Too much time on hands, clearly
I’ve spent more time looking at this issue with Ezetimibe. I now see that in the VA study, both with and without CAD in Vivo … significant differences in dementia rates. This meets as good a criteria for consideration as GLP-1’s, SGLT2’s and Rapamycin, on a superficial review. I’d however look at my further comments on this after a researcher, biostatistician, epidemiologist reviewed this article.
If the effect is real, the only explanation I can come up with, is that it must cross the BBB, as the peripheral effects don’t make any mechanistic sense to any signaling to the brain like with the GLP-1’s, and interestingly in the study, seemed like more folks on ezetimibe developed coronary artery disease. This could be confounded by ezetimibe not lowering cholesterol in the brain (but then it’d not cross over the BBB) and the other folks doing worse, presumably principally on statins. However, the associations with statins and dementia don’t seem to indicate increased risk.
This is the beauty of the forum, getting exposed to things that aren’t in the mainstream and getting a chance to investigate.
The risk of this medication is very low, so adding it is sensible, but we need more data on this, as the current article has some significant flaws.
12 Likes
It’s also possible — and I say, merely possible — that there could be a hidden intermediary that we don’t even know about, an unknown unknown, unrelated to ezetimibe’s primary and studied mechanism of action. No one will know for sure save from RCT and even those might yield a false negative if it turns out that ezetimibe needs to be taken for many years or decades to have this neuroprotective effect and it might also be something that can help prevent, but no cure. We’re all merely debating what constitutes a reasonably well placed bet and what doesn’t.
Again, I picked NVIDIA at $9.87 ![]()
2 Likes
That is a good thought. Just like alpha klotho doesn’t get into the brain, but induces platelet factor 4 which then crosses the BBB … who knows.
I secretly hate you for doing so well in the stock market. It is my nemesis.
5 Likes
I thought your nemesis was your cat? ![]()
1 Like
My now expanded set of 3 cats fail to cause the same pain as my stock investing choices.
I’m an expert in buying high and selling low.
5 Likes
Yes. Many people have the same problem. By the time you hear about a great investment, there’s a good chance the greatness has already passed.
Index funds are a lot better. Try VOO or QQQ. Buy and hold.
3 Likes
You are so smart that comparatively I feel ridiculously dumb, so you can imagine the comfort this new information brings me.
I’m sorry for your pain, but as a retired stock broker, I”m thrilled there is one thing I am better at than you, well, that, and most likely cats ![]()
3 Likes
I scoured the Drugs@FDA pharmacology reviews for ezetimibe and it seems like it is not crossing the BBB, as there was none in the brain of rats.
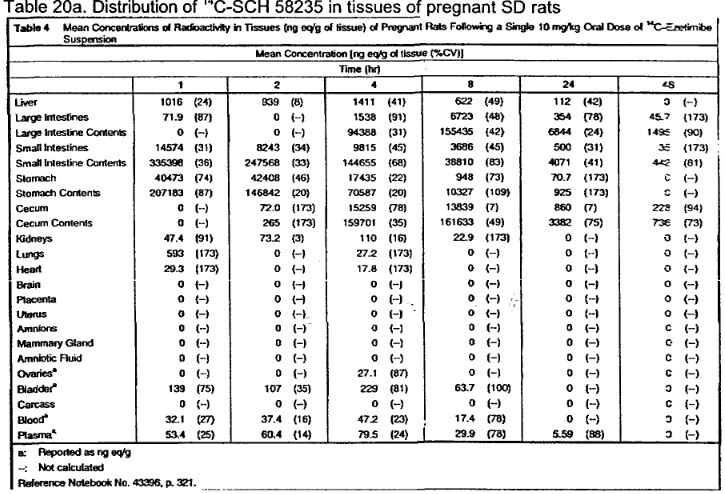
It is also conjugated in the body (90% at 0.5 hours).
4 Likes
Apply to the stock market the same principles you use to evaluate likelihood of benefit in a drug or intervention and you can’t do too poorly.

I started late 2019 but really got serious during COVID. Have liquidated maybe a third of the portfolio’s proceeds since to pay for a house so the effective return is quite a bit more than 400%. It’s not about hearing of something cool, some “hot pick” — I never ever watch market news shows or read “insider scoops”. That’s like buying a new supplement because an influencer touts it. Gotta look at the mechanism of action, do your own research. The rules of thumb I used in my initial big buys during COVID were so simple: basically I looked at historical data before everything crashed. If a stock was on the up and up for 5 years prior, more or less, but tanked with COVID, my bet was that it was going to come back eventually. And that bet alone dictated most of my picks. When there were a few bouts of panic since, and blue chip stocks dipped, I bought them. I forgot why I picked NVIDIA but I can tell you I didn’t even know what they made when I did. It was from looking at some internal trends. I might have a good intuition for this stuff. Hope it carries to my biohacking interventions.
3 Likes
Relevant article that goes into AD drug development:
The biggest thinking error I’ve seen in twenty years of investing in, creating and taking
over biopharmaceutical stocks is probability based. There is a prevailing and incorrect view of
clinical trials. The idea that a clinical trial is to determine “whether or not a drug works” is
partially correct, but misleading. For amateurs, this definition conveys the idea that chance is
involved. That perhaps this experiment may randomly work out, and the stockholder will become
rich. This is wrong.Clinical trials, done correctly, are deterministic. There is no chance. The outcome is
preordained by the laws of physics: the chemistry of the drug, the biology of the patient, the
medicine’s interference with the disease pathology. The carefully designed statistics allow us to
blend away individual differences, the minute randomness that exists. If there is a potent effect: it
will be seen.Just because a process is deterministic does not mean we can always understand it ahead
of time. Simulating the physical interactions which lead to the outcome of the throw of a dice is
beyond our greatest supercomputer. Too many atoms doing too many things for too much time.
But we can apply what we know about the world to experiments to see what likelihood exists. In
a few lines of Python, we can accurately simulate the random behavior of a dice without thinking
about atoms of physics.A simple example of how logic works in drug development: a drug that does not cross the
lipophilic blood-brain-barrier will not be able to influence a brain disease. Why not? The drug
can’t get inside the brain, where the disease is happening. Another: a drug that is metabolized
quickly into an inert metabolite that has no affinity for the key drug target cannot work. Why
not? The drug has transformed too quickly to interfere with the target protein.
1 Like
We’re getting in the weeds now. But sure, why not?
I’ve read Nassim Taleb on randomness in my early 20s and more lately Stephen Wolfram on computational irreducibility and the like, so the weeds are familiar territory, but I don’t want to merely rehash other people’s thoughts.
I meant the word “likelihood” to loosely mean, “epistemic confidence.” We make decisions in the absence of perfect knowledge ALL the time. I don’t mean that if we keep rolling the dice on the hypothetical perfect, decades long RCT on ezetimibe vs. Alzheimer’s we will get different outcomes in different branches on the multiverse. Indeed, it either works or it doesn’t, but we don’t know which, and in the absence of clarity on that issue we can presume the outcome, to be positive or negative, for the intents and purposes of taking vs. not taking that drug with Alzheimer’s protection in mind, and do so using proxies to the actual knowledge which we lack. Those proxies can be a consideration of the side effect profile of the drug.
Say, assuming that it does diddly for Alzheimer’s, will it be much worse than placebo, can it hurt? From what I understand of it, it’s highly unlikely to harm any individual. And here “unlikely” is used in the probabilistic sense, when we use it in general, even though my own specific biology is deterministic as I am not an average of all gene variants and phenotypes of humankind, I am a unique human female, of a unique molecular composition, and Zeta will either not cause me side effects or it will. At any rate they’re presumably easy to detect and reversible. Even better, it has positive effects on lipids and since I’m apoE4 that should be my choice of intervention anyway for lipid optimization, in preference to a statin.
So that’s my intellectual liver’s “first pass” metabolism of risk analysis. But if the risk profile is concerning, I proceed no further.
Next, I look at the data at hand. Was the observational study well conducted? To be honest I grow lazier and lazier every year and outsource much of the nit picking to this group. If there was something truly wrong with it I’d expect @adssx or someone of his caliber and obsession with detail to point it out.
Next, I look at the effect size. p-values are one thing but I don’t live and die by them. More important, presuming for the sake of argument that the drug DOES have an effect, is it going to make a true difference or be a rounding error? In this case there seems to be a massive effect size. That’s encouraging.
Last, I look at plausible mechanisms of action. And I say PLAUSIBLE. If zeta did cross the BBB then I’d look little further and presume it did something in the brain. Suppose it doesn’t cross it? Well, first I’d take that with a grain of salt, as our knowledge of whether it does or doesn’t is imperfect and can be further enlarged. But even if I take for granted that it doesn’t, there are other ways it can nonetheless POTENTIALLY exert influence on the brain, some of them I’ve already touched on in principle. And I go back to my being a unique individual — I have apoE4 which is known to cause a leaky BBB, so maybe zeta barely crosses the average person’s BBB while having substantial penetration into MY BBB.
At any rate, I have to remember that I cannot, through didactic logic, arrive at any hard and fast conclusions here, because there’s so much about human physiology that we won’t understand. There’s unknown unknowns there, that should be accepted as a given and give us all a modicum of epistemic modesty when we approach these things. I don’t expect the solution to Alzheimer’s to be anything obvious. If it were it would have been found already. And we can’t be overly reliant on mechanisms of action, since we don’t even fully understand its pathology. Recall if you please how a dogmatic adherence to certainty vis-à-vis its source (amyloid plaque and tau protein) ended up leading researchers astray for decades, spinning their wheels. I don’t even fully understand HOW it is that apoE4 confers higher risk. I see hints at multiple mechanisms but no smoking gun. And I’ve read about this extensively as it honestly freaks me out and keeps me up at night if anything does.
So… am I taking zeta?
No. I’m nursing a baby and if I apply my loose “algorithm” of risk analysis to her wellbeing it’s “unlikely” to be a wise choice until she’s weaned. Again, it might be totally fine and in fact it either is or isn’t. It’s a deterministic outcome. But I don’t know it. I’m erring on the side of doing no harm.
When she’s weaned I will get on it for sure.
4 Likes
It will prevent vascular dementia that’s not an insignificant amount of dementia cases by preventing atherosclerosis in the arteries around the brain. I don’t think it crosses the BBB, and it might be rapidly conjugating to another form.
The study seems to use ADRD (Alzheimer’s disease and related dementias), which might not only be AD. Why there were 5 cases of ADRD rather than 40 is interesting, but it seems like a small sample size to me, and some of this reduction might be explained by prevention of atherosclerosis.
Using everything which has a low chance of working might lead to a lot of time, attention, and effort to dead ends, a form of Pascal’s mugging. But it does work to prevent vascular dementia.
2 Likes
Also Martin Shkreli would not be my first choice, or second or third, of someone to emulate in making the right decisions for himself in the face of epistemic uncertainty. I am from the same culture as him and understand his psyche pretty well. Very intelligent guy but out to lunch. He couldn’t keep his ass out of jail but he knows “with certainty” this or that?
2 Likes
The effect size though cures a lot of sins. Hard to see how it could only be from vascular dementia. And again, nothing is certain about whether it crosses the BBB of someone prone to Alzheimer’s.
- Thanks a lot but you overestimate my skills

- Unfortunately I also outsource a lot of my brain power to this community

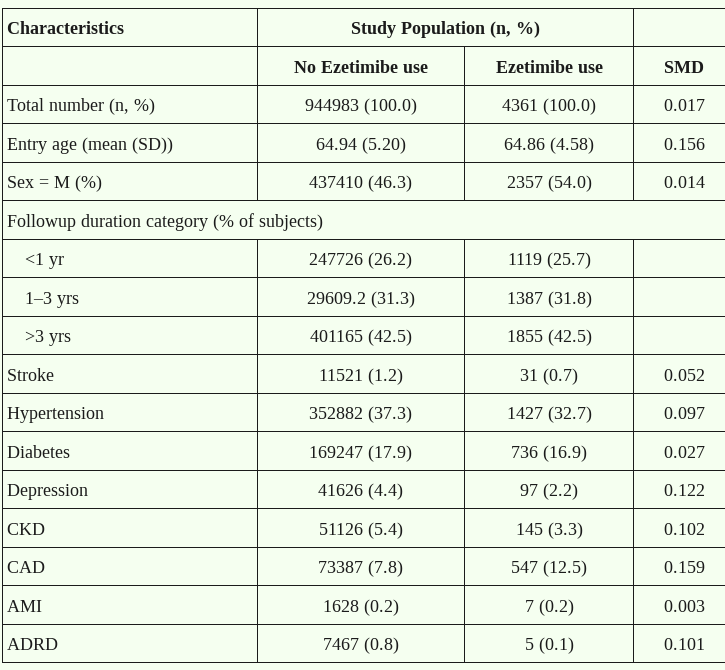
- In fact, I think that their observational study is far from perfect. They looked at all people with CAD and compared ezetimibe users to age-matched non-users:
First, the number of ezetimibe users is tiny: 0.7% of all CAD patients! Who are these people? Maybe it’s just the patients of doctors who read this forum and know that low-dose combination is better ![]() And these doctors might have richer, healthier patients. Ideally, we’d like to adjust for not only age but also sex and income.
And these doctors might have richer, healthier patients. Ideally, we’d like to adjust for not only age but also sex and income.
Second, are these 547 patients using ezetimibe only? Or ezetimibe + a low-dose statin? If they’re on ezetimibe monotherapy, it means that their LDL baseline before treatment wasn’t so bad, probably borderline normal. We want data adjusted for baseline LDL.
This inability to properly adjust potential confounders explains the incredible relative risk of 0.122 (C.I.: 0.02‒0.88; P<0.006). The CI is wide. If the real relative risk was really 0.122, we might see signals in clinical trials but:
So I assume that the relative risk is closer to the upper bound of the CI, so 0.88. This would still be great!
I think that ezetimibe is great and should be used more often for cardiovascular health. This paper is a nice potential bonus for ezetimibe users. But let’s wait for more data…
7 Likes
Thank you for providing this information - this data in rats is at least is indicative.
The design of the paper only really makes sense, if the action is taking place at the site of protein aggregation in the brain (that is: local inhibition). Even if EZ is performing activities outside of the brain which benefit AD development, it would not play to the strength of the paper the authors try to build up to.
I wonder if in humans it may still be able to penetrate the BBB - not because if limitations of the rat model, but given that blood-brain barrier disruption seems to be a common feature of early AD development (before the onset of neurodegeneration).
1 Like
But why are you limiting your statement to the subset-analysis of the observational part? Instead of the full sample which the authors analyse?
There are 4361 users of EZ and almost a million non-users in the dataset. That’s a very large number - certainly sufficient to deliver statistical power in their regression analysis (which they DO perform, adjusting for available confunders - not just age!)
The relative risk for the full sample of 0,14 accordingly has a much narrower spread of 0.06 – 0.34, P<0.0001
As for randomized trials: the average age of people in Improve-IT was 64 with a low spread. The average age in the PCSK9 + ezetimibe/statins trials was 58 ! The typical age of onset for AD is 74 - so how do you expect to receive any useful data from an analysis of clinical trials for ASCVD?
.
.
.
We lack useful RCTs - which is a common feature for almost all AD interventions (the LATTICE trial for lithium is uncommon). So we are faced of having to make guestimates based on the best available observational data. The easiest step for EZ that does not require waiting for 5-7 years would be to try to replicate the finding in an another, independent observational dataset - like the UK Biobank.
1 Like
So I’ve had a cardiologist who is a biostatistician and researcher review this article. This is the review:
Methodologically it is a pretty horrible paper. Much of it deals with laboratory work involving nematode cells expressing human genes, and also human neuroblastoma cells. I am no expert in all that, but it is clearly a fairly long way from human neurons and astrocytes. Their work may well raise interesting questions but hardly more than that.
Then there is the clinical work, which theoretically is much closer to a proof of principle type of investigation. But the details of that are so scant. How was this database gathered? Apparently by some pharmaceutical consulting company (IQVIA), that contracts with several drug companies—am I correct? It is critical to know much much more about this database and particularly a much more detailed comparison of many variables between those receiving Zetia and those not. Further, in the statistical methods there is no evidence given of the analytic strategy used. Later it is stated as a “time-dependent regression model”. Did they really know what they were doing—impossible to tell.
So, I would interpret that as “interesting to further watch this space” but this level of evidence is impossible to evaluate. Zetia is pretty easy to take-particularly if lipids high, but not sure I would bother based on this.
8 Likes