Currently I am only taking rapamycin, but am considering both acarbose and a SGLT-2 inhibitor, specifically Jardiance. I am curious if anyone has tried this combination or a similar one. If so, did you notice any effects, good or bad? Are you still on this protocol? Any advice? Anyone think this trio is not a good idea?
3 Likes
i am 70 currently taking all three, daily 10 mg Jardiance, acarbose 25 mg twice on two meal time every day, 4 mg rapamune once a week, no adverse effect, lost ten pound and and able to maintain weight at 150 lb.
7 Likes
Yes - I use all three. I started with canagliflozin then moved over to empagliflozin / jardiance. I’ve written about my experience here: Canagliflozin for Anti-aging - One Month and 4 Month Updates
Now I’m on empagliflozin and acarbose (50mg or 100mg) (PRN, as needed, when I take breaks from the SGLT2 inhibitor. Acarbose is much better with a diet that avoids wheat (for me, from a side effects perspective). More details here: Acarbose - Another Top Anti-Aging Drug
6 Likes
Today on twitter: (ACA = acarbose, Cana= Canagliflozin
4 Likes
Currently, I am taking 4 medications to control blood glucose. High glucose causes inflammation of arteries feeding the kidneys, heart, brain and all other organs throughout the body. Inflammation= plaque buildup and “hot plaque” which causes embolism. Controlling inflammation and arterial health is top priority for me. I currently take Rapa, Metformin, Jardiance, and Acarbose. Use Beano to control gas caused by Acarbose. 76 yo, 75 kg, 180 cm
6 Likes
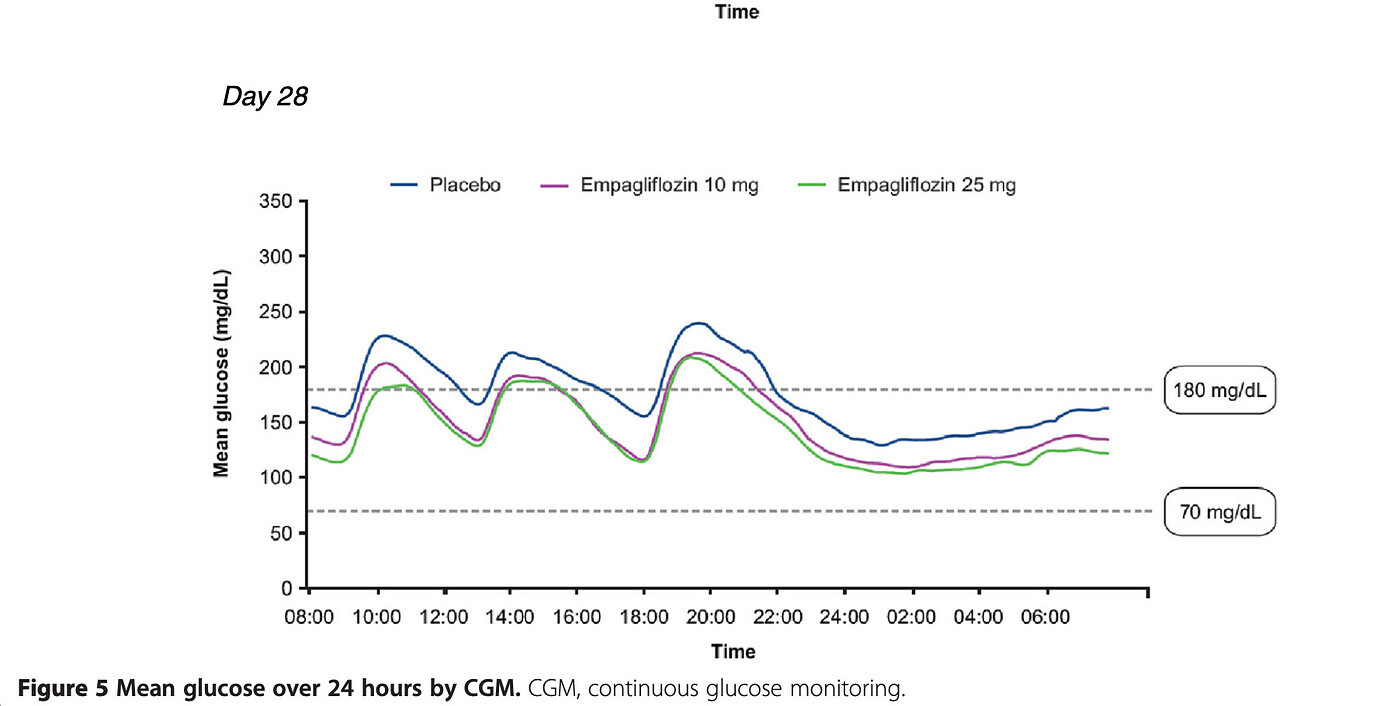
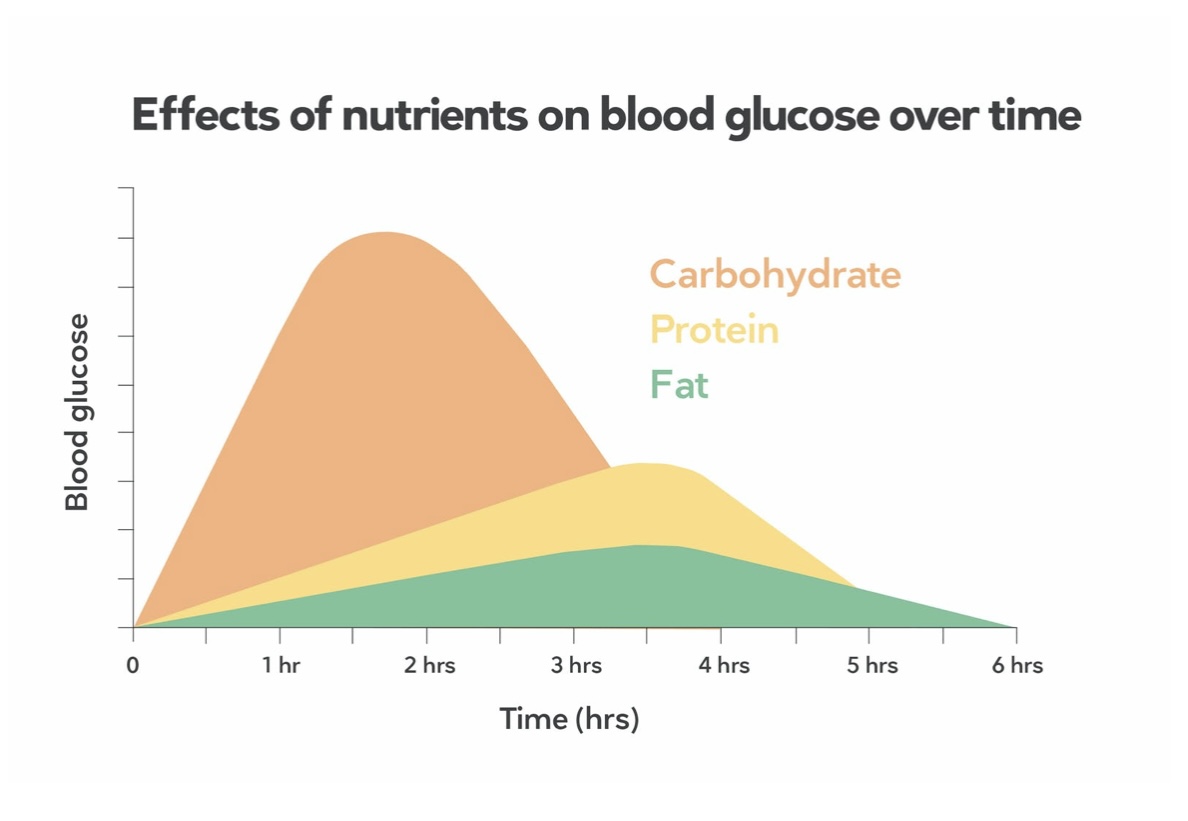
I guess Agingdoc1 didn’t look up the actual human trial data and overlaid to a true keto diet? The blunting is actually a complete shift shifting down. So potentially an unsafe bias for true low glucose ketogenic diets? (at least at “therapeutic” doses). It would be interesting, since keto is lower starting glucose and far lower post prandial spike. Only a trial would elucidate.
CANA
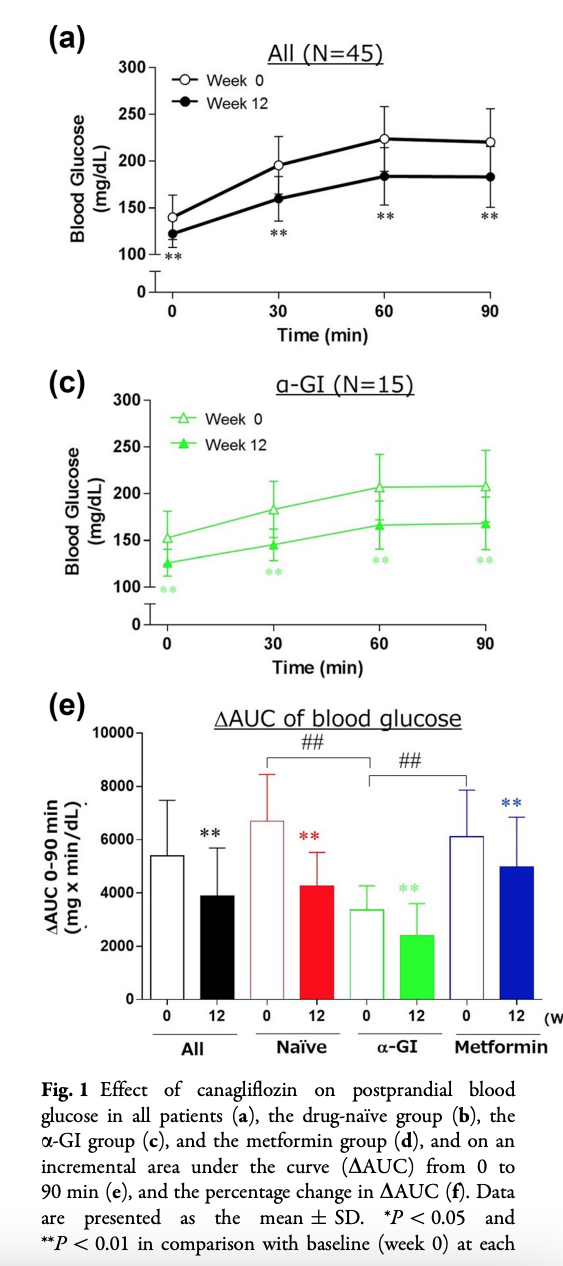
EMPA
4 Likes
Thank you RapAdmin and MAC for your many informative posts. MAC, I think your point is that, if one is on a true (strict) keto diet, then supplementing with acarbose and an SGLT-2 inhibitor might well lower blood glucose too much; am I correct?
3 Likes
Yes, that’s my theory. Since these meds shift the entire curve down, not just blunt the spike, there is significant hypoglycaemic risk, especially if you adhere to a strict keto, low blood glucose diet.
When I played with a freestyle libre glucose monitoring device for a few weeks, post prandial glucose rose very minimally. I had a glass of orange juice once just for fun, it skyrocketed.
2 Likes
I agree with Mac on this - if you’re already very low carb, you are not getting much in the way of blood glucose spikes anyway, so its probably not worth the time, effort, money and risk to add these blood glucose control medications, and it might lower your blood glucose too much and be harmful.
I don’t take acarbose and empagliflozin at the same time because that seems redundant as we are trying to blunt glucose spikes, and that is well achieved (in my experience) by either one alone. I may try them together in the future though, and with close blood glucose monitoring to make sure I’m not hypoglycemic, just to see how it modifies things.
For me, eating mostly a veggie and fish diet, its been good though. I avoid simple carbs / breads / sugars, etc. and my blood sugar is typically in the range of 80 to 110, which is exactly my target range.
2 Likes
When you do take either acarbose or empagliflozin you take it with the first bite of a meal that contains some carbs, correct?
2 Likes
No - not exactly correct.
For Acarbose - that is the case - I take the acarbose (25mg, 50mg or 100mg, etc.) with the first bite of the meal.
But with the SGLT2 inhibitors I take it 1 hour or more before the meal. The SGLT2 inhibitors take longer to get into the blood system and become effective.
Here is the blood curve for canagliflozin:
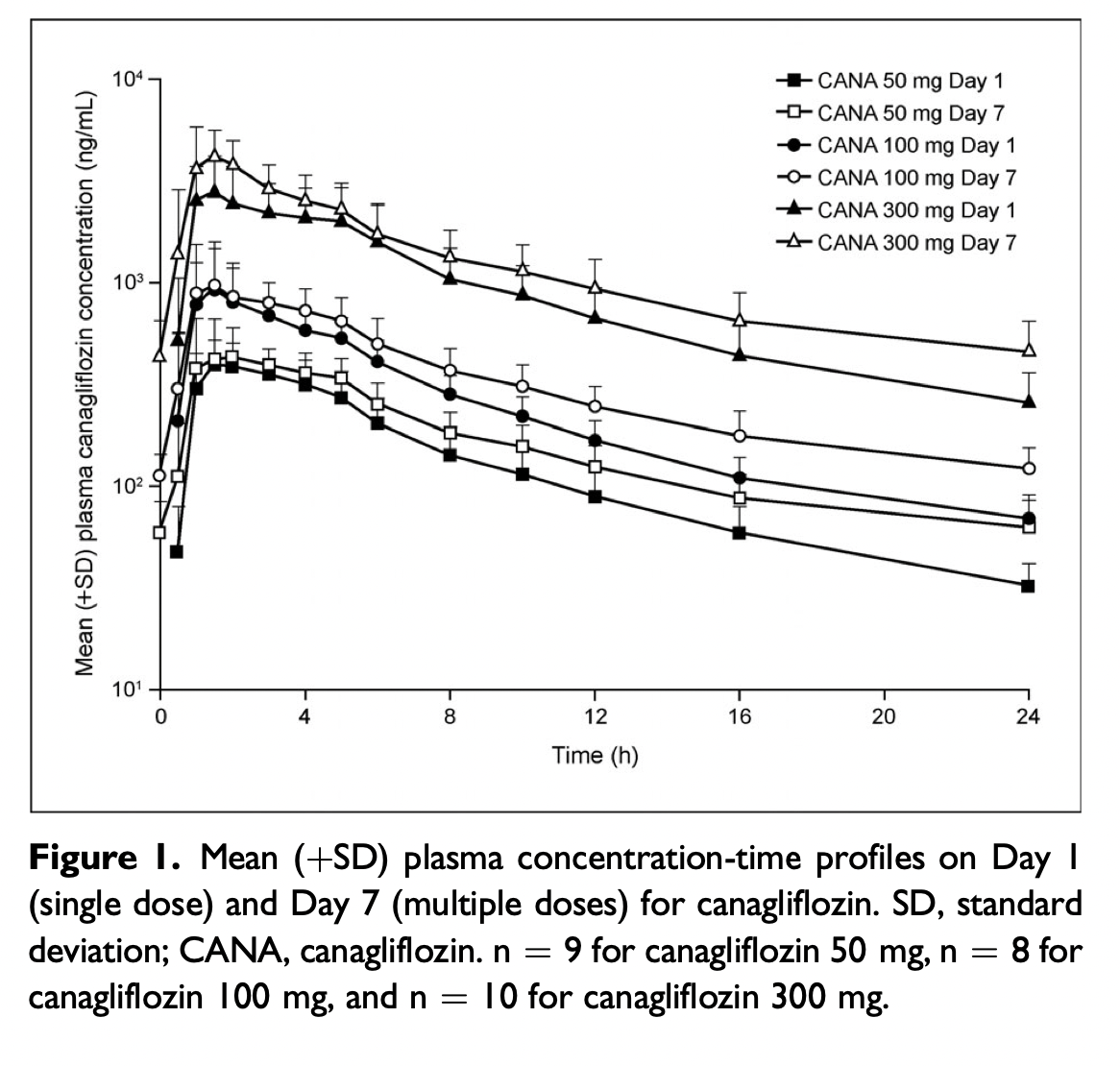
Source: https://accp1.onlinelibrary.wiley.com/doi/pdf/10.1002/jcph.88
Here is the full insert for Canagliflozin - good to read and review prior to taking the drug:
4 Likes
A good talk about Canagliflozin and using both Canagliflozin and Acarbose:

6 Likes
Any thoughts on these studies relating to Acarbose and SGLT-2 Inhibitors and muscle mass?
2 Likes
Pollux, I wanted to thank you for sharing your regime. It is so very helpful for those of us starting this journey. I’m 62 and have been on the rapa since January and after delving into the pubmed research, am ready to add the other meds.
With gratitude Adrienne
2 Likes
This is fantastic info. I have found that Farxinga does not have a large enough effect on lowering glucose A1C. I am adding acarbose as shown in the video to get a big enough effect, and to avoid metformin. I do not like the effect metformin has on my lactate production when I exercise.
2 Likes
RE: Other anti aging meds.
Hmm…… Sadly does not appear as efficacious for women. “Ultimately, the resolution of these sex differences comes down to experimentation. “
“A promising and novel approach for identifying anti-aging therapeutics has been the repurposing of clinically approved and readily available drugs in mice. Canagliflozin, a clinically approved safe, and effective drug for type 2 diabetic patients, was recently shown to robustly retard age-related lesions in male mice but less so in female mice. While this type of sex disparity is often seen in the field of aging, it does represent a dilemma of not knowing the cause or how translationally relevant the sex differences would be in older humans treated with Canagliflozin.
Thoughtful and mechanistic investigations are needed to understand why these differences are present and whether they can be eliminated by new drugs.”
http://www.antpublisher.com/index.php/APT/article/download/530/632
1 Like
This is interesting - epidemiological, but plausible.
Strength is important in aging but it seems to me if you keep exercising you will be fine.
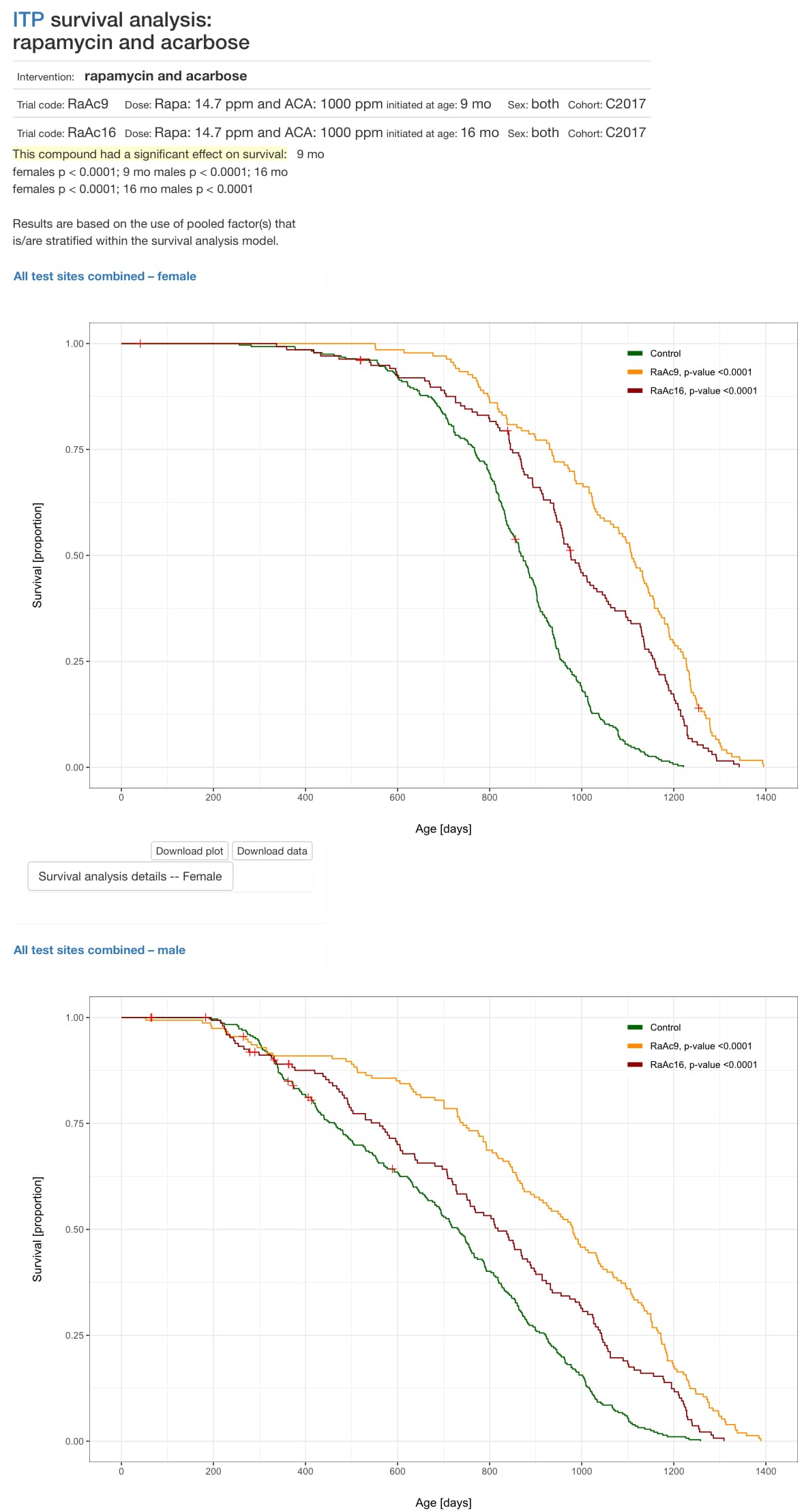
Rapamycin + Acarbose is by far the most promising intervention, with the largest ITP effect.
5 Likes
So my understanding is you do not take Acarbose and Jardiance at the same time due to the risk of low blood sugar. The only reason you use them both is so you can take breaks from Jardiance or from Acarbose.
What is the logic of taking breaks from either one? Which one is it you use most of the time? How long are your breaks?
Thanks RapAdmin.
1 Like
My thinking has changed a little on this over the past year. I need to do more testing with my CGM and acarbose and SGLT2 inhibitor, to see how my blood sugar levels fluctuate with just one or both of them. Acarbose may have benefits outside of the blood glucose lowering, as might the SGLT2 inhibitors… that is what the current research seems to suggest now.
The logic of breaks (only from SGLT2 inhibitors) is that you are peeing out a lot of sugar with them, and with the increase in sugar (my pharmacist friend tells me) … bacteria love sugar, and so the more sugar in your urine, the more risk of UTIs. I’ve never had a UTI, and as male I think we get fewer anyway, but taking periodic breaks are going to help lower bacteria levels in your Urinary tract, at least thats part of my thinking. The other part of my rationale is that as a healthy person taking these drugs it seems reasonable to take breaks periodically just to help minimize risks associated with poly pharmacy (numerous drugs at the same time).
But its all a SWAG (scientific, wild ass guess). I have no data to back any of this up yet. I will continue to do blood glucose and blood testing to track my results over time. Nothing major to report yet.
2 Likes
@RapAdmin Dont forget about methylene blue. It accumulates in the bladder and is an antimicrobial. And it has nootropic benefits (helping brain and other mitochondria to function better).
Stem talk podcast with Dr. Francisco Gonzalez-Lima, a behavioral neuroscientist at The University of Texas at Austin.
4 Likes