I never got COVID when I was vaccinated. Protection lasted for a year. However, I have gotten it every year I did not get the vaccine. The only good news is that each time was milder than the prior.
5 Likes
Cognitive dissonance perhaps? Not one person I know who did not get the shot regrets not getting it… on the other hand…
1 Like
Seems like even the compounded effect alone is materials and should be weighted
We found that COVID-19 reinfection resulted in a roughly 35% increase in the incidence of long COVID in a matched cohort using observational electronic health records.
2 Likes
2 Likes

Well, many of those who might have regretted it might have got this instead: Herman Cain Award - Wikipedia
2 Likes
I don’t really pay attention to long covid. On the list of diseases to worry about, for me, covid is way down the list. Heart disease is probably 100x more likely to get me in the next 2 years than covid is. Same with cancer.
If people want to spend their time and energy avoiding endemic respiratory viruses, I don’t mind. That is up to them. I am not planning on masking, isolating, boosting, etc. etc. for the next 20 years. I am going to ignore it and live my life.
If new and compelling information comes to light, I reserve the right to change my mind.
6 Likes
This is not solid logic, since the vaccine does not prevent us from getting covid. Logically, if getting vaccinated you have 2 things that could cause myocarditis - the vaccine, and the subsequent covid infection - which you are still likely to get.
I think we share the idea that the risk of myocarditis post-vaccination is lower than it is pre-vaccination, and so we believe it will net out that your overall risk of myocarditis is lower with vaccination. But this is not entirely clear in the data as far as I know.
There is a ton of low-quality observational data showing better health outcomes among the vaccinated / boosted. But all of it suffers from obvious confounding. It turns out those who get vaccinated are, as a group, healthier, wealthier, and wiser than those who don’t. They have fewer car accidents, for instance. The groups are not the same.
Obviously researchers try to account for this, but we can never know whether we’ve got it right. Hence the need for periodic RCTs, which we don’t have. So the whole subject ends up in this zone of “expert opinion”. Which is often correct, but not always.
2 Likes
Quick question, are there already any trials to induce broadly neutralizing antibodies for covid?
1 Like
I got the shots, I sincerely regret it. Having said that, I am a big believer in vaccines in general.
Because I was in the Navy and later on worked for a civilan contractor overseas, I have had about every vaccine that’s available. Some even that are a little rediculus. Just yesterday my pharmacy reminded me that I was behind on my shots. I got the flu shot and Hep B & C even though there is not even a remote chance that I would get hepatitis. Some vaccines I have been required to take more than once, just because it was a requirement for my job.
In the last 50+ years, I have never once gotten the flu. I don’t even remember the last time I caught a cold. You would think because of my age, I would get the occasional cold because of the predicted lower immune system. I think rapamycin has offered additional protection.
As I said, the only vaccine I regret taking was the Pfizer Covid vaccine. I know that there are many doctors and other educated people who are forum members that are big fans of mRNA vaccines, but I truly believe they are playing with fire. The consequences of mRNA vaccines might not show up for decades.
5 Likes
With how many old people we’ve vaccinated with mRNA vaccines until now, shouldn’t we have seen a huge uptick in cancer death rates in them if there really was an unknown risk invovled? Or birth defects in (pregnant) women vaccinated between 2021 and 2024.
If something is unknowingly dangerous, we’d first detect it in animal research or at the latest a few years in human use in the most fragile amongst us. The notion that it starts affecting young to middle aged people after decades somehow but is ridiculous.
1 Like

23 NNT with 0.10% Azelastine nasal spray x3 a day at the calculated ARR.
2 Likes
There is a non-mRNA vaccine available.
2 Likes
2 Likes
No, it is not. You don’t understand one of the basic principles of cause and effect. The longer the time between cause and effect, the harder it is to detect the negative consequences.
"Delayed negative consequences, especially from pharmaceuticals and chemicals, highlight the importance of vigilant long-term monitoring and post-marketing research to uncover risks that may only emerge after years of widespread use and exposure."
Some people regard us skeptics as conspiracy theorists. We regard them as naive.
I could make this list much longer if I were to include many other chemicals, smoking, products such as Roundup weed killer, asbestos, etc.
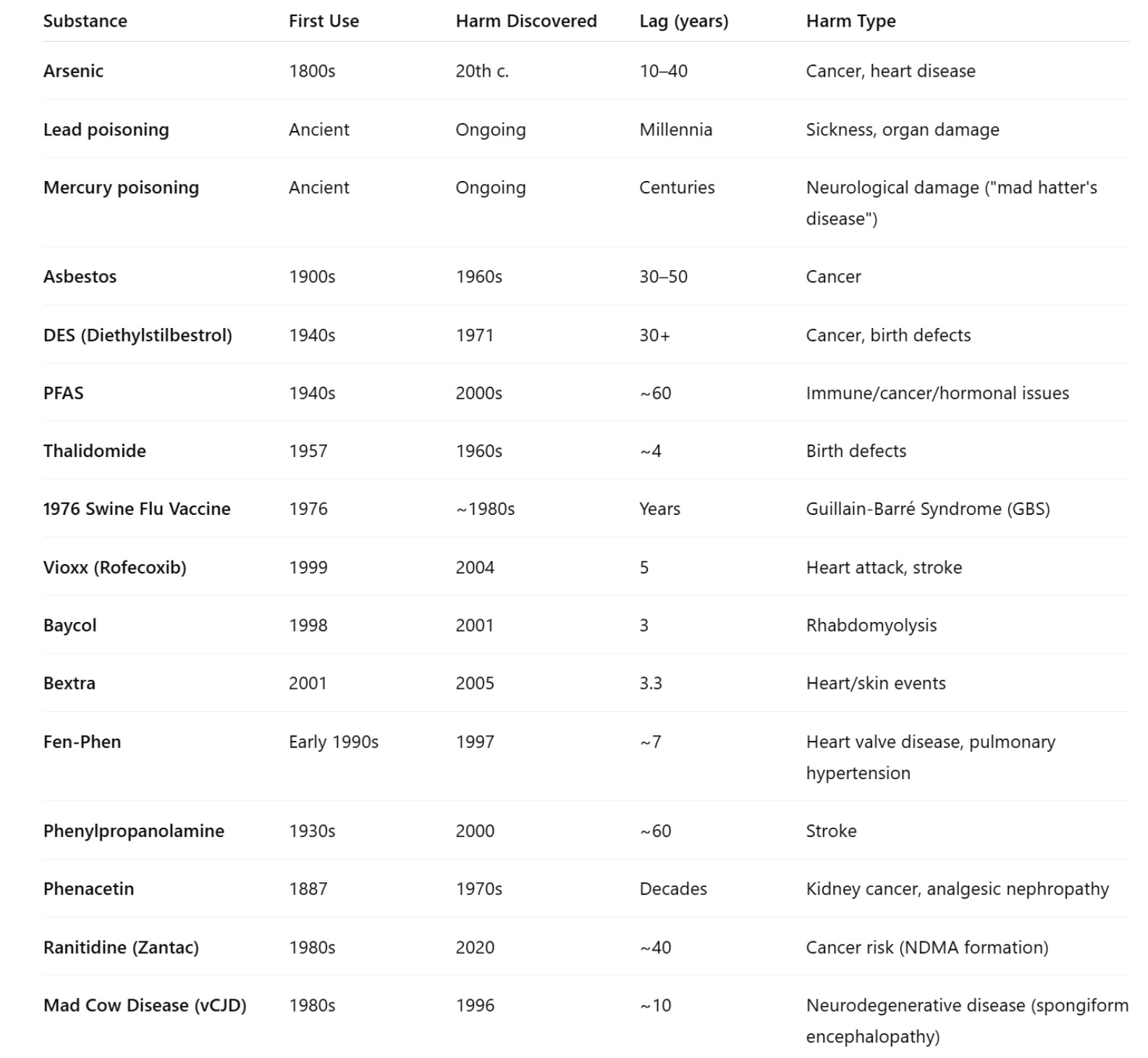
I hope for my sake as well as yours that mRNA vaccines will have no long-term consequences. But we know that is not true for the many who have already experienced them.
That, coupled with the fact that the COVID-19 vaccine was probably only 40% effective at best.
Yes, given the COVID-19 vaccine history, I will skip any further COVID jabs.
I know that immunologists are all giddy about the potential of mRNA vaccines, but then so were the scientists behind many failed drugs.
What we don’t know:
1. Potential for Autoimmune Reactions
-
Unknown: How long-term mRNA exposure in the body could potentially trigger autoimmune responses.
-
Argument: mRNA vaccines instruct cells to produce a spike protein that the immune system recognizes as foreign. In some rare cases, this could potentially trigger an autoimmune reaction, where the immune system mistakenly targets healthy tissues. Conditions like myocarditis and autoimmune diseases (e.g., lupus, rheumatoid arthritis) have been seen in rare instances following vaccination.
2. Gene Integration or Altered Gene Expression
-
Unknown: The potential for mRNA or the DNA fragments within the vaccine to integrate into the human genome.
-
Argument: While the mRNA is designed to stay in the body temporarily and degrade, there’s uncertainty about whether fragments of mRNA or reverse-transcribed DNA could integrate into the genome. If integration occurs, this could lead to unintended genetic mutations or long-term effects like cancer (via activation of oncogenes or suppression of tumor suppressor genes).
3. Unanticipated Long-Term Effects of Spike Protein
-
Unknown: How long-term production of the spike protein could affect tissues beyond its intended duration of expression.
-
Argument: The spike protein created by the mRNA could potentially accumulate in tissues, especially in organs like the heart, brain, and liver. If the spike protein persists beyond its typical clearance time, it could cause chronic inflammation, vascular damage, or neurodegenerative changes over time.
4. Unknown Effects on Reproductive Health
-
Unknown: The impact of mRNA and any associated genetic material on fertility and pregnancy in the long term.
-
Argument: While no direct links between mRNA vaccines and infertility have been conclusively proven, concerns exist regarding potential long-term impacts on male and female reproductive health. The spike protein’s interaction with reproductive tissues and whether it may have delayed effects on pregnancy or fertility remains uncertain.
5. Immune System Dysregulation
-
Unknown: How repeated exposure to mRNA vaccines over time might impact immune system function.
-
Argument: There’s concern that repeated stimulation of the immune system via mRNA vaccines might lead to immune system overactivation or dysfunction, potentially increasing the risk of chronic inflammation, immunodeficiency, or autoimmune disorders in the long term.
6. Long-Term Impact on the Microbiome
-
Unknown: Whether mRNA vaccines have any indirect effects on the human microbiome and gut health.
-
Argument: While mRNA vaccines act primarily in muscle tissue, they could have unforeseen secondary effects on the gut microbiome or other microbiota populations, which are crucial for immune regulation and overall health. Changes to the microbiome could indirectly affect the immune system and long-term health.
7. Unpredictable Long-Term Effects of DNA Fragments
-
Unknown: The fate of DNA fragments from the vaccine after mRNA is translated into the spike protein.
-
Argument: While the mRNA is designed to degrade, the possibility of DNA fragments (from the reverse transcription of mRNA) persisting in the body is a concern. If these fragments remain in cells, they might contribute to genetic changes over time, potentially affecting cellular behavior or leading to gene mutations.
8. Unforeseen Interactions with Other Vaccines and Treatments
-
Unknown: How the mRNA vaccine interacts with other vaccines, medications, or underlying conditions over the long term.
-
Argument: Long-term interactions between mRNA vaccines and other vaccines or treatments (especially in the context of polypharmacy in older populations) are not fully understood. For instance, how mRNA vaccines might interact with cancer treatments, immunosuppressants, or antiviral drugs is still under investigation.
9. Lack of Long-Term Safety Data
-
Unknown: The full scope of long-term safety and adverse effects, especially as mRNA vaccines were developed and deployed rapidly in response to the COVID-19 pandemic.
-
Argument: While short-term safety data is robust, long-term data spanning several years or decades is unavailable. This leaves open the question of whether previously undetected side effects will emerge as more people receive the vaccine over extended periods.
10. Potential for Chronic Conditions or Long-Term Illness
-
Unknown: Whether mRNA vaccines could contribute to the development of chronic conditions such as fatigue, neurological disorders, or other long-term illnesses.
-
Argument: There are concerns that mRNA vaccines could contribute to chronic health issues in a small subset of people, particularly those with underlying conditions. The possibility that mRNA vaccines could trigger long-term fatigue, brain fog, or other neurological issues, similar to post-viral syndromes like long COVID, is a potential risk that remains poorly understood.
11. Impact on Cancer Risk
-
Unknown: The possible long-term impact of mRNA vaccines on cancer development due to immune system changes or genetic alterations.
-
Argument: There is a concern, albeit speculative, that the mRNA could have an unintended effect on cell division or tumor suppression mechanisms, leading to an increased risk of cancers. This could occur if mRNA leads to gene mutations or altered immune responses that facilitate tumor growth.
Conclusion:
While mRNA vaccines have shown immense promise in preventing infectious diseases like COVID-19, there are numerous uncertainties about their long-term effects, especially concerning genetic material (both mRNA and DNA). Until more long-term data is collected, concerns about autoimmunity, gene integration, and the broader, unanticipated health effects persist. Further research and continued monitoring are essential to fully understand the long-term safety profile of mRNA vaccines.
As I have undoubtedly taken more vaccines other than the most extensive world travelers, again I reiterate that I am not against vaccines.
So we have once again beaten this into the ground. Covid vaccines, lovers and haters. At this late date, it is unlikely to change anyone’s mind.
3 Likes
So how do you make of the fact that you’re still going to be exposed to the COVID virus – of which the vaccine is only trying to emulate the spike protein? And without natural antibodies to the new variants, after all – the virus is mutating?
The spike in the vaccine is carefully engineered.
Ask an AI about the amount of binding the pre-fusion stabilized spike protein in COVID vaccines has to the ACE2 receptor compared with the ones in the COVID virus itself.
Mine suggests it’s negligible – so the COVID vaccine spike protein might be inactive and neutral.
You use some cells to produce the spike proteins with mRNA vaccines, but that’s mostly in the shoulder area and not a lot.
3 Likes
2.1. Coronavirus Spike Glycoprotein as Vaccine Target
Coronaviruses are a family of (+) ssRNA enveloped viruses that encode four structural proteins.
Among these structural proteins, S is a key target of neutralizing antibodies and therefore an
important antigen for vaccine development. The spike protein is an important vaccine target or
antigen, as it mediates first the specific binding of the virus to the angiotensin-converting
enzyme 2 (ACE2) host cell receptor and then the fusion of the viral envelope with a host cell
membrane. By these actions, the virus can enter human cells where it replicates, often causing
illness, and potentially spreading to other people. Data available from other coronaviruses such
as SARS and MERS had established that antibodies to the S protein can block the binding of the
virus to cells and prevent viral infection.10,11 The Pfizer-BioNTech COVID-19 Vaccine encodes
a membrane-anchored, full-length S protein with two point mutations to proline within the
central helix domain to lock S protein in an antigenically preferred prefusion conformation.12,132.2. RNA-Lipid Nanoparticle Formulation
The Pfizer-BioNTech COVID-19 Vaccine is based on an RNA-LNP platform of nucleoside-
modified RNA, which has blunted innate immune sensor activating capacity and thus augmented
antigen expression. Pfizer-BioNTech COVID-19 Vaccine, BNT162b2 (30 μg), encodes a P2
mutant S (P2 S) and is formulated in LNPs. Encapsulation into LNPs enables transfection of the
RNA into host cells after intramuscular (IM) injection. These LNPs are composed of four
different lipids in a defined ratio. During mixing of the RNA and the dissolved lipids, the lipids
form the nanoparticles encapsulating the RNA. After injection, the LNPs are taken up by the
cells, and the RNA is released into the cytosol. In the cytosol, the RNA is translated to the
encoded viral protein. The P2 S antigen incorporates into cellular membranes and induces an
adaptive immune response. As S is the antigen that recognizes ACE2 and enables infection of the host cells, it is a key target of virus neutralizing antibodies. Furthermore, as RNA-expressed S is fragmented intracellularly, the resulting peptides can be presented at the cell surface, triggering a specific T cell-mediated immune response with activity against the virus.
https://www.fda.gov/media/144246/download
Update accordingly how so many people believe false things and how many are influenced by them. Since there’s so much anti-covid vaccine sentiment on false grounds it might make you believe there is something, but there seems to be not. That’s quite a staggering finding about a lot of people.
And then there are those heavily influenced by Big Pharma propaganda.
- Potential for Autoimmune Reactions
Unknown: How long-term mRNA exposure in the body could potentially trigger autoimmune responses.
Argument: mRNA vaccines instruct cells to produce a spike protein that the immune system recognizes as foreign. In some rare cases, this could potentially trigger an autoimmune reaction, where the immune system mistakenly targets healthy tissues. Conditions like myocarditis and autoimmune diseases (e.g., lupus, rheumatoid arthritis) have been seen in rare instances following vaccination.
If virus spread requires host mobility & social contact → selection often nudges toward lower virulence (but not guaranteed).
That certainly seems to be the case with Covid. As reported by @DeStrider who seems to get it every year, though with mild symptoms. Maybe the vaccine is reducing his symptoms or maybe in his case it prevents nothing.
2 Likes
Yes the prefusion stabilized spike protein creates an immune response, that’s the point. It doesn’t seem to do any harm to tissues as the ACE2 binding is lower than the spike protein on the virus according to AI. This doesn’t exclude the fact of exposure to unrecognized SARS-COV-2 spike proteins by antibodies without artificially produced antibodies to new variants.
So avoiding the vaccine booster means:
- No antibodies to new variants of SARS-COV-2, that means flooding the body with SARS-COV-2 that mass produce new viruses exponentially with spike proteins with higher binding to ACE2 obviously, as that’s how the virus get into cells.
- Body is flooded with SARS-COV-2 spike proteins that bind to ACE2 indiscriminately.
- Diseases from the virus AND the immune response.
While meanwhile you reduce risk from the virus with artificially produced antibodies.
You don’t avoid the immune response with or without vaccine.
2 Likes
The vaccine and booster, in my case, each provided a year’s protection. My whole family got COVID, and I did not, as I was the first one to be vaccinated in my family at the start of the pandemic. After a year, I started getting COVID again. The disease also provided a year’s protection. So now, like clockwork, if I don’t get vaccinated, I get COVID in the early Spring. I’ve had it for the past 3 years.
My sister-in-law got COVID, and it destroyed her kidneys, which no longer function. Now she has to do 6 hours of dialysis at the hospital 3X a week and is expected not to make it to her 60s. (She hasn’t been able to get a transplant.)
COVID, at least at the beginning, was incredibly dangerous and harmful. It was like playing Russian roulette. You might be fine, or you might die or have something heinous happen to you, like losing your kidneys.
I still believe that getting the vaccine is better than getting the disease, so, based on my history, I’ll probably start the vaccine again, as I don’t want any more infections. I tend to believe that viruses like to hide out in your body and wait until you are weak to strike you down.
4 Likes