Because of my low Lp(a), should I be concerned about Repatha?
Low Lp(a)? Consider yourself lucky!
1 Like
From Gemini Pro:
Clinically low levels of Lipoprotein(a) [Lp(a)]—typically defined as <10 mg/dL or <25 nmol/L—are overwhelmingly established as cardioprotective and beneficial for human longevity due to a drastically reduced risk of atherosclerotic cardiovascular disease (ASCVD) and aortic stenosis,
2 Likes
That statement from Gemini Pro is kind of confusing – makes it sound like having some (very low level) is cardioprotective when I think it means to say that the absence of Lp(a) is what is beneficial.
Actually I think there is some small protective benefit of Lp(a) as a protection against infection but over around 30mg/dl it is bad --causes inflammation in the blood vessels.
My Lp(a) was 40 mg/dl before I started Repatha. It went down to 27.
My Lp (a) is 9. Will Repatha make it even lower? And if it’s that low why it didn’t protect me from having a high calcium score? I suspect that either my Lp (a) or CAS were calculated incorrectly.
Having a low Lp(a) doesn’t guarantee a low calcium score if your LDL particles have been elevated much or most of your life and/or if you’ve had some chronic low grade inflammation. Things would likely be considerably worse if you also had high Lp(a).
5 Likes
You have side effects from those 3 different classes of medication? I don’t know how to explain that. Are you being prescribed these by a doctor?
LDL 5.5 = ~200mg/dl, which is very high. And you have a positive calcium score. That means you already have established cardiovascular disease. You’ve built plaque, and it’s been going for long enough to go through cycles of repair and calcification. And with LDL of 5.5 mmol/L, you will be building more plaque as time goes on.
How old are you?
Tadalafil may be cardioprotective by lowering cardiac stress, but it doesn’t affect lipids. Rapamycin may be protective by lowering inflammation, but it generally makes lipids worse.
Mine wasn’t affected at all by Repatha. I think it’s quite unreliable as an Lp(a)-lowering agent.
The CAC might have been worse if your Lp(a) was higher. And of course there are contributions from ApoB (LDL-C etc), and others. Atherosclerosis is generally “area under the curve” thing, where the longer you went with higher lipids and other risk factors, the higher the CAC will go, with some lag time. You can roughly imagine that 10 years at 200mg/dl is equivalent to 20 years at 100mg/dl in terms of total accumulation.
2 Likes
Exgenous androgens lower Lp(a) 25 to 75%, but then you have to contend with low hdl, líber strain, and elevated ldl. No free lunch!
1 Like
I’m currently experimenting with oral enobosarm (ostarine) 6mg daily, which has completely normalized my Lp(a). LDL and ApoB are extremely low thanks to modern pharma and liver enzymes are normal, courtesy of TUDCA. I’m going with the theory that any risk from low HDL is more than offset by the 75% drop in Lp(a) and my very low LDL/ApoB. Next I’ll lower the enobosarm dose to 3mg and retest Lp(a) to see what the lowest effective dose is.
To be clear, enobosarm is still experimental (in stage 3 clinical trials) and is not approved for any use at this point and comes with risks of serious side effects such as (but not limited to) suppression of endogenous testosterone/estrogen synthesis. Its effect on Lp(a) has never been tested in clinical trials.
Note: I posted a few months back that it was IGF1-LR3 that was responsible for my decreased Lp(a), but I had no idea at the time that the enobosarm I was also taking off/on could have such a dramatic effect on Lp(a). Stopping enobosarm while continuing LR3 caused my Lp(a) to climb back to 175. Stopping LR3 and restarting enobosarm quickly dropped Lp(a) back to 50.
5 Likes
I don’t think Lp(a) could ever be too low. I am pretty sure lower is better with no floor.
my cRP bounces around like a pinball based on what injury I have inflicted on my body. A bruise or cut and it jumps to 8-10. Meanwhile my ESR stays below 5 and often at 1
3 Likes
well, mine is at 13 so I don’t know if it can go any lower lol, blessed with that not so much with LDL at 125
If your LDL is 125, I’d lower it to below 70, IMHO.
I am really loving pitavastatin 2 mg. I feel so much better. I didn’t realize that Atorvastatin 5 mg EOD was causing that much muscle weakness and fatigue until I switched to pitavastatin! I’m never going to use another statin again.
8 Likes
yes that’s the plan. Taking 2mg pita and 5mg ezetimibe for last 3 months. Hopefully that will be enough to lower it. I plan on testing in a month or so to see if its working or not.
4 Likes
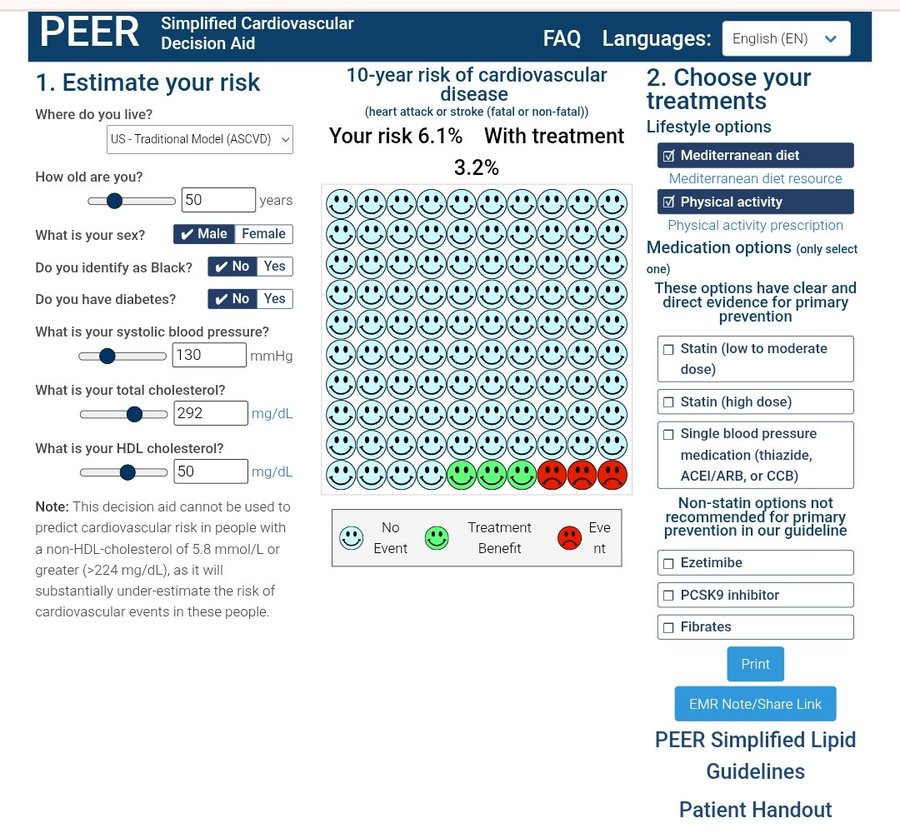
an interesting tool: (not quite as granular as I would like… for example I’d like to see LDL-C, APO-B, LP(a), etc.
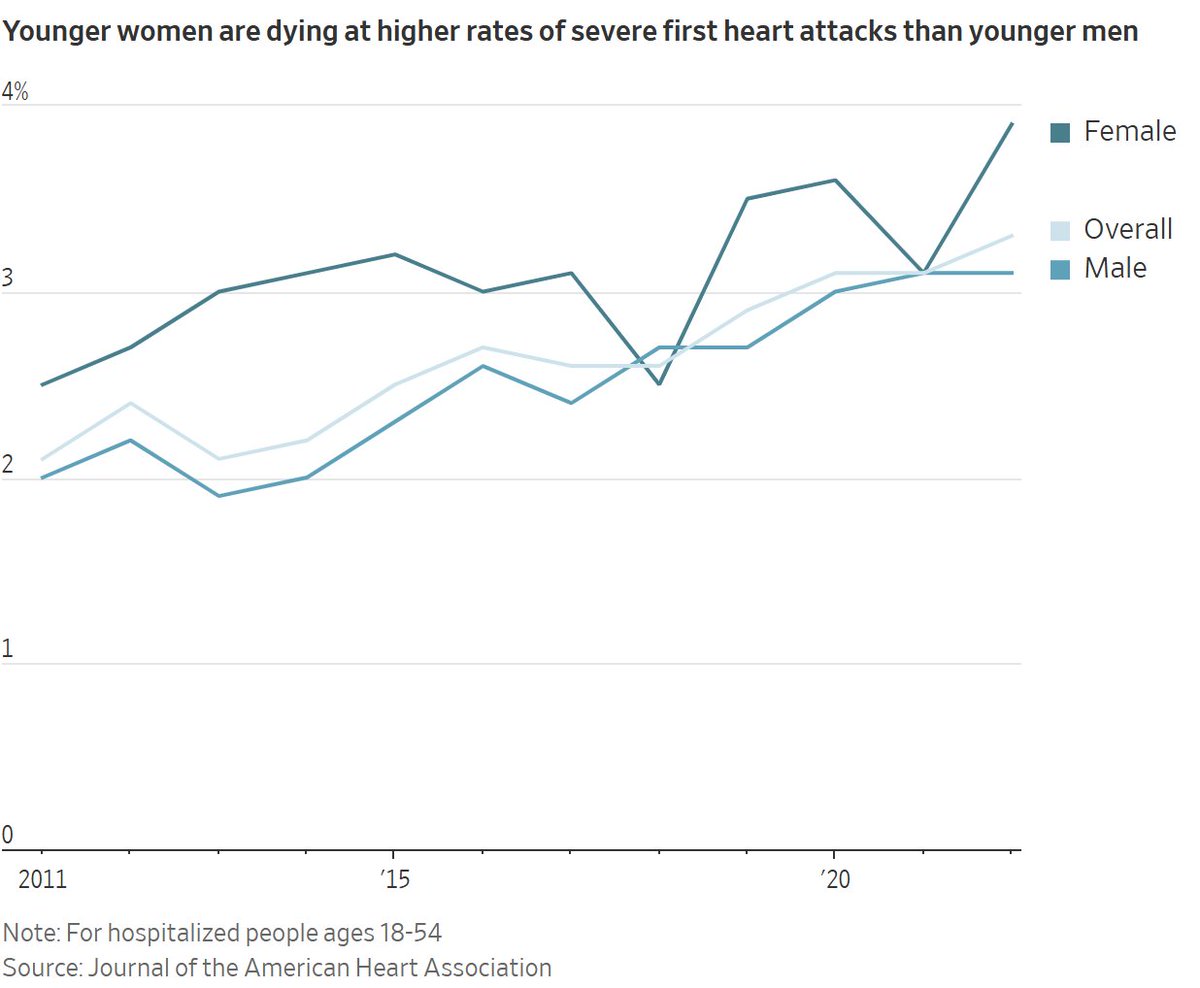
More Americans Under 55 Are Dying of Severe Heart Attacks
Proportion of adults ages 18 to 54 who died of severe first heart attack rose 57% between 2011 and 2022, new study finds
The last thing someone in their 30s or 40s should worry about is dying of a heart attack. But new research shows more are.
The proportion of adults ages 18 to 54 who died in a hospital of a severe first heart attack rose 57% between 2011 and 2022, according to a new study published Thursday in the Journal of the American Heart Association.
Most of those who died were men, but women died at higher rates than men.
The study offers the latest evidence of worsening health among younger U.S. adults, including deaths from conditions traditionally tied to aging, such as heart disease and cancer.
Poorer health among younger adults is one reason heart disease remains the leading cause of death in the U.S., despite decades of medical advances that have saved millions of lives from heart attacks and other life-threatening cardiac events.
Read the full story: More Americans Under 55 Are Dying of Severe Heart Attacks (WSJ)
- Title: Sex Differences in Outcomes of Young Adults Hospitalized With First Myocardial Infarction From 2011 to 2022
- Lead Author: Mohan Satish, M.D.
- DOI: 10.1161/JAHA.125.046517
Why do you think that is. My observation is that young people probably have diets at least as healthy as young people of my era. There is certainly more information about healthy foods and diet. I know it’s hard for young people to understand the days before the internet. Television was full of harmful diet information. Can young people even imagine that real doctors thought smoking was safe. My generation ate tons of things like bacon, cake, pies, ice cream, candy bars, etc. So, no, I don’t think diet is the cause.
Two things that I observe (I have grandkids that are still young) are lack of physical activity and much more stress caused by such things as social media.
My bet is that life is much more stressful for young people than it was when I was young.
“Chronic stress** significantly increases the risk of life-threatening conditions like heart disease, stroke, and cancer. Prolonged exposure to stress hormones like cortisol causes cumulative “wear and tear” that can lead to premature mortality”
6 Likes
My friends and acquaintances who died in their 50s of CVD were obese and some morbidly so. They also didn’t take any lipid controlling meds.
2 Likes
I am the same my hsCRP jumped from .4 to 2.7 after I fractured my hip. Lp(a) it seems to make everything worse, but it has a more modest effect on a CAC score. It is a small fraction of the lipids compared to LDL-C. If both are high, I would blame the CAC on the LDL-C or other factors.