There was a higher rate of incident dementia in the No Statin group (4.7%) versus the Statin group (3.2%). Additionally, we observed a 22% all-cause mortality benefit associated with statin therapy.
Does anyone have access to the full paper?
Anyway, I’ve just started ezetimibe 10 mg. If it’s not enough to lower my ApoB I’ll reconsider atorvastatin 10 mg. (Still praying for obicetrapib to show amazing results and to be approved in the next 12 months )
What data is that, isn’t it just lipid lowering in 300 patients with FH? I don’t think you will have enough data that makes it look better than any other drugs at that point then?
I was as just saying that there is more data than the 300 patients
Is personally def think twice to use a new approved med in the beginning if there are relatively good alternatives. (And probably even where there are no alternatives- eg re Lp(a) for me).
(Btw, think that the number of patients across their trials is larger than 300)
Yes, BROADWAY, which is due to finish in September, has 2.5k patients. PREVAIL (until 2026) has 9k participants. And they have smaller trials with 100–400 participants.
This reminded me of inclisiran which is approved because it lowers LDL, meanwhile as larger trials are underway (it works via PCSK9 but only needs to be taken twice yearly).
If obicetrapib is as good as preliminary data and MR suggest, then it could be a replacement for atorvastatin, at the very least for statin-intolerant people and for people with uncontrolled diabetes (despite being on antidiabetic drugs). Also for people with Parkinson’s disease?
I don’t know about uncontrolled diabetes but statins are indicated still for those with diabetes. If obicetrapib is better than PCSK9 inhibitors or bempedoic acid for statin intolerant at that point it seems unlikely to me. Just let’s not get caught up in the storm of stories. Hard endpoints in clinical trials matter a lot although MR is nice.
Have you taken a look at the large clinical trials?
(I can recommend if interested adding a column in clinicaltrials.gov with enrollment then downloading the excel file and sorting by size). But I can take a look, I am mostly interested in cardiovascular death as I’ve heard ezetimibe reduces it.
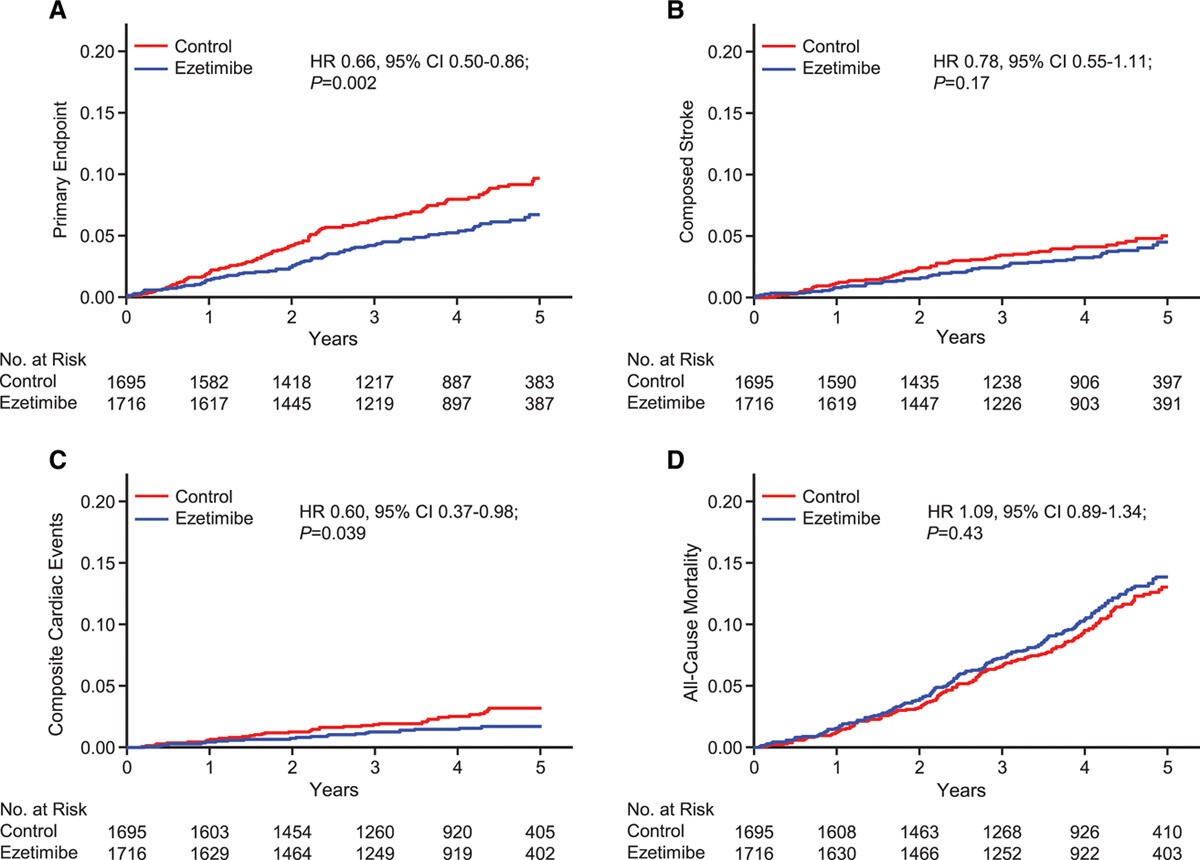
Since publication of the included systematic reviews, 2 new ezetimibe RCTs have been published. A 2019 open-label RCT compared 10 mg of ezetimibe once a day versus no treatment (no other lipid-lowering therapies were allowed) in 3796 participants 75 years and older without a history of coronary artery disease (CAD) for approximately 4 years.46 Ezetimibe significantly reduced the incidence of the composite outcome of sudden cardiac death, fatal and nonfatal MI, coronary revascularization, or fatal and nonfatal stroke by approximately 35% (ezetimibe 5.2% vs 7.8%) but had no effect on all-cause mortality. However, the trial had multiple major limitations (only 63% of the planned sample size enrolled, the trial had an open-label design, and 28% of participants withdrew or were lost to follow-up).
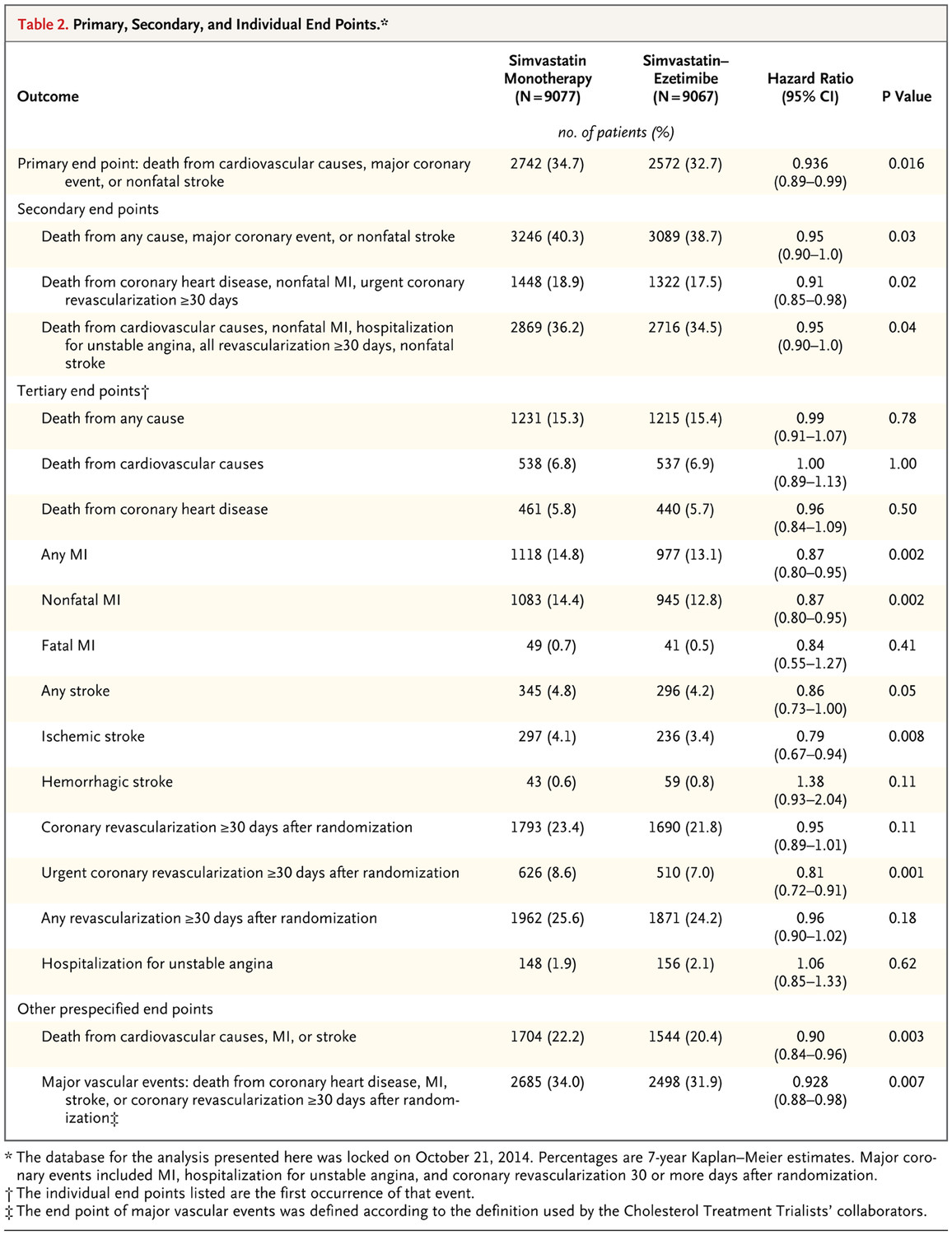
I looked at all the large trials, it seems only IMRPOVE-IT will inform our decision on the clinical trial side for ezetimibe. I’ll have to read it again carefully but it decreases composites, non-fatal MI’s, stroke, no detection of all-cause mortality and no decrease in cardiovascular deaths unlike what I have heard. It’s interesting ezetimibe decreases stroke if it it’s only active in the gut, so that means serum LDL have an effect on that?
That ACM curve might just be random risk, ACM can be very noisy like if someone slipped on a banana peel in the ezetimibe group, unrelated to the drug. Needs very large trials and duration especially for something with not a large effect on LDL like ezetimibe.
No between-group differences in cardiovascular mortality or in the rate of death from any cause were anticipated or observed in IMPROVE-IT, findings that are consistent with those in trials of intensive-dose versus standard-dose statin therapy.
For all the noise in the ACM data, it would be nice to see a benefit in ACM for once, even if it’s not statistically significant.
Given that cvd accounts for a major % of all cause deaths in the age cohort, and banana peel deaths are pretty rare, it’s interesting that multiple studies find a cvd benefit but a non-statistically-significant increase in ACM.
I wonder they’re dying of.
Yes but the absence of any positive sign of ACM benefit is disappointing after almost 5 years. It’s a large trial and well over a third of deaths are from cvd in that cohort. So the fact that acm is numerically higher in the ezetimibe group is… “disappointing”