After the Blagosklonny article, I find myself (hopefully excessively) focused on the mtor rebound effect. If it applies to rapa, it would seem possible to apply during the eating festivals…
2 Likes
Frankly, this article is not really useful from a practical point of view. It’s a nice intellectual exercise, but with no experiment or data to back it up. Before worrying about rapamycin optimal dosage, I have other more actionable stuff to hang on to like exercise, diet, and sleep.
5 Likes
Please ask it to provide links, at the very least. Using this program for medical advice is like Russian roulette, at best.
3 Likes
Here’s the relevant quote from his recently posted article.
“However, intermittent therapy may have some disadvantages. Such schedules include drug-free periods. During these periods, mTOR can be over-activated in compensation and may, in theory, cause acute harmful events. (I believe that rebound of mTOR in endothelial cells may increase thrombosis, arterial permeability and arterial spasm)”
1 Like
I’ve not heard much of this, and I think we need another topic just on this and to review the research on this. I don’t know how much in the way of good studies have looked into this…
3 Likes
I imagine you saw the Blagosklonny comment the other day. I find it pretty concerning.
1 Like
No - I seem to have missed it. Please post.
I posted it above. Here it is again:
"“However, intermittent therapy may have some disadvantages. Such schedules include drug-free periods. During these periods, mTOR can be over-activated in compensation and may, in theory, cause acute harmful events. (I believe that rebound of mTOR in endothelial cells may increase thrombosis, arterial permeability and arterial spasm)”
2 Likes
Ah - I was unclear what you were referring to. Yes - have seen that, but he provides no data supporting this theory, so its hard to put much value in it as yet.
This is a new theory that nobody else has proposed, to the best of my knowledge, and no supporting data. Blagosklonny knows a lot about mTOR and cancer, but he’s not an experimental biologist so doesn’t actually get involved in studies, doesn’t run a lab. I would like to run this hypothesis he has by people like Richard Miller, Matt Kaeberlein, Dudley Lamming, Adam Konopka, etc… people deeply involved in the actual studies.
4 Likes
That would be great. Look forward to hearing more!
The main thing is we don’t really have any major certainty beyond the fact that Rapamycin taken intermittently has some known side effects.
I would think apart from the people who are coming off Rapamycin I am the person in this forum on the least frequent dosing schedule. I probably take more blood tests than anyone else on this forum as well as the usual measurements and running a fitbit. I am also coming off a CGM in less than 24 hours. I have not noticed an unexpected issue.
What we can useful do is to put together what semi anecdotal data there is. Blagoskonny does say intermittent usage may be good. Personally I think having a period of time when mTOR is not inhibited is quite important. Hence you have to work out a time when the effective dose is negligible and make sure that period is quite a while. I don’t think targeting the level at which you next take it is right as we are not trying to keep up the level, we are trying to ensure that mTOR is not inhibited for a material period of time.
Still careful experimentation measuring things with detailed records and reporting on outcomes sounds a sensible strategy.
1 Like
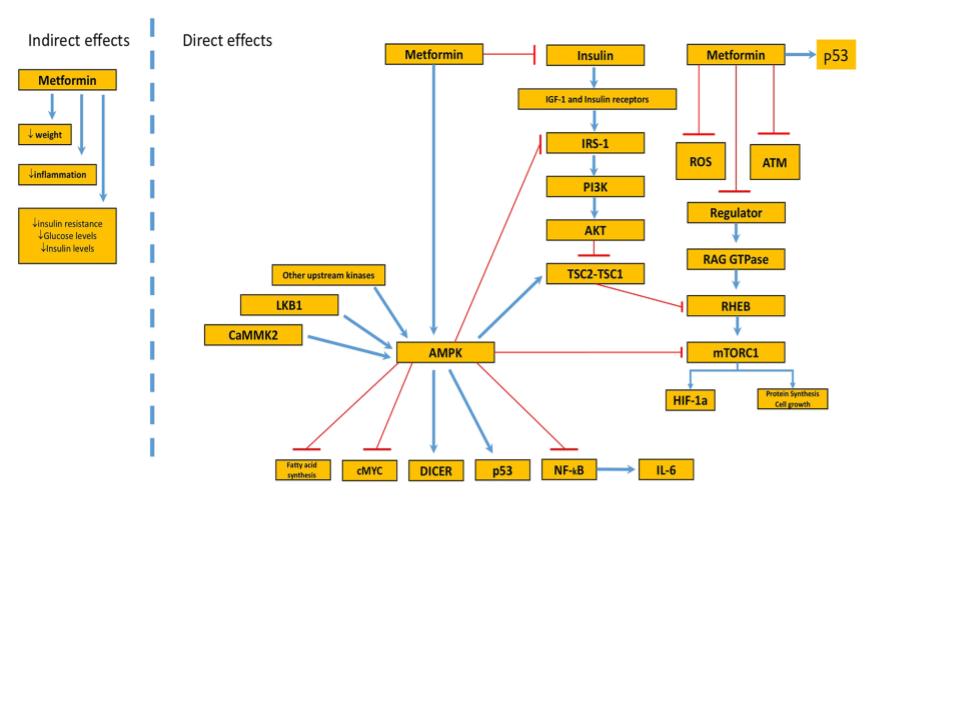
If Dr.Blagosklonny is correct perhaps we can use metformin to prevent the mTORC1 rebound effect from cycling rapamycin.
Here is one of many articles mentioning the mTORC1 inhibition by metformin in addition to its anti-cancer properties.
“It is thought that it exerts its anti-cancer effect through the inhibition of the mammalian target of rapamycin (mTOR) signaling pathway. Because of its effect on the mTOR pathway, there may be a role for metformin in slowing or reversing growth of life-threatening hamartomas in tuberous sclerosis complex.”
“The mechanism by which metformin exhibits its antineoplastic effect is through the inhibition of the mammalian target of rapamycin (mTOR) signaling pathway, by activating the AMPK regulator (adenosine monophosphate-activated protein kinase) and p53.”
“The journey of metformin from glycaemic control to mTOR inhibition and the suppression of tumour growth”
https://bpspubs.onlinelibrary.wiley.com/doi/full/10.1111/bcp.13780
6 Likes
May I ask how much rapa you feel is best & how long you think the rapa-free period should be? Much of Blagosklonny is like a riddle. We learn throughout his writings that rapa is the nectar of the gods & then out of nowhere we get hit in his most recent post with the ‘theoretical’ possibility it can cause acutely harmful thrombosis, arterial permeability & arterial spasm. I just took 6 mg’s yesterday but will probably abstain going forward until this riddle is resolved.
1 Like
That’s all very true, but he reads anything and everything having to do with rapamycin. The fact that he so specifically referenced endothelial damage and thrombosis as the rebound issues makes me think that he’s read or heard something specific in this regard.
1 Like
I don’t know how much is best. So far I have taken 2, 4 and 8 mg. I did not have any grapefruit juice or similar enhancer, however. Next time I am likely to take 4mg with an enhancer.
Personally I think weekly is too frequent as it does not leave enough time with mTOR uninhibited for it to do what it needs to do. A lot depends upon what the deminimis serum concentration of Rapamycin is and I don’t really know about that. I have not yet had any material side effects from Rapamycin although I think it did increase my blood glucose by about 0.5mmol/L (9 mg/dL) for a period of time.
I do a lot of experimentation with a lot of different things and take a lot of measurements.
2 Likes
But I do think this point is highly pertinent to the most central question about rapa. Whether it’s healthy to take long term. I’d think it wouldn’t be too hard to find out if there’s an mtor rebound effect.
There’s quite a few question in my mind regarding this matter, not the least of which is the definition of intermittently and how the definition of intermittently may vary based on the dose. The second question is how much mTor1 inhibition is enough to cause a rebound once it’s no longer inhibited?
The study of Everolimus to determine its effects on vaccines in humans used dosing of .5 mg/day, 5 mg/wk and 20 mg/wk. In Peter Attia’s podcast with Lloyd Klickstein, Lloyd said that mTor1 inhibition for the .5 mg day partially inhibited mTor1 in a sustained fashion, the 5 mg/wk fully inhibited mTor1 for a couple of days while the inhibition with the 20 mg/wk created non-stop inhibition of mTor1 for the full week, right up until the next dose. (The full conversation of this starts at 00:53:00).
This, to me, says that 5 mg/wk will allow inhibition to “wax and wane” and the 20mg/wk is full inhibition until you stop taking it. So, if there is a “rebound”, I suspect it would occur after full inhibition for a set period of time (whatever that time frame is).
I invite feedback on this.

4 Likes
Good thoughts. You’d think there would be some data out there that would help us on whether there’s a rebound & if so, what level triggers it. A daily dose of .5 would seem possibly safer on that front but of course I’m just guessing. Would it eventually hit mtor2? Or possibly trigger resistance? I calculate the steady state level at .5 per day would be about 2.4 at a 3 day half life. And, of course, how effective would that dose be?
Lloyd did go on to address the mTor2 question…he said that he would have suspected mTor2 inhibition would be an issue with the 20mg dose but he didn’t remember anyone discontinuing due to that reason…he did confess that it had been awhile, though, since he read the paper.
The .5 mg daily group and the 5 mg weekly had no real difference in adverse effects and the prominent one was, of course, mouth ulceration, with the 20 mg group having the highest incidence.
The study was on everolimus though so we’d have to make some pretty big adjustments.