Did you find any input re @adssx question in it?
The Lancet paper suggested that every 1 SD increase in lifetime apoB above the mean causes a 60% lower chance to live to 90th percentile lifespan (1 SD = 24 mg/dl) (mean about 100 mg/dl). I don’t know about the other papers.
4 Likes
Dr. Thomas Dayspring is a big proponent of wiping ApoB and LDL out.
Thomas Dayspring on X: “This paper is mandatory for those who want to better understand & then eliminate atherosclerosis. All including LDL deniers must realize that humans were never meant to harbor the LDLc (apoB) levels that are now commonplace. NORMAL LDL-C is 20-40 mg/dL https://t.co/KXl2L60sQc https://t.co/hGibTLPA1S” / X (twitter.com)
3 Likes
The paper Dayspring quotes is a little suspect. It references two studies supporting the “NORMAL LDL-C is 20 - 40 mg/dl” stating that …
“This value is consistent with the LDL-C levels observed among hunter-gatherer populations [65,66].”
Neither of those studies support the sentence.
The first shows an LDL-C of 62 in The Hadza
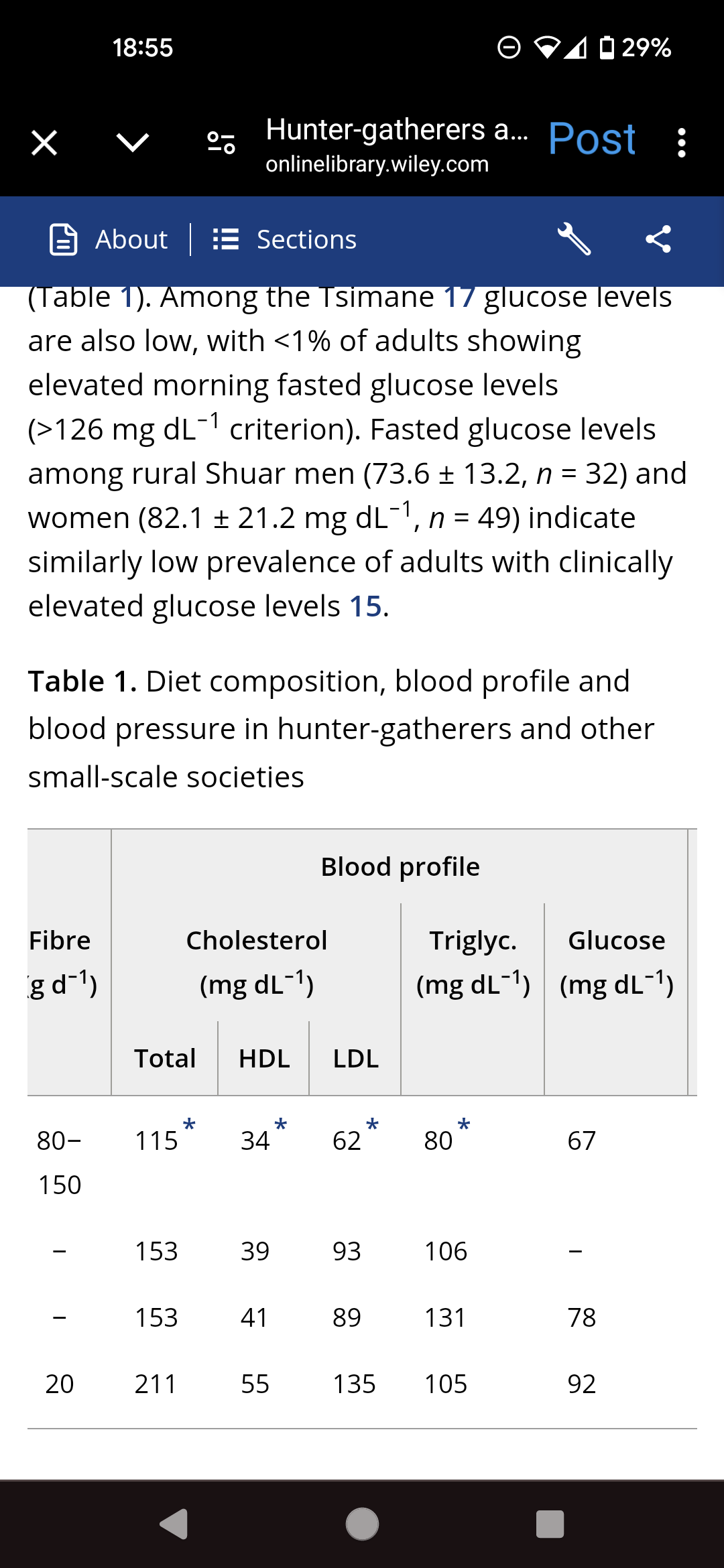
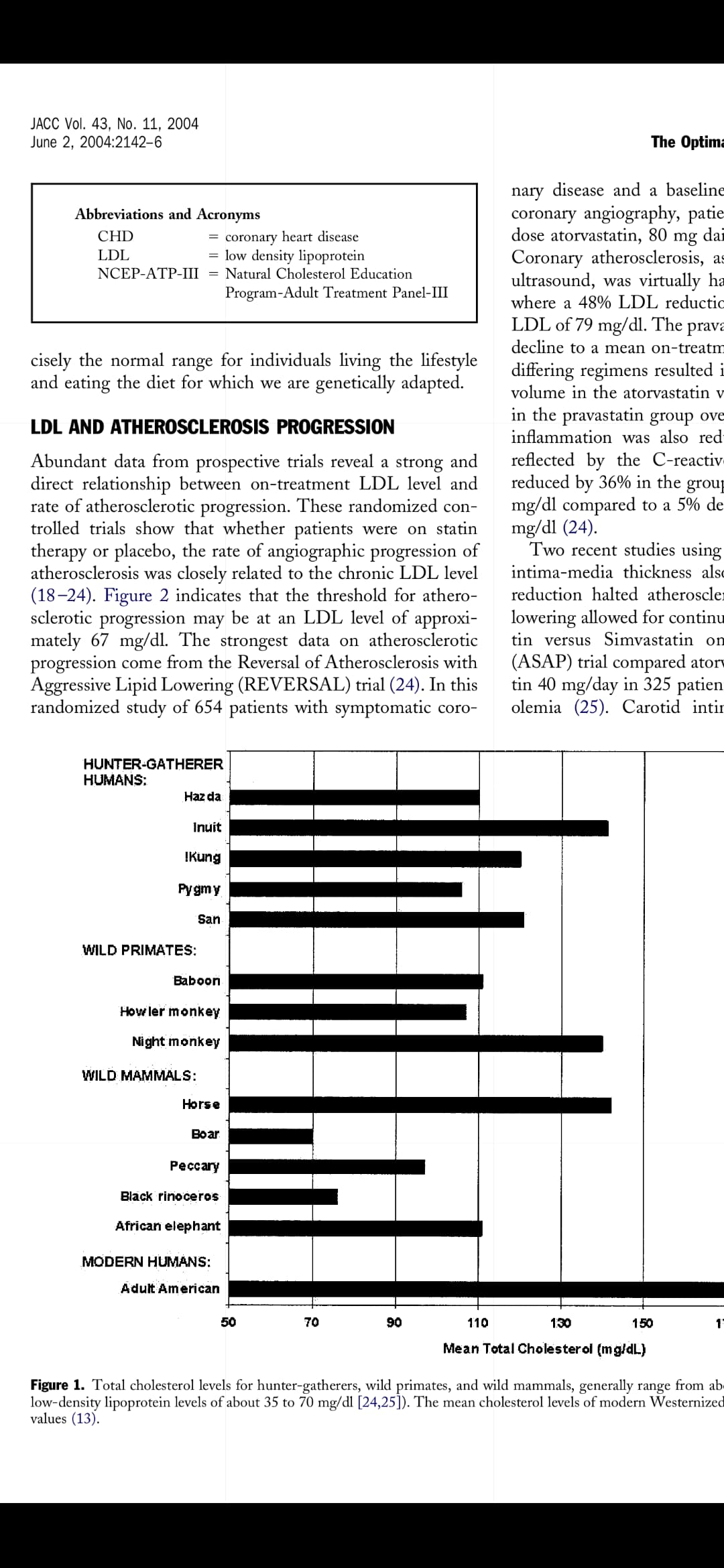
The second study shows total cholesterol only, but at levels suggesting ldl-c above 40 ng/dl for all the native groups
1 Like
I’d say those papers actually support a NORMAL ldl-c 40 to 65 ng/dl
3 Likes
The technique I use is inject the 15 mg / 0.5 mL pen into a sterile 10 mL bottle - carefully. Then inject 1.0 mL of bacteriostatic water into the sterile bottle. Now you have 15 mg / 1.5 mL in the bottle.
If you wanted a 5 mg dose, you can withdraw 0.5 mL from the bottle. 7.5 mg dose = 0.75 mL. And etc.
The volume of fluid is large enough this way to practically divide. And the bacteriostatic water should help with maintaining sterility. Put the bottle in the fridge for a week and use it again.
Your thoughts?
This is probably okay - however, it is really unclear from the manufacturer details (as I looked into this in the past) - what the appropriate dilutent would be. Most peptides do fine in bacteriostatic water, but they have the formulation at a specific pH and I have no idea what effect you might have on the actual active remaining peptide by doing this. It’s an unknown - and I tried to sort through this looking at the full PI on Tirzepatide … and it remains unclear.
There is a real convenience of doing this into a vial. I also really like when my patients aren’t in a state where the compounding companies are pretty well locked out, as just being able to Rx this from Empower Pharmacy in Houston is great, as they have a 17 mg/mL, 2 mL vial (total 34 mg) that delivered with supplies is ~$330. Then we are fine doing doses from this and micromanaging have them go up and down. For folks on Semaglutide - they do 12.5 mg for ~$250. Either way, a really good quality medical grade product. Requires a prescription.
Hopefully that helps … but for the time being, if splitting, I’d not dilute as I have no evidence that dose #2 and #3 you are pulling having sat for a week or two haven’t significantly degraded due to the dilutent.
2 Likes
I appreciate the information. Thank you.
Good interview between medical professionals regarding Bempedoic Acid.
Their thoughts on why BA did not reduce all cause Mortality was enlightening.
Also interesting was the idea of adding a statin to BA as well as Ezetemibe.

4 Likes
Thought this was very interesting on the possibility of reviving people beyond just CPR and defibrillators.
" He told me about one patient who received CPR for three hours, and was taken to two different hospitals, before Marinaro’s team put him on ECMO. “That guy walked out of the hospital,” he said."
How ECMO Is Redefining Death
The machine, called ecmo , which stands for extracorporeal membrane oxygenation, removes carbon dioxide from the blood and replaces it with oxygen. It can perform the work of the heart and lungs entirely outside the body.
https://www.newyorker.com/science/annals-of-medicine/how-ecmo-is-redefining-death
Paywall-Free Version: How ECMO Is Redefining Death (NewYorker)
6 Likes

3 Likes
Hey! Sorry for the late reply. I just put it in sterile 2 milliliter vials that I got on Amazon… I then draw up with a 29 gauge 1 mL syringe by easy touch, I only draw up .5 mL or 50 units on the syringe, and get 70 mg every two weeks this way. It has reduced my LDL down in the 30s, my ApoB is 42 I believe last I checked.
4 Likes
Hi Neo, I replied to RapAdmin Above, but didn’t know how to tag you, to add further context, with the LDL in the 30s, in addition to the 70mg of Repatha I also have been using Ezetimibe 10mg and Bezafibrate 400mg a day. I use the Beza for other stuff, it doesn’t lower LDL very much. It will lower ApoB though due to its triglyceride lowering and thus VLDL particle lowering
4 Likes
Have we seen anything in MR on longevity I other studies on HMGCR (the statin) pathway
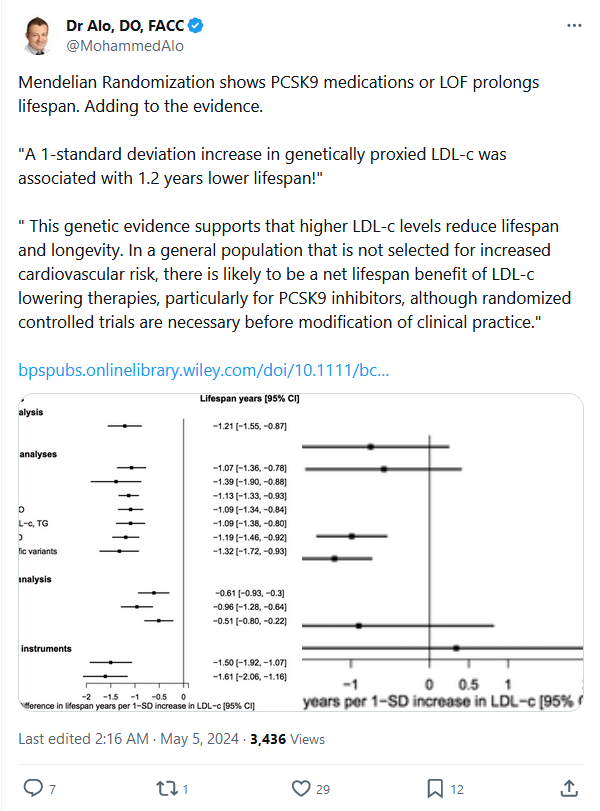
Here it’s only the PCSK9i pathway that was statistically significant?
Gene-specific Mendelian randomization analyses showed a significant effect of LDL-c modification through PCSK9on lifespan (−0.99 years, 95% CI −1.43, 0.55, P = 6.80 × 10−6); however, estimates for HMGCRand NPC1L1 were underpowered.
What exactly is the optimal LDL level from this study and what was the standard deviation value?
It looks like the baseline is 100 and the standard deviation is 38.7. so for every 38.7 pts above 100, you live 1.2 fewer years.
That sounds correct, so if there isn’t many years that keeping lipids low would give, it would dramatically increase healthspan to avoid many heart attacks, strokes, etc. If low enough, almost all if not all of the former. The study results kind of break if you think in the rare situation someone would avoid other causes of death, as max lifespan wouldn’t be limited by cardiovascular disease. Like in the case of possibly reversing aging a bit or slowing it down.
1 Like
That story if true would be remarkable! As an ER Physician, getting patients acutely on ECMO is very difficult, but even with quality CPR, it is almost certain that even with return of circulation at even 30 minutes, the neurologically intact survival is absolutely dismal.
The outcomes if, shortly after arrest, in a younger/middle aged individual who isn’t awful protoplasm, if able to acutely get on ECMO is still dismal, but some will do okay.
This is a technology that has it’s uses, and increasingly in some centers is used acutely, but often is a very high cost high resource approach with some success stories, but a lot of high costs with dismal outcomes would be my experience.
Published data indicates ECMO within 60 minutes of cardiac arrest can increase survival from <5% to 30%. In one trial reporting neurologically intact, the 530 pts who got this, 91 (17%) had what was considered neurologically intact survival. Again - really must be within 60 minutes, and the sooner the better.
3 Likes
Maybe he walked out of the hospital as a brain-dead Zombie… ![]()
2 Likes
I’m struggling with the decision as to whether to start on a low-dose statin. I’m considered low risk - 40 years old with LDL-C around 95 and no risk factors/otherwise in good health. Ideally I would like my LDL-C to be even lower, and I’m generally doing everything I can on the diet/exercise front. My main hesitancy re statins is that there seems to be fairly convincing evidence demonstrating that, for someone low-risk like myself with a CAC score of 0 (as far as I know), statins provide no benefits (see, e.g., this study, among others: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6309473/ ). I’m familiar with the evidence indicating that lower is better when it comes to LDL-C, but that evidence seems less directly relevant to this particular question. What am I missing?
1 Like