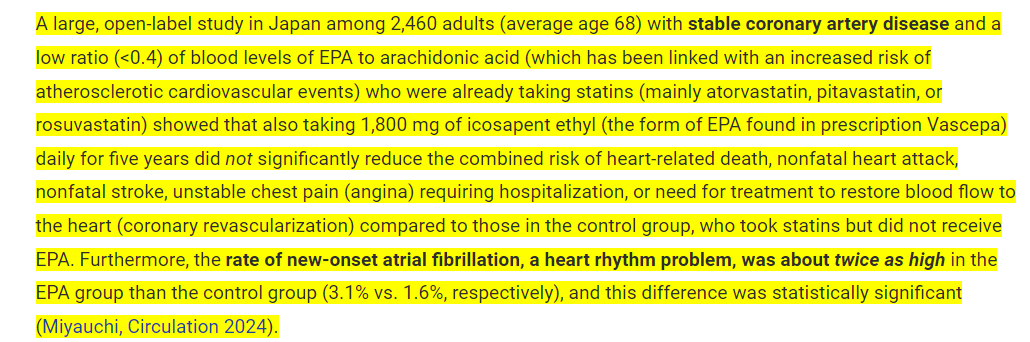
Here is one common combination that doesn’t work out. It’s better to NOT take these two together. I’ll be cutting my Omega-3 dose in half based on this to 1 g a day down from 2 g.
According to ConsumerLab, it appears that taking fish oil with a statin doesn’t convey any lower risk of CVD. In fact, it provides detriments in a doubling of the risk of Afib. So, you may want to cut back on that fish oil if you’re already taking statins. The 1,800 mg of EPA is equivalent to about 4 g of fish oil which has shown to be correlated to increased Afib in other studies. It seems that the statin provides the benefits and the Omega-3 can’t do anything else for CVD on top of the statin. A 1-2 g dose of Omega-3 daily should be fine though.
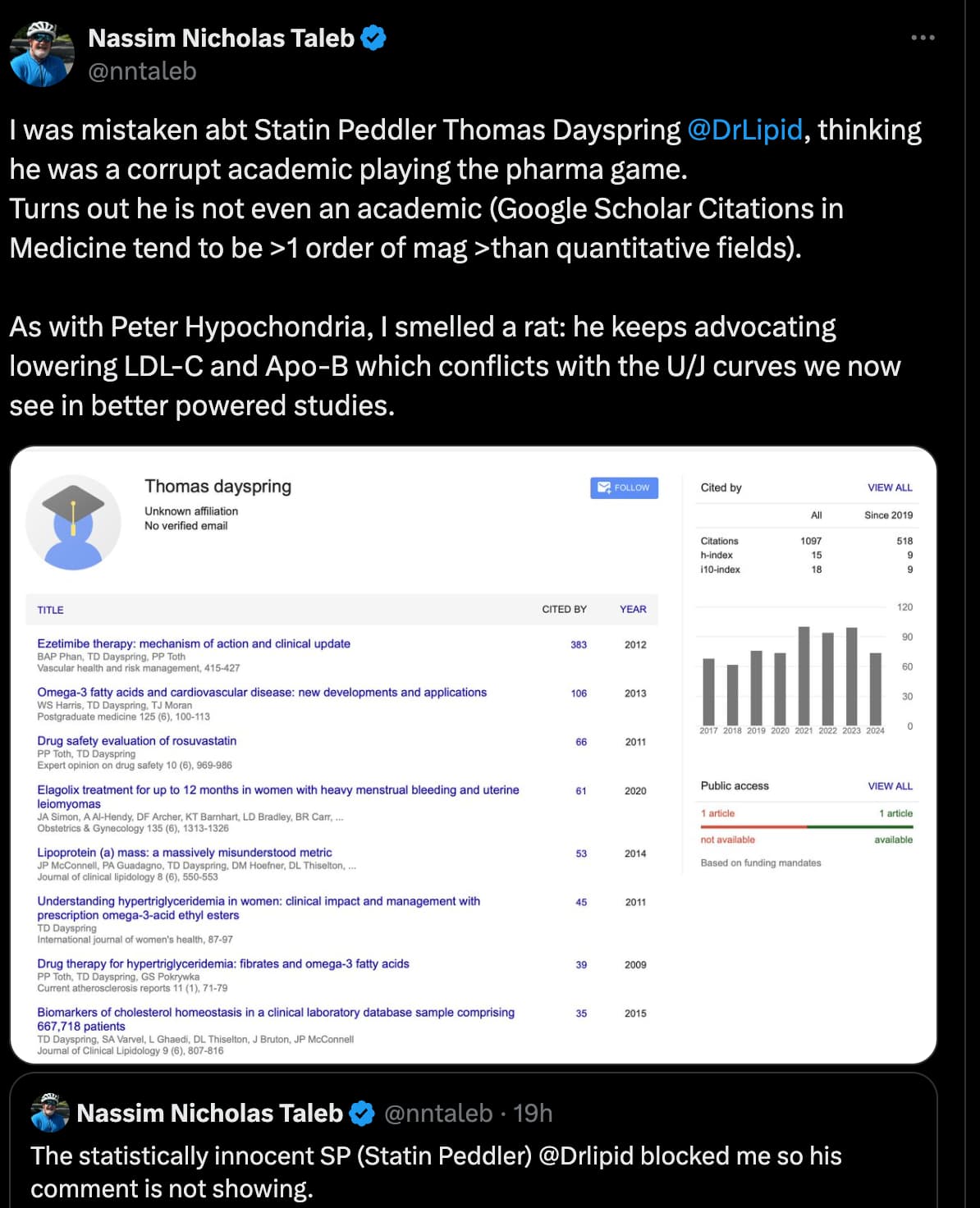
That, however, is an ad hominem attack. I am relatively open minded on statins and the lipids debate. However, if someone wishes to engage they should not use perjorative terms like statin peddler. There is a place in the uk where black swans swim in the river.
I like Nassim Taleb’s books, but I don’t necessarily follow the opinions of hedge fund managers / derivatives traders for cardiovascular advice. The name calling also doesn’t sway me towards his case.
Btw, he can’t stand being referred to like that. He hasn’t been either of those in a really long time.
When it comes to probabilities, statistics, and mathematics, he is very intelligent, but as a person, he is extremely aggressive and makes things personal.
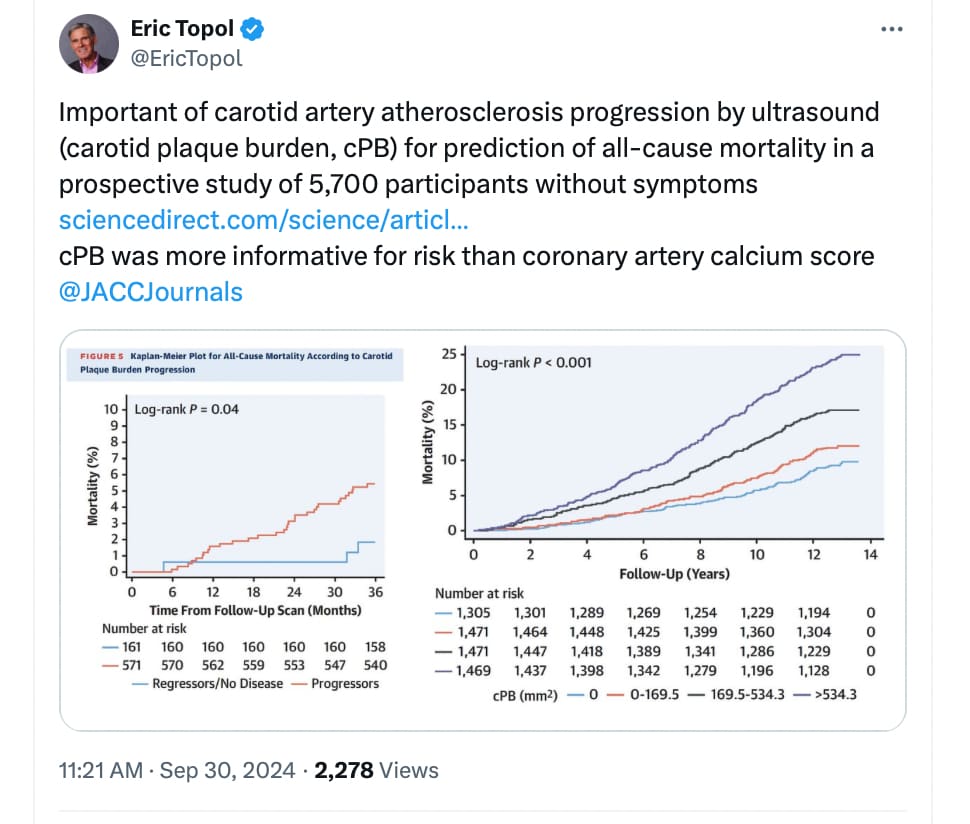
Influence of Subclinical Atherosclerosis Burden and Progression on Mortality
Results
Over a median 12.4 years’ follow-up, 901 (16%) participants died. After adjustment for cardiovascular risk factors and background medication, baseline cPB and CAC score were both significantly associated with all-cause mortality (fully adjusted trend HR: 1.23; 95% CI: 1.16-1.32; and HR: 1.15; 95% CI: 1.08-1.23), respectively (both P < 0.001), thus providing additional prognostic value. cPB performed better than CAC score. In participants with a second vascular ultrasound evaluation, median cPB progressed from 29.2 to 91.3 mm3. cPB progression was significantly associated with all-cause mortality after adjusting for cardiovascular risk factors and baseline cPB (HR: 1.03; 95% CI: 1.01-1.04 per absolute 10-mm3 change; P = 0.01).
Conclusions
Subclinical atherosclerosis burden (cPB and CAC) in asymptomatic individuals was independently associated with all-cause mortality. Moreover, atherosclerosis progression was independently associated with all-cause mortality.
I wonder how informative observational trials are when we have:
RCT’s of high-intensity statins lowering to even lower levels showing decrease in events. I think they were somewhat observational in design as they just looked at events for those who reached lower levels.
Ezetimibe RCT’s, as an add-on to high intensity statins, even further decreasing LDL and events but I don’t know to what level.
PCSK9 inhibitor trials, like for Repatha and Praluent, recruiting people with already low LDL’s on high intensity stains, further decreasing events. For Praluent even ACM in a post-hoc analysis.
Mendelian randomization data showing benefit down to 70 mg/dl apoB on events.
So I think to sum up that that lowering further works, it seems safe in short-term trials although most probably weren’t powered to detect ACM, but we have some signal with Praluent, & MR and genetic studies.
You are of course going to be doing quite well if your apoB hasn’t been elevated (around mean), than if you had a higher apoB, throughout your life. Higher than mean levels are disastrously harmful. It also depends on overall risk, if you’ve had elevated apoB, if you have had high Lp(a)… etc…
We will probably have much more data soon on at least the short term with siRNA PCSK9, CETPi.
But lower is with high certainty better all things equal and I am probably going to target very low levels.
However, I’d like to know what these residual biases can be; it could inform us on lifestyle modifications: it exercise? diet? use of other drugs? etc.
This is where a mechanistic hypothesis helps (but only if it is true). Exercise and nutrition that leads to more efficient mitochondria or does not damage mitochondria seems to be a logical hypothesis.
The trouble is all 3 types of study have limitations when it comes to statins
the rct’s are relatively short, underpowered for Aall cause mortality and often rely on subjective designations of cause of death
the mendelian randomization studies could have confounding biases that we just don’t know about (compensating genetics, developmental impacts etc) and don’t tell us comprehensively about drug safety
and the observational trials have obvious confounding risks.
So given the lack of certainty, im not sure why you’d ignore any type of study. if I had to pick one type it would be MR, but I’m not sure why anyone feels they need to pick just one type of study.
Surely you mean the “LDL-hypothesis” not just statins - the cohort studies and MR do not target the mechanisms statins are supposedly addressing (I say supposedly, as statins are lowering events and mortality more than a proportionate lowering of LDL by any other intervention)
Honestly there is no further debate necessary here. We have a very complete understanding of the progression and mechanisms of ASCVD. Without APOB there can be no ASCVD.
The true question therefore should be:
a) does very low APOB/LDL pose a risk for other kinds of pathologies?
b) specifically: do particular interventions that cause low APOB cause frequent fatal side-effects?
As for statins: we DO have data for all cause mortality out of the major trials for Rosuvastatin, Atorvastatin and Simvastatin. These trials show statistically highly significant lower ACM. The absolute effect of course is small after just 2 years. Then again: it’s interesting to get clear data on ACM in people after 2 years at all. But for Rosuvastatin and Atorvastatin we also have long-term follow up data of up to 20 years after the unblinding - confirming lower ACM.
I really don’t understand the skepticism about statins. They have better data than PCSK9 - not just more data. But better outcomes for ACM and cardiovascular mortality. Lowering your LDL by 40 mg with a statin will lead to better mortality than lowering it by PCSK9. Not even considering that statins are a small fraction of the costs.
Is there something specific about HMGCR inhibition that makes it better for ACM than PCSK9i or NPC1L1 inhibition or were it just a matter of being detected in the trials? Kind of like luck?
I am still not convinced of this hypothesis. If LDL-exposure was all that mattered, the effects of statins and PCSK9 inhibitors would only be seen after 10 years or longer and plaque would never regress nor stabilize despite various studies showing that it does.