The guy is kooky, as I said, and some of the references are no good either, but there are so many links that it is worth looking into, because more established sources never mention many of those studies and deny such results exist.
About nocebo, again: It is not applicable to usual patients, because they do not expect any such particular side effects.
Your study here first gave the patients side effects from the statins, and then tested with placebo, which is very different.
The average patient researches medication for at least a few minutes on the internet. Especially statins because over 1/5 of the population is on them.
Your study here first gave the patients side effects from the statins, and then tested with placebo, which is very different.
The study I posted had three groups: control, placebo and statin group. The placebo and statin groups both had myalga symptoms (slightly but not statistical signficantly higher in the statin group).
All those old people getting statins from the doc can suddenly go beyond the first few google results, reaching information that does not downplay the side effects??? Why this then only with statins and other strongly shilled drugs such as covid gene therapies (“vax”)?
And about that study you refer to: It was done in order to give support to this nocebo charge that the statin shills dismiss so many suffering patients with. So they made the participants aware of those side effects on top of the on-off design of the dosing. They know what they are doing! Science is a lucrative game, we know how to play it. I do.
“study I posted had three groups: control, placebo and statin group.”
No! From the paper:
“Participants received 12 1-month medication bottles, 4 containing atorvastatin 20 mg, 4 placebo, and 4 empty.”
The statins gave them the side effects, and thus deepened their expectation. The researchers wanted to find nocebo, so they did everything so they would find nocebo. It is sophisticated fraud.
The first results on google and youtube are from antivaxx quacks that say that statins and the covid vaccine will give everyone and their puppies a trillion side effects.
So they made the participants aware of those side effects on top of the on-off design of the dosing.
But if the nocebo effect wasn’t real, then the placebo group should’ve had the same myalga score as the control group, right?
“Participants received 12 1-month medication bottles, 4 containing atorvastatin 20 mg, 4 placebo, and 4 empty.”
So one statin group, one placebo group and one control group.
The statins gave them the side effects, and thus deepened their expectation.
Again, both the statin and the placebo group had side effects.
I kind of don’t understand what you are arguing here for.
Are you claiming that the nocebo effect isn’t real and therefore all side effects experienced on statins must originate from the medication itself? In that case, there are multiple studies proving that even the placebo group experiences side effects at nearly the same rate as the statin treatment group.
Or are you claiming that the nocebo effect is real but because none of the millions of patients ever read up on possible side effects or get informed of them by their doctors, they don’t experience the nocebo effect and therefore any side effect must exclusively come from the medication itself? That also doesn’t make any sense because even boomers and what remains of the silent generation use the internet nowadays. Even your 99 year old grandmother who doesn’t even know how the tv works would at least get come consultation by her doctor regarding her medication.
First of all, I’m asking you for evidence to support your statement that statin manufacturers organise a conspiracy to secretly pre-select trial participants who won’t have side effects.
Second, large meta-analyses of good-quality trials have shown that the true incidence of muscle pain from statins is less than 10%. You absolutely see muscle pains in some patients taking statins, but when they’re blinded to the treatment, there’s also increased muscle pains in the placebo groups. The effect also isn’t “downplayed”. Every doctor prescribing a statin tells their patient to watch out for it, which most likely increases the % of patients who notice it.
Third, those studies (to “downplay the side effects” in your words) are done precisely to address the noise of multiple people complaining that they DO have side effects. It’s not shilling for anything. It’s actually trying to address the question of whether these effects are real. Drugs have been taken off the market when those side effects turn out to be real.
Fourth, the original, major point is that side effects are not the reason why such a high % of people discontinue taking statins. It’s because you don’t have a tangible observable benefit like you do with many drugs.
Lastly, it’s ironic I guess that you’re talking about qualification, education levels and brainwashing and then followed it up by saying "covid gene therapies (“vax”). Kinda tells us everything we need to know.
yes, around these places, if people cannot grasp or deny the difference between a proper vaccine and those mRNA spike protein clot shots, that indeed tells all we need to know!
The only people getting clots are the antivaxxer cholesterol deniers. And deservedly so.
I could point out how stroke and MI (death) rates have continued to decline post 2021 but of course that would all just be some jewish conspiracy by the Big Pharma deep state.
what’s wrong with rosuvastatin? I have been taking 10mg with 10mg ezetimibe for many, many years and my lipids are well below the normal ok ranges. no issues with side effects.
That’s an “umbrella creates rain” scenario. They probably nag because they know people don’t take them. The general public is kinda dumb and lazy, and isn’t very proactive, if we’re honest. That’s a far more likely explanation than there are serious adverse events which remain hidden in huge clinical trials.
You are the norm. That drug combination works fantastically for the vast majority of people who take it, and it’s adding years to your life by delaying heart attacks. Easy.
Yes - non-adherence to medication regimens are a huge problem in medical treatment.
From Google Gemini:
Medication nonadherence, or failure to take prescribed medications as directed, is a common issue, with studies estimating that up to 50% of patients do not take their medication as prescribed. Various factors contribute to nonadherence, including cost, fear of side effects, and lack of understanding about the medication or its purpose.
Specific rates and factors:
Cost-related nonadherence:
A study found that 29% of older adults did not take their medications as prescribed at some point in the past, with nearly one in four Americans who take prescription medications saying it’s difficult to afford them.
Unfilled prescriptions:
Some studies have shown that 28% to 31% of new prescriptions for conditions like diabetes, high blood pressure, or high cholesterol go unfilled.
Reasons for nonadherence:
Cost: High medication costs can lead patients to delay filling prescriptions, take less medication than prescribed, or skip doses altogether.
Fear of side effects: Patients may be concerned about the potential side effects of the medication.
Lack of understanding: Patients may not understand the need for the medication, how it works, or the duration of treatment.
Specific populations:
Seniors: Failure to adhere to medication instructions is common among seniors, with some reports indicating that as many as 55% are noncompliant.
Patients with chronic diseases: Nonadherence is particularly prevalent among patients with chronic conditions like diabetes and hypertension.
Impact of medication type:
Blood pressure medications, cholesterol medications, and diabetes medications may have lower adherence rates, possibly due to the asymptomatic nature of these conditions.
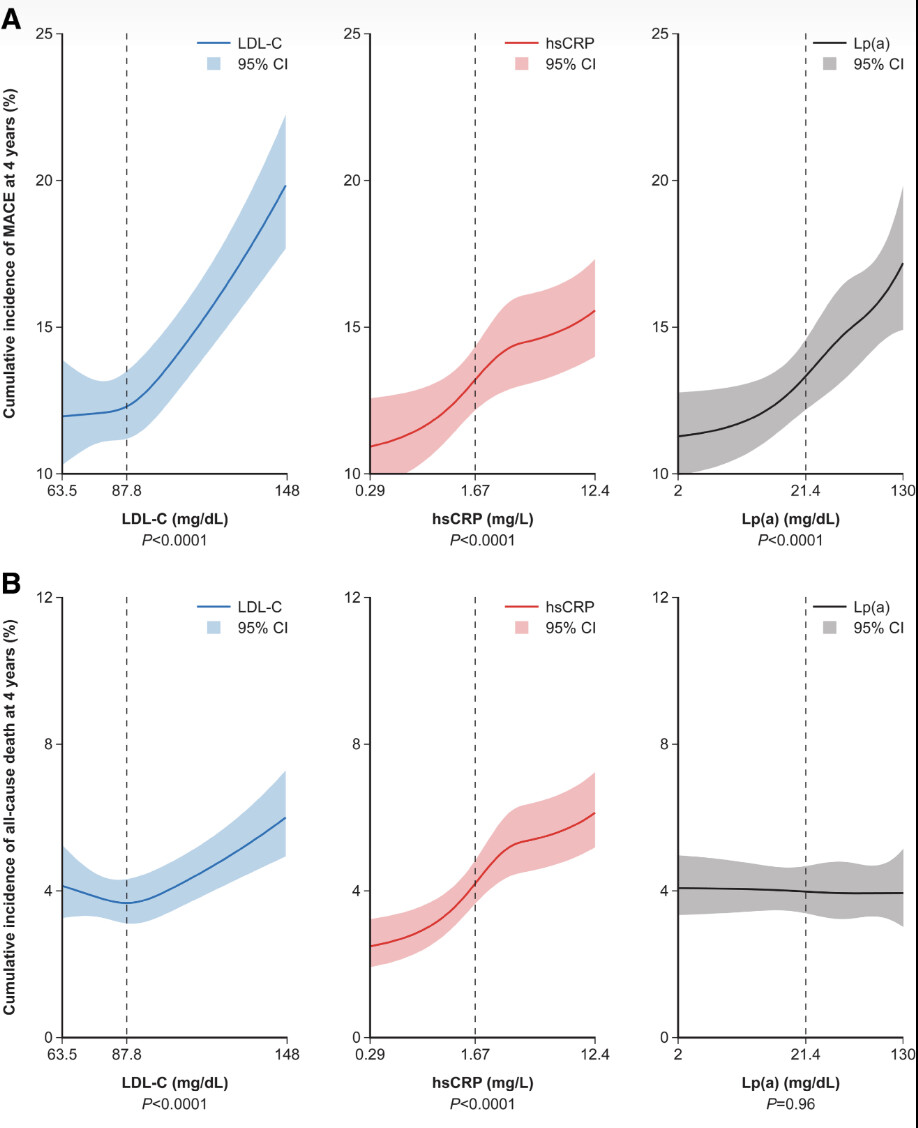
Our analysis (Figure) also suggests that the relationship of LDL-C to MACE tends to flatten below ≈90 mg/dL, the range encompassing most patients in the triglyceride-lowering trials, although the wide CIs at the lower range of LDL-C do not exclude a monotonic relationship across the full LDL-C range. The canonical view that “lower LDL-C is better” without limit may be in part confounded because measured LDL-C includes cholesterol contained in lipoprotein(a); therefore, patients with low LDL-C are more likely to have low lipoprotein(a). In the current analysis, the LDL-C relationships to events were adjusted for lipoprotein(a).
It doesn’t change my treatment decision differently, the randomized trial itself or others like it informs me what treating LDL-C lower than that does, it improves MACE and in other studies (post-hoc) show a decrease in plaque progression and maybe even regression. I think that post-hoc study on Praluent showed regression depending on achieved LDL-C as well. The treatment lowers at least Lp(a) as well, though.
Post-hoc statin studies show reduction in MACE depending on even lower achieved LDL-C levels, and as we know they don’t reduce Lp(a).
Might that reduction go away once you control for CRP? I don’t think we know this. Maybe it’s confounded by hsCRP or Lp(a). But I still think apoB/LDL-C has a linear reduction on MACE independently even below the 5th percentile.
This study suggests is identical despite different effects on other risk markers (the drugs that is).
The clinical benefit per millimoles per liter reduction in LDL-C was virtually identical for statins, ezetimibe, PCSK9 inhibition, and CETP inhibition, despite these drugs having different effects on other risk markers such as high-density lipoprotein cholesterol, lipoprotein(a), and high-sensitivity C-reactive protein. This observation reinforces the notion that the reduction in LDL-C (or more broadly, atherogenic apolipoprotein B–containing particles) is the primary driver of clinical benefit.
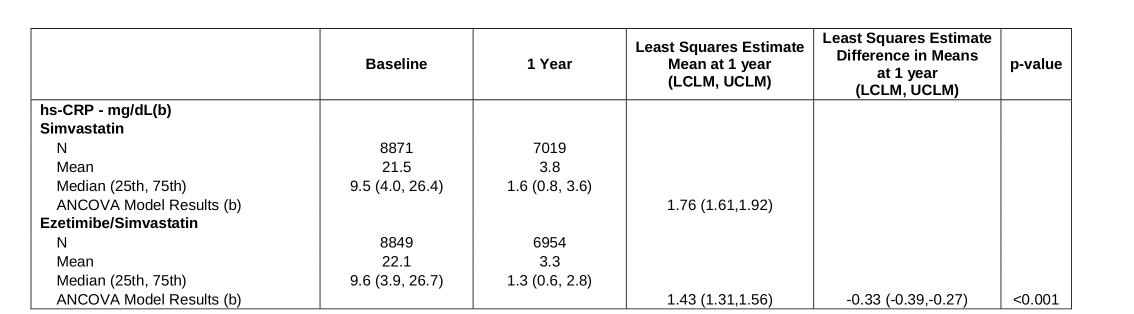
hsCRP was different at 1 year by 0.33 mg/dl in ezetimibe trial, but decreasing below 70 mg/dl for LDL-C to 53 mg/dl, is that hsCRP clinically relevant enough to confound the result?:
The median time-weighted average LDL cholesterol level during the study was 53.7 mg per deciliter (1.4 mmol per liter) in the simvastatin–ezetimibe group, as compared with 69.5 mg per deciliter (1.8 mmol per liter) in the simvastatin-monotherapy group (P<0.001). The Kaplan–Meier event rate for the primary end point at 7 years was 32.7% in the simvastatin–ezetimibe group, as compared with 34.7% in the simvastatin-monotherapy group (absolute risk difference, 2.0 percentage points; hazard ratio, 0.936; 95% confidence interval, 0.89 to 0.99; P=0.016).
@amuser you have a high CAC and had a CCTA that gave you a lot of great info, so I thought to come back to ask some questions based on what I just learned.
My brother’s cardiologist just told him a CCTA is not useful for those with high CAC scores because it can’t see through the hard plaque. Google seemed to confirm this, but I remembered your results, so is this a case of ‘it depends’?
Also, does anyone know what the CCTA shows vs a nuclear stress test and echo?
This same cardiologist suggested that instead of the CCTA. I did look it up, but why one would choose one over the other is not clear to me. Thank you
While we’re waiting for the expert, my take: The thinking is: If you have no symptoms, and a stress test shows no aberrant cardiac behavior under load, then regardless of your cac score, there’s no reason to be digging further, which involves both radiation risk and money. Nobody is going to do anything invasive if you’re that well off. Nor would it change lipid reduction strategy. If you had chest pain, might be a different story.
I have an irrational fondness for data, so pursued knowledge for the sake of knowledge. The ccta/cleerly did show that I have none of the worst kind of plaque, so that was reassuring. (But should it be? idk)
Not sure what this is about. Cleerly categorizes plaque type. CCTA doesn’t.