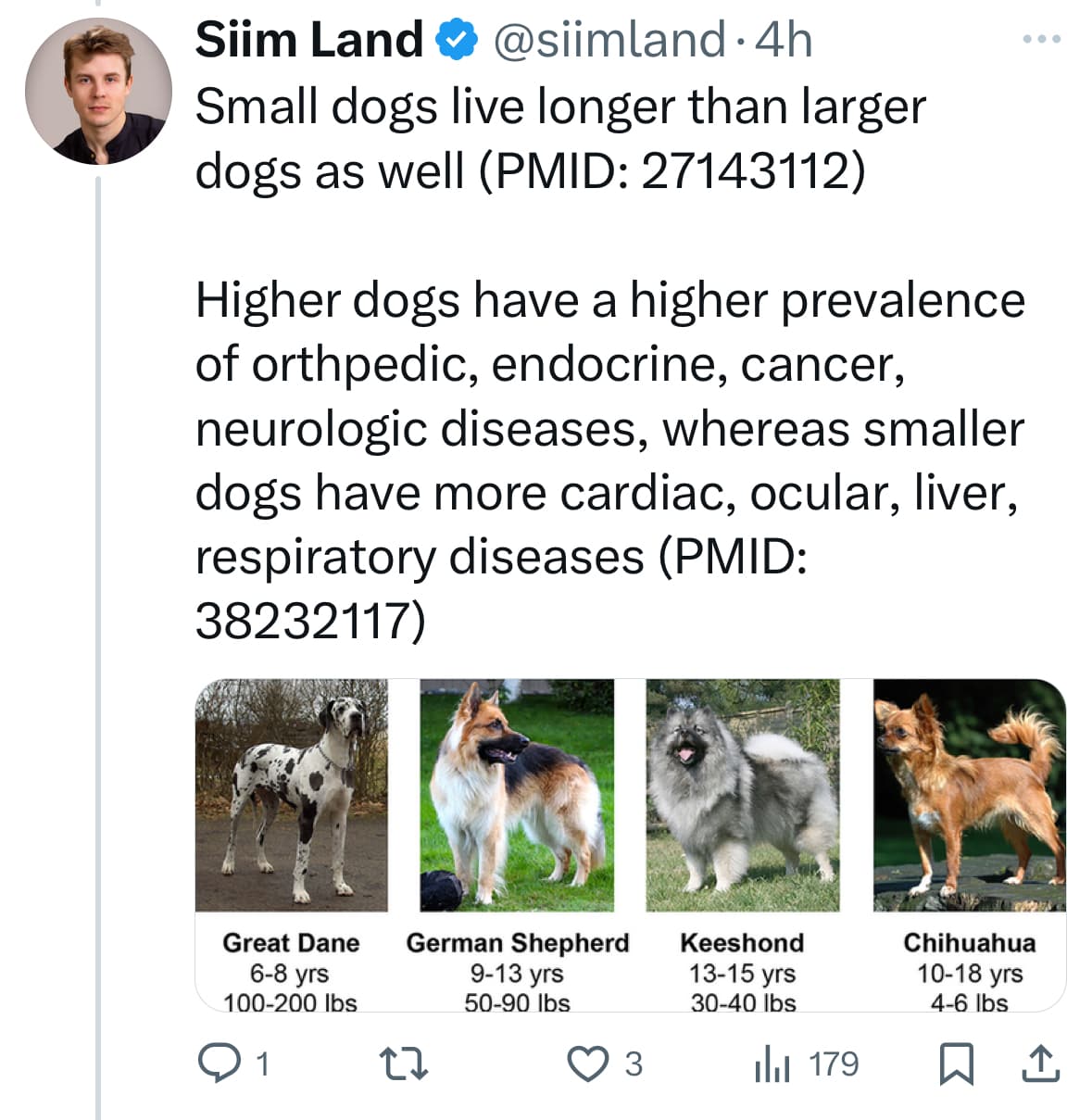
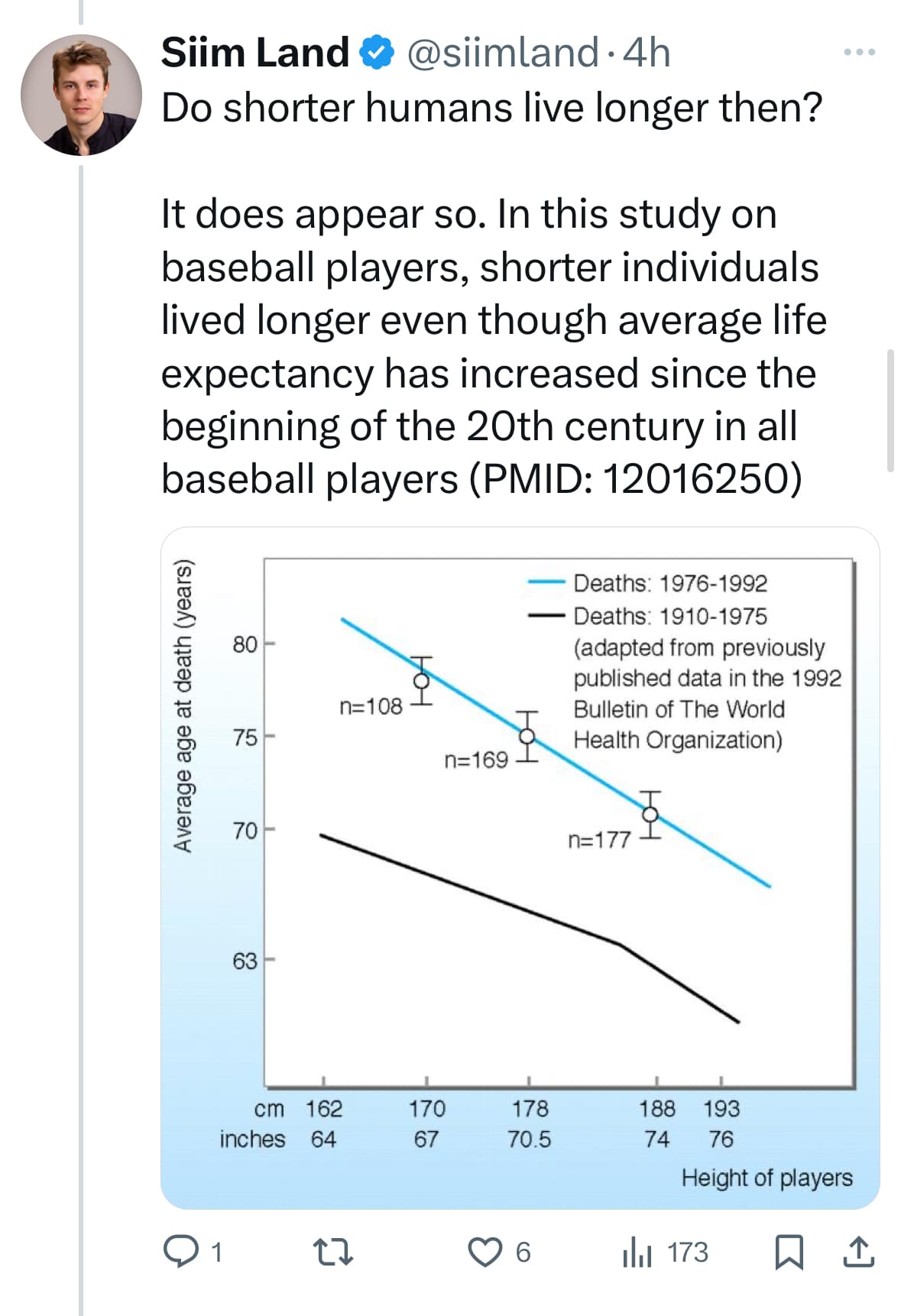
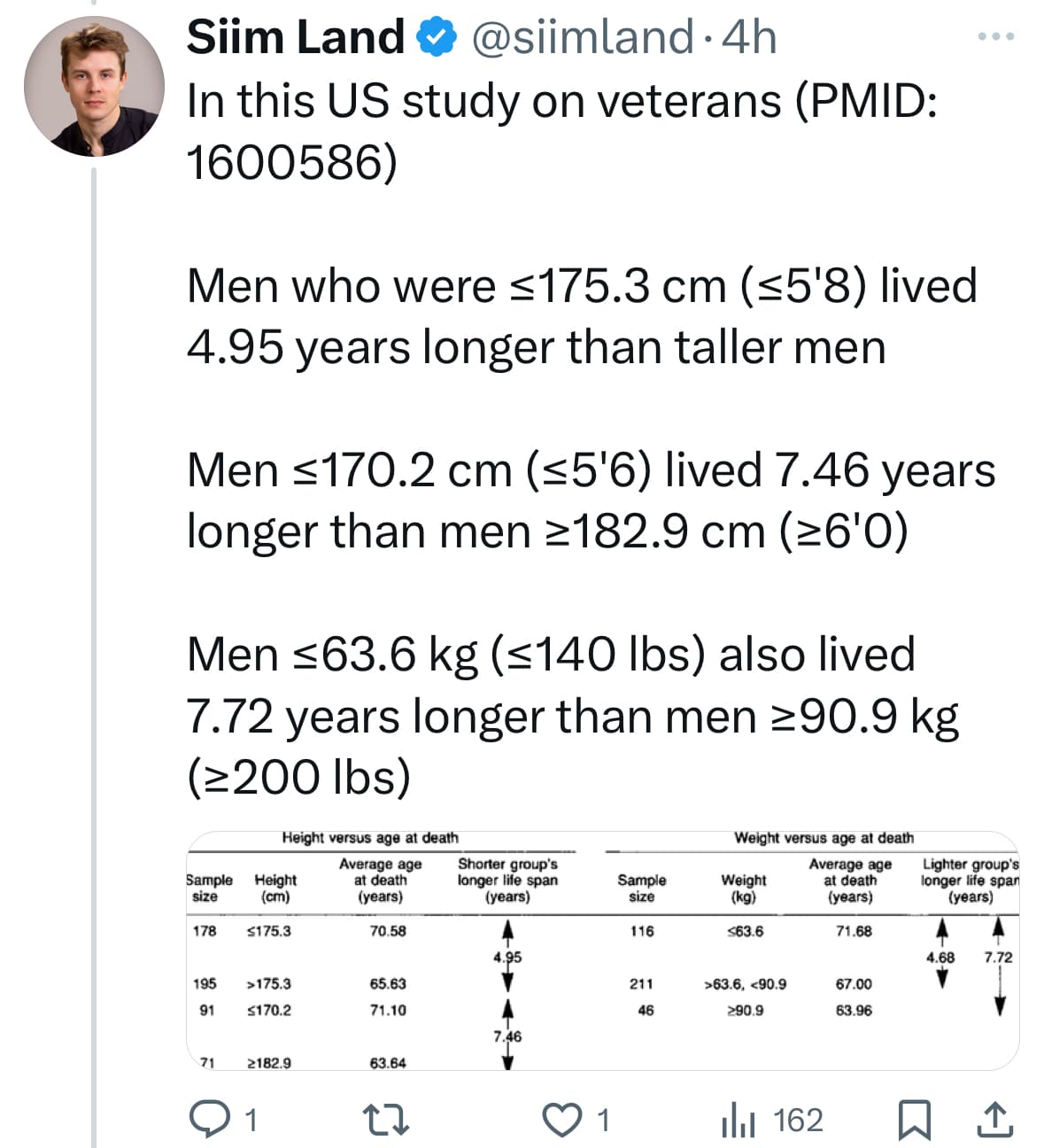
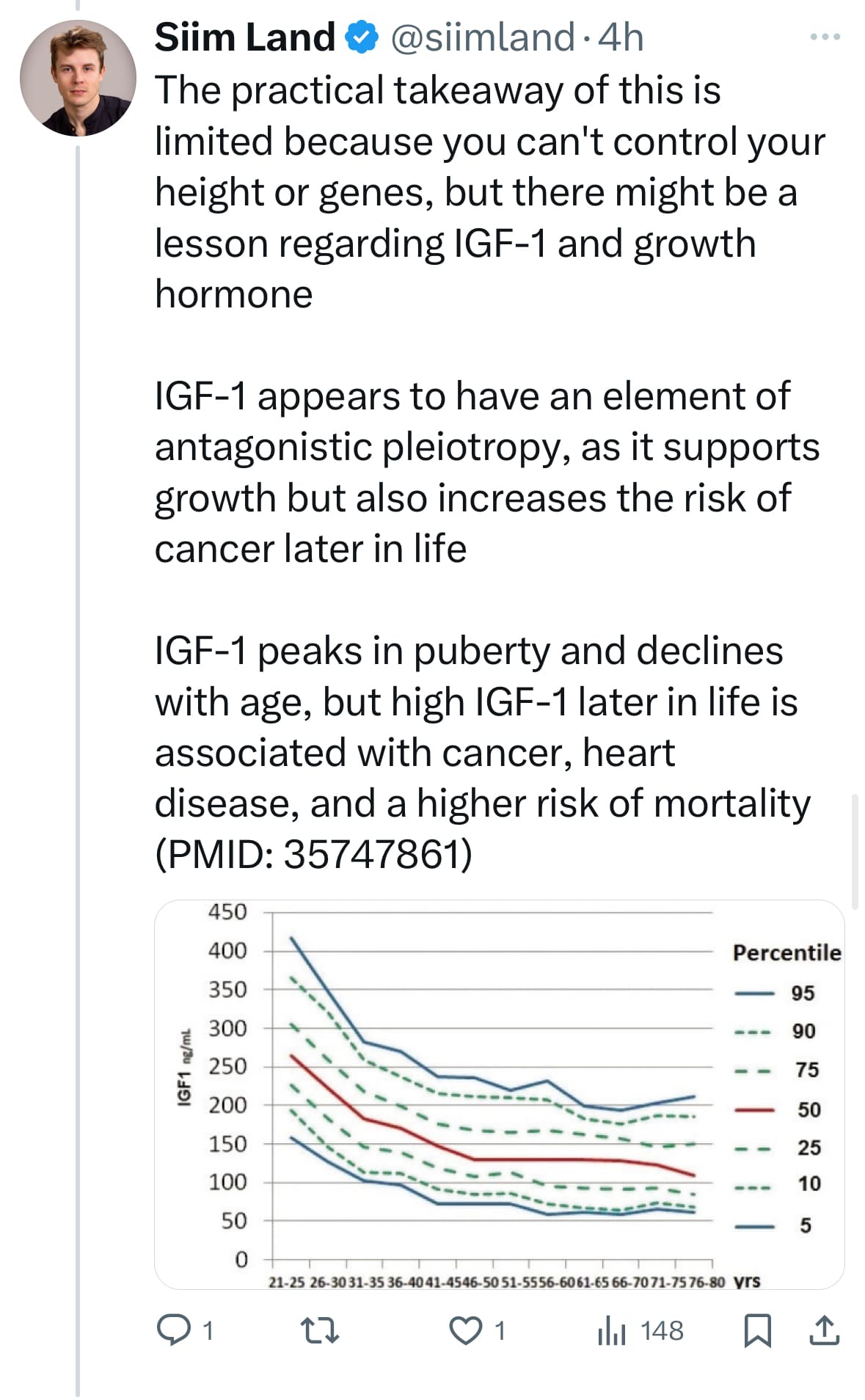
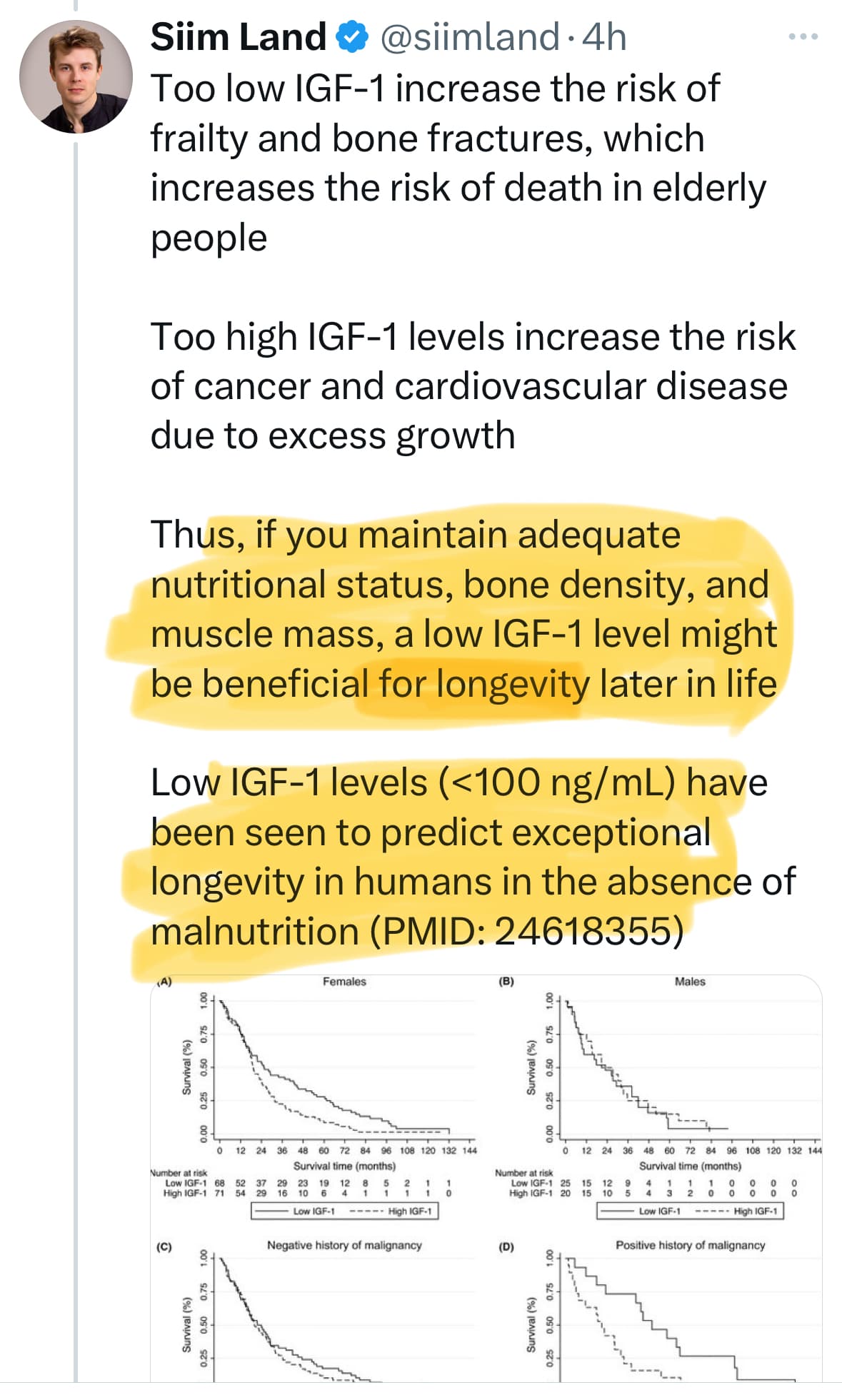
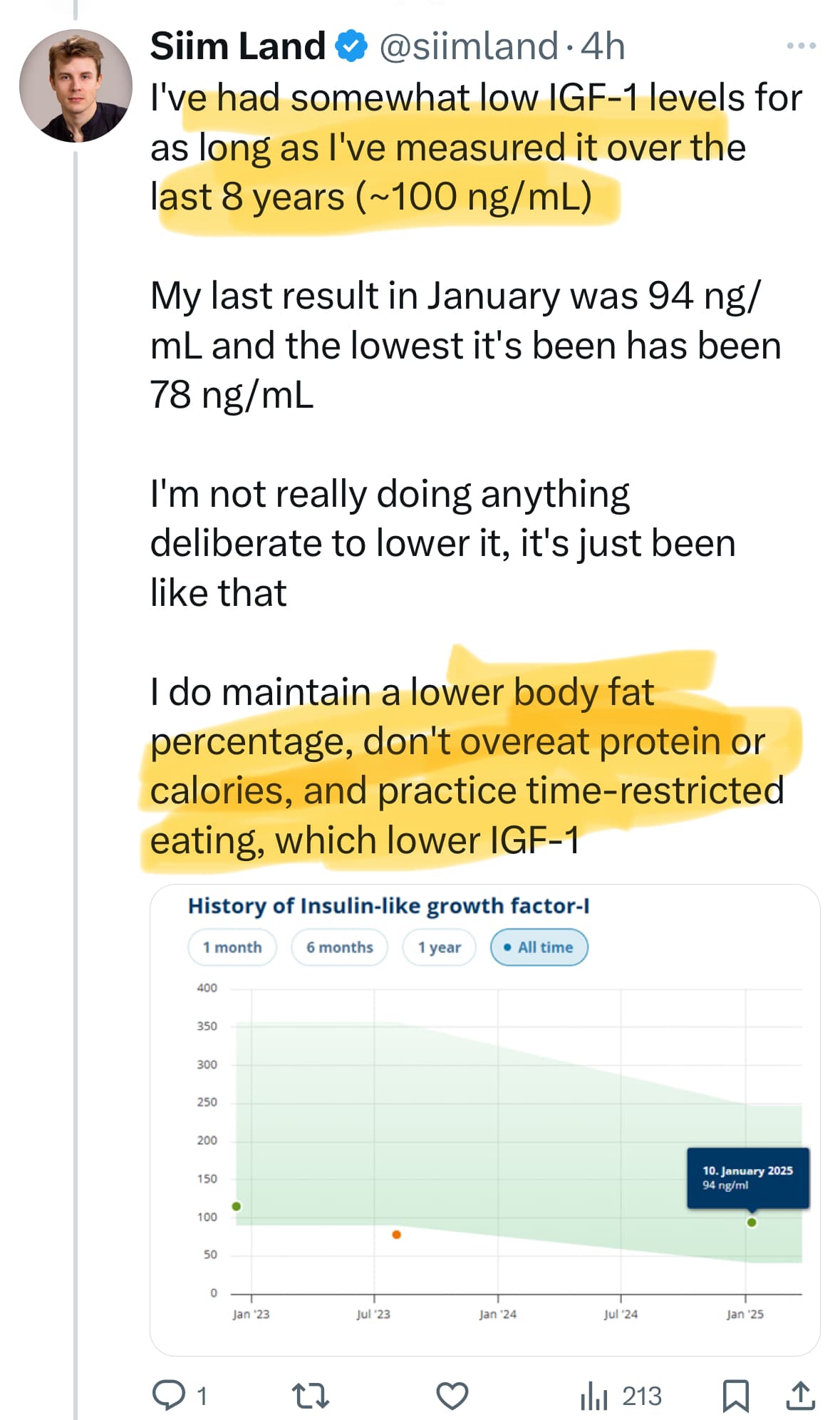

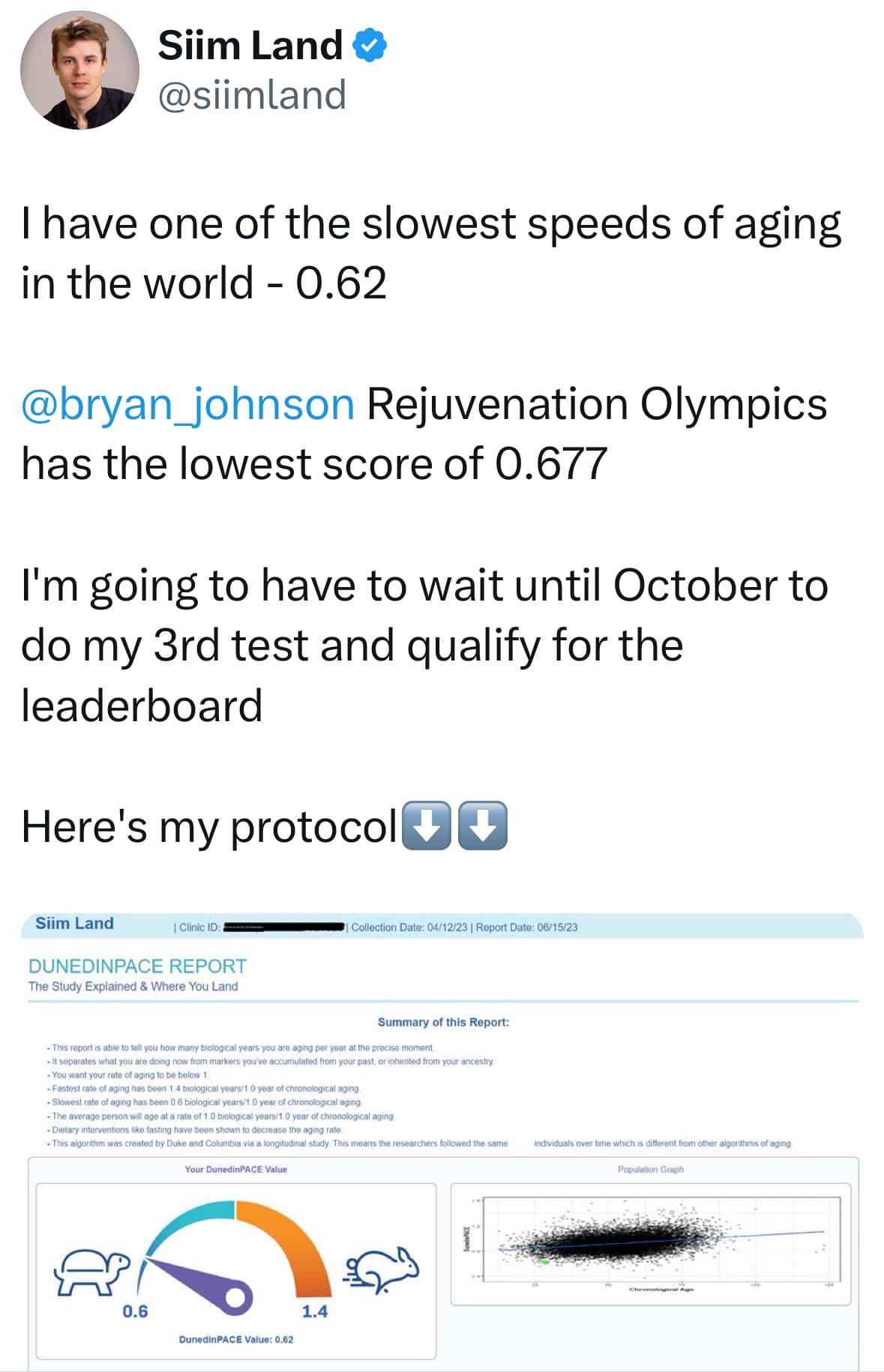
https://x.com/siimland/status/1913579283793993965?
And btw Steve - while N=1, he has low Dunedin Pace at least a while ago:
2 Likes
quality of life > marginally longer lifespan
2 Likes
@Virilius The evidence does not suggest that is the correct equation I think
Perhaps to be generous in that direction it might be
Quality of life now
<<<
Longer life and higher quality of life* later (and increased probity if intercepting powerful new therapies in a healthy enough state in the coming decades)
- like not cancer and dealing with the quality of life of the cancer itself and of chemo and radiation, etc
Are there any good cohort study tracking IGF-1 controlling for relevant confounding factors on different outcomes? Any MR study?
Seems directionally this can be answered what a good level is.
Your SHBG is quite high. So is mine. Why do you think that is?
@stealle It actually looks like it my be a good longevity phenotype to have somewhat high SHBG:
www.rapamycin.news/t/iron-an-underrated-factor-in-aging/6062/27?u=neo
Bryan Johnson’s is somewhat high to and look it to good excercise regime, being fit, lean, metabolically healthy and slight CR:
(For his values go up to the twitter link from @A_User a dew messages up from my message above
We know that a growth factor similar to IGF-1, sometimes called MGF (mechano-growth factor) is secreted locally during resistance exercise, so a systemic low IGF-1 really does not necessarily imply frailty in bones and muscles.
My only observation on your points is that you appear to neglect the IGFBP aspect. We should go into more detail, even as we should when discussing testosterone. The total amount is OK; it’s a reserve in the blood, but the available pool, the quantity that contributes to growth signaling, varies according to the amount of binding to specific proteins, as we’ve seen in some of the preceding posts.
However, I agree that if big data suggests better longevity with low total IGF-1, a lower total IGF-1 probably corresponds on average to lower IGF-1 signaling = free IGF-1. On average would be the key word.
1 Like
-
Vitamin D dosage ≤1000 IU/day significantly increased IGF-1 levels.
-
Intervention duration ≤12 weeks significantly increased IGF-1 levels.
-
In cohort study, under 60 years subjects with a higher dietary vitamin D intake had significantly higher IGF-1 levels.
The influence of vitamin D supplementation on IGF-1 levels in humans: A systematic review and meta-analysis
https://www.sciencedirect.com/science/article/abs/pii/S1568163719302302
2 Likes
Btw I noticed a reference to this study on an older thread, which showed a doubling of the independent CVD risk factor Lp(a) after GH replacement therapy in GH-deficient adults. Might be worth monitoring for those who are using GH or GH-releasing peptides:
3 Likes
The discovery of HGH-related CJD quickly led to the end of cadaver-sourced HGH in the U.S. and other countries (thankfully, synthetic HGH became available soon after). Still, over two hundred cases of iatrogenic CJD—iatrogenic meaning it was caused by a medical treatment—from tainted HGH have been documented worldwide. Most of these cases were reported between five and 10 years after people had used HGH. But prion disease can sometimes take much longer to manifest in certain people, even decades.
According to this latest report, the woman first visited doctors with tremors and trouble balancing. As is often the case, once symptoms started, her condition rapidly worsened. She was hospitalized just four weeks later, and several days into her stay, she fell into a coma that she would never awaken from.
An autopsy confirmed the woman’s death from CJD but ruled out known genetic causes. And since she received HGH treatment prior to the cadaver ban, it was likely the root source of her illness, the doctors concluded.
1 Like
I’m probably the only one here with an anecdotal experience on this. Having checked my Lp(a) a few times, I have not seen any real difference in it whether I have taken HGH or not.
6 Likes
Reducing IGF-1 is not guaranteed to increase “life span” (although it’s more about health span)
Tim Proctor - via X-com
Mitochondrial mutations may impose a hard limit on lifespan
Reducing IGF-1 signaling, a known lifespan extender, completely failed to extend life in mice with unhealthy mitochondrial DNA
mtDNA health could be the foundation for many other hallmarks of aging
5 Likes
From discussions above, is the low igf1 camp talking about chronic inhibition of igf1, or something more intermittent?
For me, if it’s between having chronically low igf1 and retaining muscle and bone mass so I can hike in my 70s, I know what I’ll choose. I liken it to mtor inhibition in that sense.
1 Like
This is a million dollar question, in my mind. Can we “have our cake and eat it too” by keeping IGF-1 in the high-normal range and then periodically do (for instance) 5-day fasting-mimicking protocols to temporarily decrease IGF-1/insulin and clean out the sludge/reboot the system?
3 Likes