I’m all for an informed patient and sometimes patients point out things I don’t know. The problem is many “informed patients” still have a huge information asymmetry.
It’s like you trying to develop software right now as a non-SWE. I assure you - you can google/StackExchange how to do some lines of code but you can’t know what to google right such that Google literally offers you the secret foobar invite I got because they think you’re exceptional at coding. (I can prove it to rapadmin privately)
There is a lot of information and misinformation.
Without medical school with 12-16 hours a day of a million “boring” associations, organizing information into the correct hierarchy of knowledge, and tons of clinical experience with complex patients to develop a keen sense of what to look for - I assure you it’s the same issue - you might read something, but it might not be applicable or it’s part of the replication crisis etc. I see that all the time with PA/NP midlevel providers who are overconfident because they have “decades of experience”. We’ve tried taking Step 3 medical board exam questions intended for MDs for an NP licensing exam for these “decade-long experienced NPs”. Most failed miserably and this is quantitative, objective evidence but they wanted the money so bad the NP board scrapped it and made licensing way easier. At least the ones from online degree mills with 100% acceptance rates tend to be more receptive and humble to just staying in their lane. But you will see way too much pushback with cherry-picking research saying NPs are equivalent or “better” (hint: they used BS metrics like patient satisfaction and uncomplicated, non-complex patients if you actually read the research in depth), on top of lobbying from private equity firms who want subpar providers to order more unnecessary labs and consults with lower labor costs. I find it absolutely horrifying that many patients (even here) still believe in midlevel providers as independent practitioners. And I really don’t care about competition and all the other stuff people will claim as personal bias - I’m aiming to be a geriatrician - the fellowship itself is pretty uncompetitive and very lowly paid with more than half open spots. I’d probably get paid less than some PAs in derm, but I could care less - plus my SO makes more than enough income for both of us as a Google “senior engineer” (I can prove this to rapadmin privately to settle this since there’s a healthy amount skepticism on my claims, which admittedly are relatively exceptional)
If I wanted to get paid more and worried about the competition from mid-levels, I could have just aimed for derm with Mohs surgery or ortho spine surgery to churn out procedures, instead of geriatrics which is primary care and lower paid than a general practitioner - because I have already accepted that I can’t change the private equity lobbying and the patient safety issue will eventually implode in a decade or so. I’m just going to save who I can who is growing old and eventually become a geriatric patient - me, my friends and family, and everyone who is willing to hear out the objective evidence I have to present my positions in a sea of noise and misinformation. I could care less if my pay is cut by 20%-30% because I end up in a research role.
“He who studies medicine without books sails an uncharted sea, but he who studies medicine without patients does not go to sea at all.” Sir William Osler
Regarding strength training, I think the volume and frequency required to stimulate adaptation is vastly lower than most are prescribed. For example, I do a single set of (now weighted) press ups every fourth day. That’s less than 2 minutes for the entire week yet I have improved the weight, or number of repetitions performed, practically every single session since January. I recently started applying this same protocol to pull ups. To reiterate, a single set every fourth day. Progress here has been slower as a single repetition amounts to a greater percentage increase but never-the-less I’ve increased every fortnight or so and gone from 5 to 14 reps.
This very simple ‘program’ effectively hits the entire upper body in only 3 minutes per week.
Depends on your goals. I want to be “bathing” in nootropics, not just look good naked.
So for me, it’s the “dosing that’s the therapy”…combined daily aerobic and resistance time x volume interaction. Having said that, my own goals is I want to increase muscle mass, strength, tone full body for more reserve going into the later decades. But your experience, no doubt real and one alternate.
I wasn’t maintaining 6%. It was a short period of time just to prove a point to my clients who complained they were “ectomorphs”. I have a small bone frame but I pulled it off.
It was just a phase of my life where I wanted to see how far I could go to prove to my clients (many of them are Asian) it is possible.
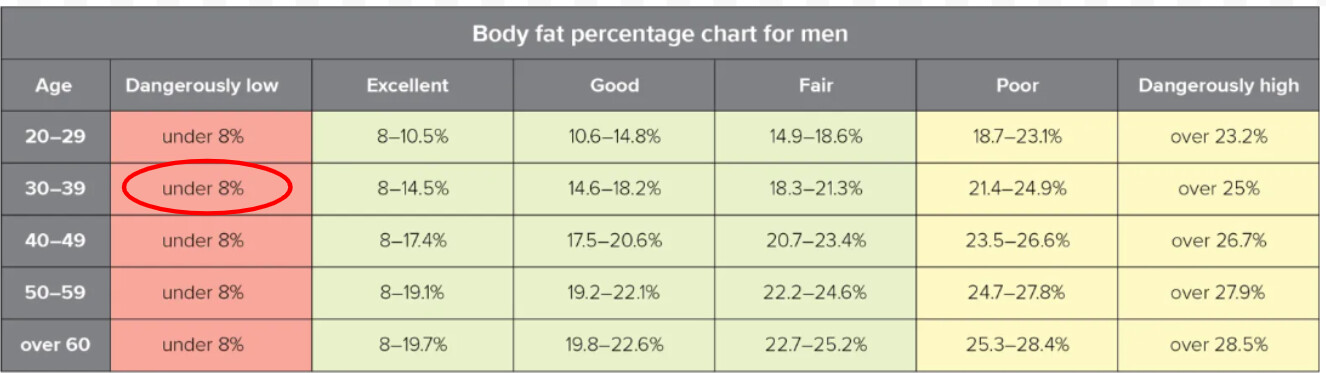
I’m currently 11% and I know that’s very roughly where healthy lies.
A bit more than 6 feet. I don’t want to put my exact info for privacy reasons as I have psychiatric disorders (ADHD) although I suppose a private investigator could figure it out.
I get the broader systematic exercise benefits from the bike (6 to 8 hours per week).
If repetitions are increasing then you are getting stronger. And if you’re getting stronger then, after the initial period of CNS adaptations, you’re adding more functional tissue.
If you don’t believe me that’s fine I don’t really care that much - again I can submit proof privately to rapadmin if you believe an independent vouch to settle this issue quickly - this saves us all some time arguing whether I actually hit a semi-pro level of natural bodybuilding without anabolic steroids (or hGH) when I don’t even care about hypertrophy currently, nor do I have any goods/supplements/affiliates or personal trainer services to sell you.
All excellent. But don’t underestimate the nootropics of resistance exercise volume as a master brain signaller. Why I don’t make a singular bet, do them both with volume x time.
If I happen to pass by my free weights in the pm (fasted all day) and just grab the 25lb barbell and do a good set…as soon as I am done, my liver goes haywire. I get a HUGE pang signal.
My feeling is that strength training again before super compensation (not just recovery) occurs interferes with the adaptation from the initial stimulus. So there’s a chance you just ‘spin your wheels’… Though that’s irrelevant if you’re strength training to minimise cognitive decline rather than maximise lean tissue. (I have a family history of dementia so am very sympathetic to this idea).
This is really my goal…to prevent cognitive decline with age. Of course, the CVD and cancer benefits are thoroughly documented as well…leading to the only metric that matters, all cause mortality. But for me, if I loose cognitive…I’ve lost. A longevity statistic from that point onwards is meaningless.
I have not looked at this issue… But is there a validated model of the optimal type of exercise for the best long-term brain health and cognition, in terms of percent or time per week doing strength training, HIT, zone 2, etc?
Thank you for specializing in geriatrics. The world certainly needs more and the need will be growing almost exponentially.
This is the observation of an “old” man: We are basically invisible to young people, old people too:
I can tell my primary physician is not interested in my opinions and I only use him to get my prescriptions for metformin, Flomax and tretinoin refilled.
As I told my late wife when she was worried about her appearance when we were going to the supermarket: " We are old and mostly invisible. We notice young attractive or striking people and probably will recognize them again, but seldom remember the “old lady” in front of us in the check out line."
But, I also notice that there are many young people wanting to help me if they think I am trying to lift and load something they deem too heavy for someone my age
Thank you. And also glad you are sharing your experience.
As you seemed to have implied - old people tend to get more invisible, and ageism tends to set in - especially in engineering, which it appears you are in (there’s reverse ageism in medicine, though).
I found it utterly horrifying that many practitioners chalk up dementia signs to “normal aging” and I’ve seen way too many older folks that clearly have MCI/early dementia with positive MoCA on anticholeringerics prescribed by a subpar provider when it is very much contraindicated.
Even worse is the nursing homes puts them on haloperidol and restraints while with MCI/mild dementia because they spend less on labor. And you’re paying 100k+ per year for bare-bones nursing homes and ~250k+ per year for assisted living with memory care. You’ll go broke quickly even if you are a millionaire.
Nearly none of my colleagues (at my age) are even thinking about how the heck they are going to deal with the horrors of LTC in the US.
If you are skeptical, feel free to watch this PBS Frontline documentary of the for-profit LTC industry first and then do a bit of research. I really hope to be proven wrong.
I’ll also add this short rant, so you can do your research to find the right team of physicians and experts or refute my claims - geriatrics is a highly complex field but highly underserved (not even that much of a financial issue, but an awareness and access issue) - most patients are on a complex arrangement of meds with different physiology, and nearly nobody is the arbiter of truth when it comes to legitimate “anti-aging” where it is mostly guesswork as you already can see for yourself. It’s even worse than finding accurate information on effective dermatology-related prevention with all the industry bias, sales, and hearsay that seeps into dermatology practice. Even derms are joining multilevel marketing schemes for skincare products of questionable value.
Few physicians are qualified to look out for geriatric patients (as you can see with the examples of highly common contraindicated meds), and the average geriatric patient tends to be unaware of it. Many of the brightest minds tend to go into dermatology practice to make more money, and a sizable amount of geriatricians are hiding their fellowship credentials to earn more as a general practitioner.
It’s not much surprise there is a direct correlation between $/hr and procedures rather than complex clinical thinking, which is paid very low (not everyone, but a good amount of physicians) if you look at official statistics. And then few physicians are satisfied working with patients who are mostly dying where there is not much you can do to help besides complex med management/missed diagnoses. I’ve literally seen a cardiologist recently putting a geriatric patient on a beta blocker (ultra common med in cardio) and caught that as a reason for new onset psychosis, so the primary team wouldn’t throw antipsychotics unnecessarily. If nobody spoke up (pretty common), this patient would literally be on the inappropriate polypharmacy train with no capacity to make medical decisions against antipsychotics which has plenty of nasty side effects.
However, I think that will eventually change when the FDA finally has a new paradigm on disease definitions in a decade or so and Medicare eventually has enough pressure to do medicine right when the official statistics are undeniable to even the non physician bean counters
Validated? I don’t think there is a “clinically” proven model. I just immersed myself in the cognitive/exercise literature and settled that I absolutely needed to do both regularly.
For cardiovascular remodelling, which I extrapolate to the brain, you want to be Zone 2-3. My MHR is 220-57 = 163. 70% is 115 bpm, but I normally do my daily aerobic at 125 bpm. My cardiologist I recall advising to stay below 130. The 10,000 steps thing, sorry but pretty much meaningless interventionally speaking.
For resistance, that one is more nebulous. I’ve just distilled it out as a full body workout with growth in strength and musculature over time, no hard target. For me, this is about 30-45 mins, including rest between sets. I could do less by focusing on certain muscle groups, but I just personally prefer the whole body workout. Of course, I balance against how I feel, recovery, sleep, tiredness, muscle aches and pains. Would dial down if I was starting to impact any of these.