Vascular disease is multifaceted, but the low hanging fruit are:
Blood pressure, Insulin Sensitivity and Lipid optimization.
So minimally increasing LDL while lowering blood pressure and increasing insulin sensitivity, like occurs with the SGLT2-i on balance gives benefit. Also, I’d guess most individuals on one of these drugs is managing/optimizing their lipids anyway.
Here’s what Vera-Health.ai says on SGLT2-i and insulin sensitivity and BP.
SGLT2 inhibitors, primarily used for managing type 2 diabetes mellitus (T2DM), have been shown to both lower blood pressure and increase insulin sensitivity, offering benefits beyond glucose control.
Blood Pressure Lowering: SGLT2 inhibitors have a significant blood pressure-lowering effect, which is dose-independent and comparable to low-dose hydrochlorothiazide 2. This effect is primarily due to natriuresis and osmotic diuresis, which reduce blood volume and subsequently lower blood pressure 9. Additionally, these drugs improve vascular function by reducing oxidative stress and inflammation, further contributing to their blood pressure-lowering effects 4.
Insulin Sensitivity: SGLT2 inhibitors have shown potential in improving insulin sensitivity. For instance, empagliflozin has been demonstrated to improve hypothalamic insulin sensitivity in patients with prediabetes, suggesting a potential reversal of brain insulin resistance 1. The mechanism involves reducing glucose reabsorption in the kidneys, leading to glucosuria and a decrease in blood glucose levels 1. This reduction in glucose levels can improve insulin sensitivity by decreasing the need for insulin secretion and improving β-cell function. Furthermore, SGLT2 inhibitors promote weight loss and modulate adipocyte function, which also enhances insulin sensitivity 1.
In summary, SGLT2 inhibitors effectively lower blood pressure through mechanisms involving natriuresis and vascular improvements, while also showing potential to enhance insulin sensitivity by modulating glucose levels and adipocyte function. These effects make SGLT2 inhibitors a valuable therapeutic option for managing T2DM and its associated comorbidities.
Thanks. Yeah, one Chinese paper. I would be much happier if there are more papers confirming this result from different unis in more countries. Would be fantastic if true.
Follow up here, in June for Eric Topol - top cardiologist and one of the most cited physicians on the planet.
Don’t think that one trial result should lead to that conclusion in @DeStrider s post.
There are 6 other generally large trials showing results in the right direction…
(My inflammation is always super low (eg hs-CRP below or at the lowest bound) so I’m not going to read up more on this at this point, but wanted to share a more holistic and I believe actually view of potential here.)
The Clinical Trials
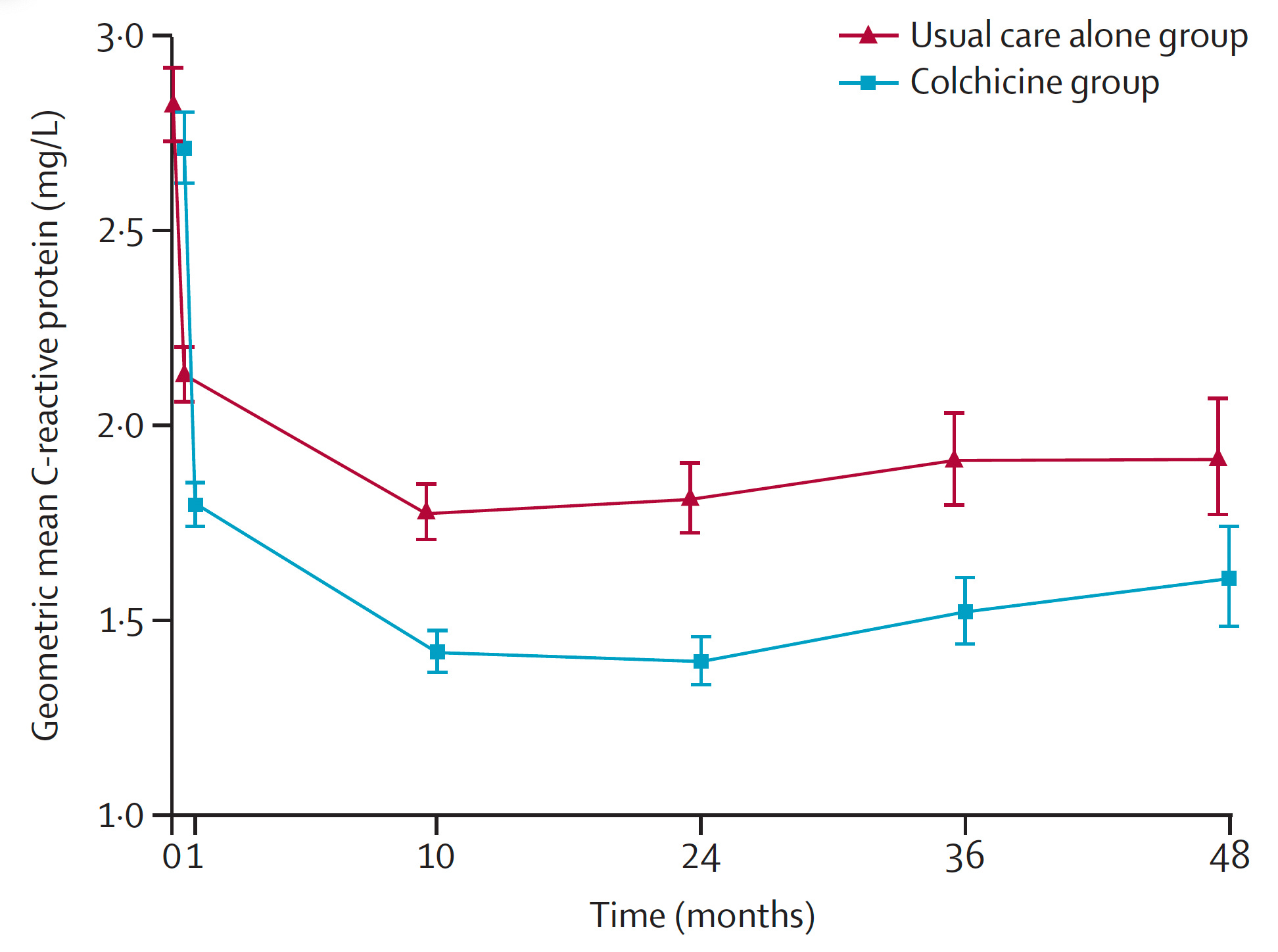
Yesterday a new randomized trial of colchicine, a potent anti-inflammatory agent, to prevent events after stroke, was published in The Lancet.Over 3,100 patients with a non-severe, non-embolic stroke or TIA were randomly assigned to 0.5 mg colchicine per day plus usual care vs usual care only. The primary endpoint was the composite of heart attack, stroke, cardiac arrest, or hospitalization for unstable angina.
In the colchicine group, the event rate by intention-to-treat was 9.8% vs 11.7% in controls, a 16% reduction that was not statistically significant (upper bound 95% confidence interval 1.05). Colchicine led to a significant reduction of high sensitivity C-reactive protein (hs-CRP) at all time points assessed (Figure below). By a pre-specified on-treatment analysis, the primary endpoint was reduced from 11.7% to 8.0%, a 20% reduction, which was statically significant.
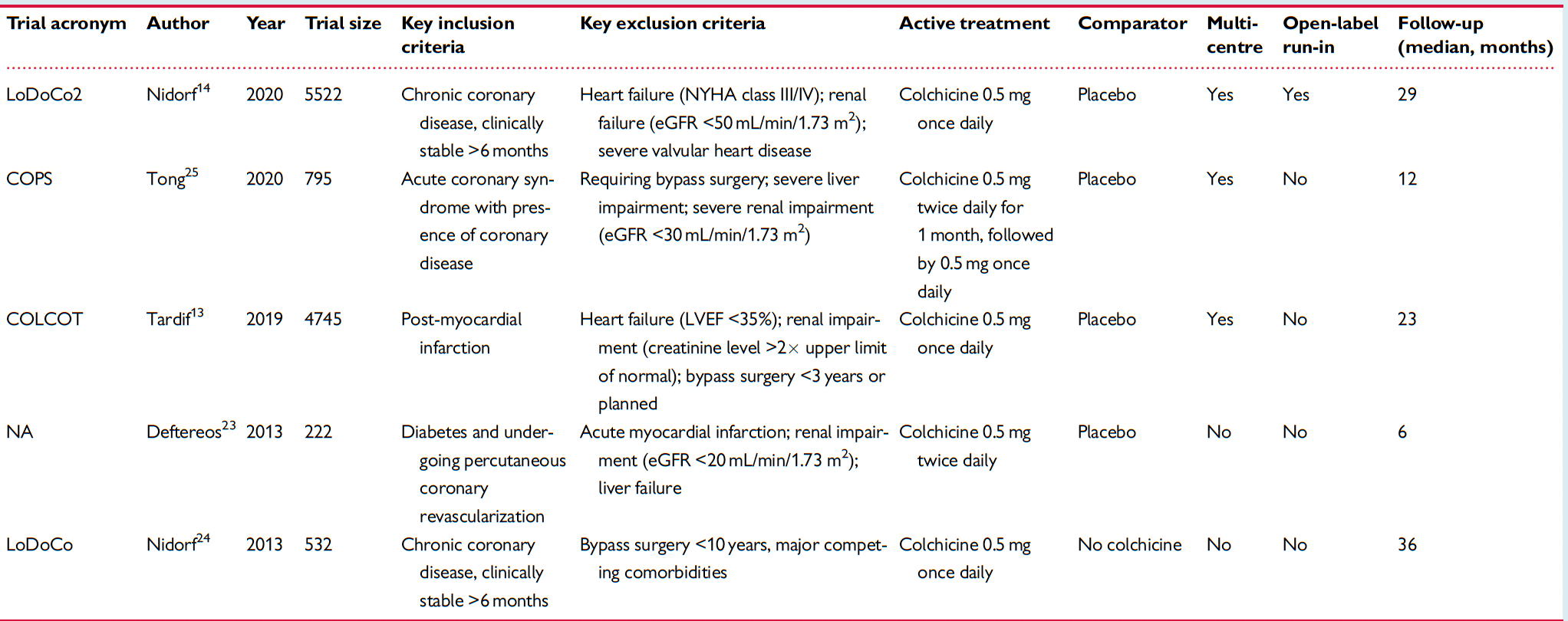
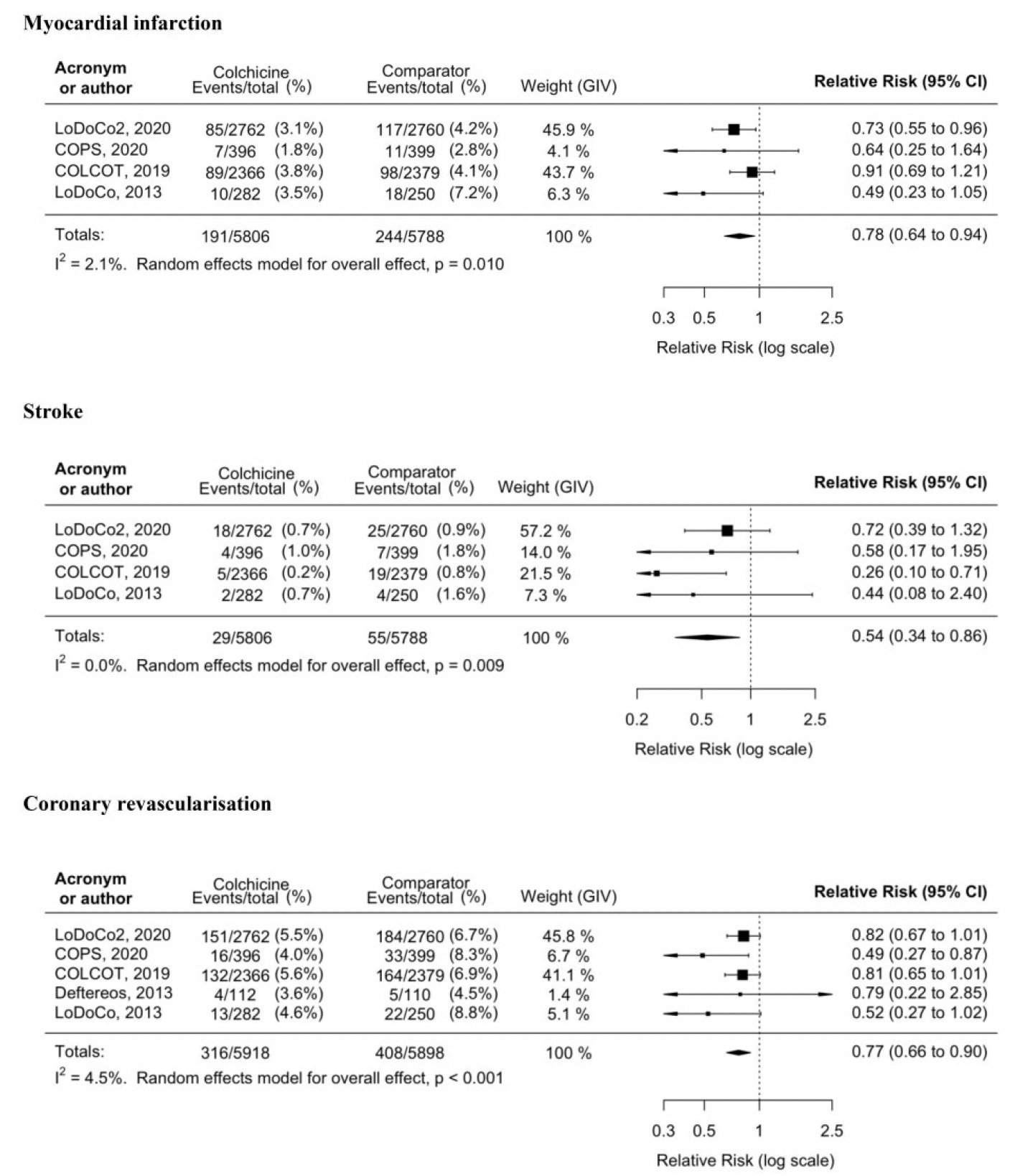
The new colchicine trial comes after 5 preceding ones that were subject to a meta- analysis. To summarize the 5 trials, the Table below shows 2 were large, each about 5,000 participants, one in chronic coronary artery disease and the other after heart attack, both with about 2-year follow-up.
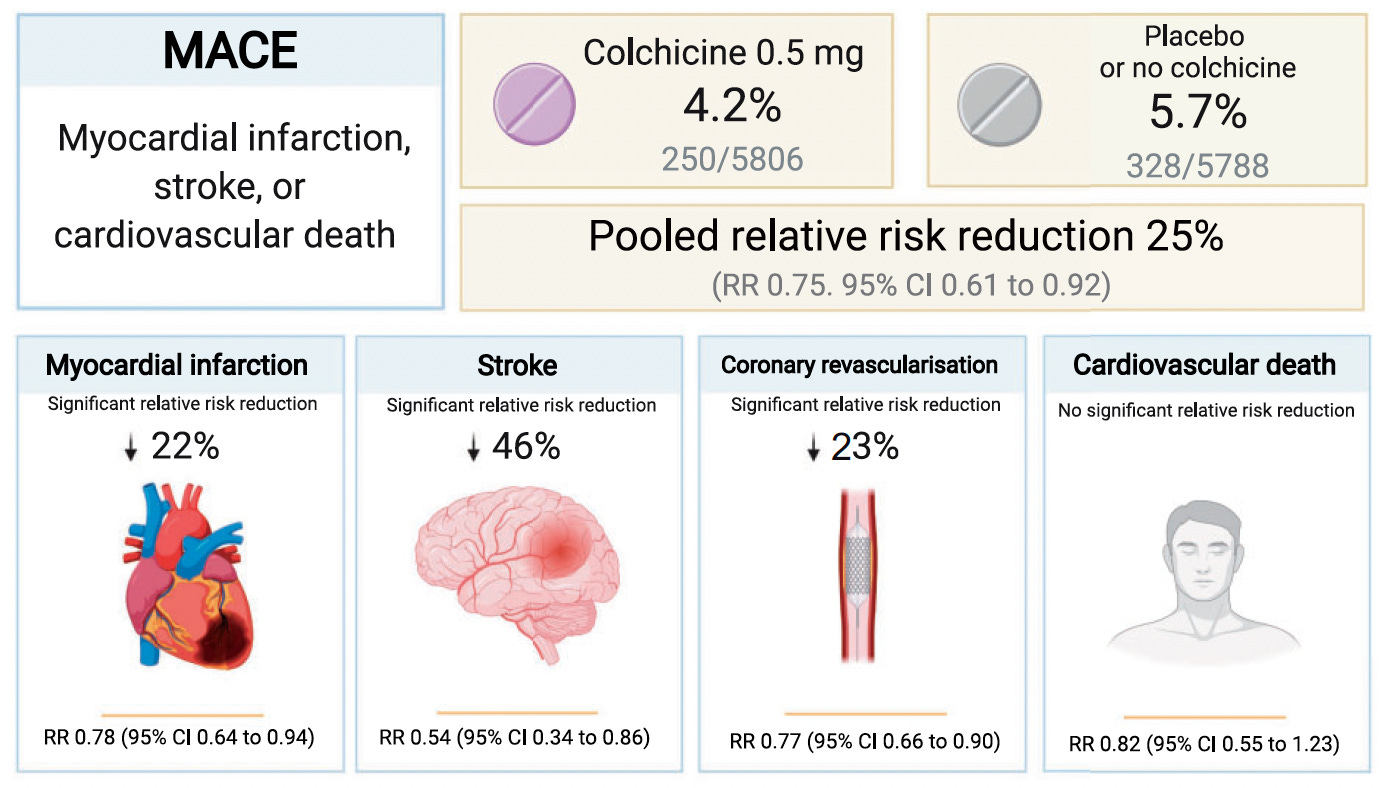
I was doing great till the very end where it shows no improvement in cardiovascular death. How can it improve MI and stroke by so much and not improve death? Because strokes don’t kill? My great uncle had one, lived a couple more years in a nursing home, then just died. Not a good 2 years. Is that what they’re talking about?
Either it doesn’t decrease MI and stroke by enough to cause a statistically significant reduction in acm or alternatively colcichine increases death by other causes as a side effect which resuls in a net zero benefit.
Probably both, that MI and stroke don’t usually kill just make you unproductive, and it lowers immunity or something by killing inflammation. Rats, it seemed like such a nice drug.
Re: optimization. I am also trying to balance lipid lowering / glucose. As are many others I suspect.
I just -restarted Repatha, which worked well but raised glucose. To mitigate that, considering (1) increasing metformin and berberine (2) taking Repatha every 3 or 4 weeks instead of 2 (3) taking a small dose of an SGLT-2 or possibly restarting a pulsed tiny dose of Rybelsus.
On that last one: my insulin is low so the GLP-1 seems like a good idea, but even on the tiniest dose I lost weight, felt terrible and developed kidney stones. I know that GLP -agonists are supposed to reduce/prevent kidney stones but they can also have the opposite effect. So, yes polypharmacy is a challenging project.
Not every medicine works for everyone. If a med causes too much pain or side effects, it’s best to stop and look for another solution. That’s what happened with me and Rosuvastatin. It caused muscle myopathy that I couldn’t handle. So I found Atorvastatin which was much better.
@DeStrider that was my experience with 5mg/day Rosuvastatin also. I’ve switched to 10mg/day ezetimibe and no issues so far. Testing lipids soon and I expect that ezetimibe monotherapy will suffice, but if need be I will try atorvastatin combo therapy in the future.
Also of note that while my current stack of supraphysiological testosterone+daily μ-opioid agonist therapy allows for an incredibly intense resistance training approach (90-120min/day @ 5.3-5.6 days/week) with little soreness, it wasn’t sufficient to prevent rosuvastatin-induced myalgia.
Perhaps some might find AI’s thoughts on the mechanism of rosuvastatin-induced myalgia of interest:
Rosuvastatin-induced myalgia, like myalgia from other statins, is believed to result from multiple mechanisms related to muscle cell metabolism, mitochondrial function, and cellular signaling. While the exact cause is not fully understood, several key pathways are thought to contribute to statin-associated muscle symptoms (SAMS). Here’s a look at the primary mechanisms potentially underlying rosuvastatin-induced myalgia:
1. Reduced Mevalonate Pathway Activity
Cholesterol Biosynthesis Interruption: Rosuvastatin inhibits HMG-CoA reductase, an enzyme involved in the mevalonate pathway, which is crucial not only for cholesterol synthesis but also for the production of other essential molecules like coenzyme Q10 (ubiquinone) and isoprenoids.
Decreased Coenzyme Q10 (CoQ10): CoQ10 is essential for mitochondrial energy production (ATP synthesis). Lower CoQ10 levels in muscle cells may lead to mitochondrial dysfunction, resulting in reduced energy availability and accumulation of metabolic byproducts that can cause muscle pain and weakness.
2. Mitochondrial Dysfunction and Oxidative Stress
Impaired Mitochondrial Function: Reduced CoQ10 levels from statin therapy can impair the electron transport chain in mitochondria, limiting ATP production and increasing oxidative stress. Mitochondrial dysfunction can cause muscle fatigue, pain, and an increased susceptibility to damage.
Oxidative Stress: Increased oxidative stress in muscle cells may lead to membrane instability and muscle fiber injury, which can contribute to pain and inflammation in muscle tissue.
3. Altered Calcium Homeostasis
Statins have been shown to disrupt calcium signaling in muscle cells. Calcium ions play a crucial role in muscle contraction and relaxation, and their dysregulation may lead to muscle cramps, spasms, or pain.
Calcium Leak from the Sarcoplasmic Reticulum: Some research suggests that statins can lead to an abnormal leak of calcium from the sarcoplasmic reticulum (SR), leading to muscle stiffness, fatigue, and myalgia. This calcium leakage can also stimulate proteolytic enzymes, contributing to muscle breakdown.
4. Increased Apoptosis and Muscle Cell Damage
Muscle Cell Apoptosis: Statins may trigger programmed cell death (apoptosis) in muscle cells, potentially through pathways involving increased oxidative stress, mitochondrial dysfunction, and disrupted cellular signaling.
Proteolytic Enzyme Activation: Calcium imbalance and oxidative stress can lead to activation of proteolytic enzymes like calpain, which degrade muscle proteins. This process may exacerbate muscle injury, leading to soreness and weakness.
5. Genetic Susceptibility
SLCO1B1 Gene Variant: Certain genetic polymorphisms, such as variants in the SLCO1B1 gene, affect statin uptake and metabolism in the liver and are associated with a higher risk of statin-induced myopathy. Patients with this variant may have higher circulating levels of rosuvastatin, increasing their risk of muscle symptoms.
Other Genetic Factors: Variations in genes related to muscle function, oxidative stress response, and mitochondrial function can also influence susceptibility to statin-induced myalgia.
6. Immune-Mediated Necrotizing Myopathy (Rare)
Although extremely rare, some patients develop an immune-mediated response to statins, leading to a more severe muscle condition called immune-mediated necrotizing myopathy. This condition involves antibodies against HMG-CoA reductase, leading to persistent muscle inflammation, weakness, and pain, even after stopping statin therapy.
Summary
Rosuvastatin-induced myalgia likely results from a combination of mitochondrial dysfunction, reduced CoQ10 levels, oxidative stress, calcium dysregulation, and genetic susceptibility. While myalgia is a common side effect, its severity and occurrence vary between individuals due to genetic factors and other health conditions. In most cases, symptoms resolve upon discontinuing or lowering the statin dose, or switching to a different statin with a potentially lower risk of muscle-related side effects.
@jnorm Thanks for that. I am now taking Bempedoic Acid (180 mg) + Ezetemibe (10 mg) in one tablet (Brillo EZ). There are 0 side effects and the results are excellent. It dropped my LDL and ApoB to 68. I added 5 mg Atorvastatin and that lowered LDL and ApoB to 48. I wanted to be under 50.
I think the Atorvastatin may cause some myalgia ( I feel a little weakness in my thighs, calves and lower back) but it’s nowhere near as bad as Rosuvastatin and it may be due to the dose I was taking on my GFJ day (GFJ multiplies the dose of Atorvastatin). So, I have skipped my Atorvastatin on my GFJ/Rapamycin day.
Was your dose of rosuvastatin also 5mg? Perhaps the weightlifting was exacerbating the myalgia for me, and I also noticed that cannabinoids strongly amplified it.
I’ve treated bempedoic acid as a 3rd or 4th option behind statins and ezetimibe. Although having researched it less I’m unsure if the literature bears out that approach. Seems like it’s working for well you though!
Hopefully ezetimibe alone will be sufficient for me since my baseline CV markers were pretty good (triglycerides 44, LDL 83, ADMA 103, ApoB 71, Lp(a) <1.16, TMAO 5.7, fibrinogen 164, CRP 1.16, non-elevated BP). Would like to have extremely low CRP like so many on this forum (and also lower ADMA would be nice), but the rest of these parameters are already pretty solid. Of course anabolic steroids can also throw your lipids out of whack (although I’m not going crazy with the dose), so it will be interesting to see where I stand.
@Neo I don’t have any insight into that question so I posed it to ChatGTP
As of now, there are no FDA-approved therapies specifically for lowering asymmetric dimethylarginine (ADMA), a naturally occurring amino acid derivative that can inhibit nitric oxide synthesis, leading to endothelial dysfunction. Elevated ADMA levels are associated with cardiovascular diseases, hypertension, and other metabolic disorders, but direct treatments targeting ADMA reduction are not yet approved.
Research is ongoing to identify effective ADMA-lowering strategies. Some studies have explored indirect approaches, such as:
Lifestyle Interventions: Exercise, healthy diet, and weight management may help lower ADMA indirectly by improving overall endothelial function.
Medications: Certain drugs, such as statins and ACE inhibitors, have shown some ability to lower ADMA in clinical trials, though not as a primary target.
L-Arginine Supplementation: Since ADMA competes with L-arginine, increasing L-arginine intake can sometimes help restore nitric oxide production. However, its effects can vary.
Future treatments may involve targeting ADMA production or its metabolism, but these approaches are still under investigation and are not yet available for clinical use.
Worth noting that Citrulline is generally considered more effective
Both citrulline and arginine are known for their role in boosting nitric oxide (NO) production, which can enhance blood flow and improve exercise performance. However, citrulline is generally considered more effective for this purpose, and here’s why:
Better Absorption: When taken orally, citrulline is more efficiently absorbed by the body than arginine. Oral arginine is partly broken down in the liver before it can reach the bloodstream, whereas citrulline bypasses the liver and is readily converted to arginine in the kidneys, allowing for sustained increases in blood arginine levels.
Longer-lasting Effects: Since citrulline raises arginine levels more consistently, it provides a more sustained release of nitric oxide, which can lead to longer-lasting effects on blood flow and exercise performance.
Less Gastrointestinal Discomfort: High doses of arginine can cause gastrointestinal discomfort in some people. Citrulline is typically easier on the stomach, making it a more comfortable option at higher doses.
Practical Use
L-citrulline is often recommended in doses of 6-8 grams per day to effectively raise nitric oxide levels.
Citrulline malate, which combines citrulline with malic acid, is also commonly used and is thought to improve endurance and reduce muscle soreness post-exercise.
In general, citrulline is preferred over arginine for boosting NO levels because of its superior absorption, better sustained effects, and lower likelihood of side effects.