Ok I just got my results back. On 2.5mg Rosuvastatin & 10mg Ezetimibe, LDL was 47. After switching to 2mg Pitavastatin and keeping Ezetimibe, my LDL went up to 57.
So it’s a 10 point increase. I want to continue this particular statin since I believe it is the reason a lot of of my weight lifting joint pain went away so I will ask to increase it to 4mg. I would imagine that would get it back down to under 50.
I am awaiting the ApoB result but it is usually about 10 points higher than my LDL, and I don’t like to see my ApoB over 60 so that’s why I intend to increase to 4mg Pitavastatin.
Pitavastatin is considered a moderate intensity statin, with 4mg being roughly equivalent to 10mg rosuvastatin. Of course, there are individual reactions, some people’s lipid levels react stronger to one statin vs another. I take 4mg pitavastatin, and get slightly lower LDL than from my previous 10mg atorvastatin. But that’s the upper limit on pitavastatin (there were some studies in Japan where 8mg was used successfully), if you want to go high intensity statin, you have to go to atorvastatin 40/80mg or rosuvastatin 20/40mg. If you don’t need high intensity statin, pitavastatin is a great option.
For whatever reason, my LDL was 27 I think when I was on 5mg Rosuvastatin (w/ Ezetimibe). So clearly for me, Rosuvastatin is much stronger. I have seen some funky LDL peaks and valleys though so who knows. I just love that I have been able to lift pain free and back to my heaviest weights again simply from switching to Pitavastatin (unless there is another cause but that’s the only thing I changed)
I don’t think the expiry dates matters that much for meds:
You should do a blinded experiment to control for the placebo and nocebo effect which are powerful. Depending how long until you have the effect you’ll have to use one bottler longer until you check.
If I were ever able to get mine to 70, you’ll never hear me complain about it, ever LOL. Moving to 4mg might work but that seems to be the upper limit and sides may creep in at that level, so If I were you, I’d change nothing (for a while) unless it keeps moving higher (on your next test) especially given the fact that your joints seem to be loving Pita at 2mg. Just MO.
Immune system overreactions may be the true culprit of cardiac illness—and lifesaving drugs can calm them down
Doctors have been drilled for decades on the four big risks for heart disease, which kills more Americans every year than any other illness. The fearsome foursome: hypertension, smoking, high levels of “bad” LDL cholesterol and type 2 diabetes. Yet for just as long cardiologists have seen patients who have none of these problems die from heart ailments. And the heart specialists haven’t had the slightest idea why.
Up to a quarter of the people admitted to hospitals for heart attacks don’t have any of these four risk factors. Mysteriously, these “low-risk” heart disease patients actually have the worst outcomes. A 2023 analysis found that hospitalized acute coronary patients without any of the four hazards were 57 percent more likely to die compared with those who had at least one.
If the big known risk factors miss one in four patients, they still predict trouble as expected for the remaining three. That’s a good record. But it also means that of the roughly 920,000 Americans who die of cardiovascular disease every year, about 230,000 of them will have done so for no understandable reason.
This deadly puzzle has haunted cardiologist Paul Ridker for years. “I remember saying to myself that there must be some other fundamental determinant of heart disease,” says Ridker, who is director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital in Boston.
Dozens of studies and clinical trials later, Ridker thinks he has found the missing piece. His work, along with that of other researchers, now suggests that chronic inflammation—a prolonged and body-damaging state of immune system activation—may be the hidden factor that accelerates cardiovascular problems to a dangerous and deadly state. When cholesterol builds up in the arteries, it shape-shifts into a sharp and jagged form the body no longer recognizes, provoking the immune system to wage war against it and blood vessels. It is a battle with no winners, and the wreckage it leaves behind ends in heart attacks and strokes.
Initially treated with skepticism, this idea now is becoming widely accepted by other scientists. Heart disease is “a disease of inflammation,” says Kathryn Moore, director of the Cardiovascular Research Center at New York University’s Grossman School of Medicine. And in the fall of 2025 the American College of Cardiology recommended that health-care providers routinely screen patients for inflammatory proteins.
Yes that’s all correct and that’s what I am hoping for. I am still waiting to hear back if my cardiologist will raise my dose to 4mg (they’re being slow on the health portal) but if it’s an issue, I’ll just order it myself from an Indian pharmacy so I can take the higher dose.
The prevailing clinical paradigm for managing cardiovascular disease—waiting for established atherosclerosis to manifest before aggressively intervening—is fundamentally flawed and actively costing lives. For decades, target thresholds for Low-Density Lipoprotein Cholesterol (LDL-C) have been physiologically mismatched to the actual biological requirements of human lipid homeostasis. The core thesis of the reviewed material is that “normal” cholesterol levels (100–130 mg/dL) are pathogenic, and the widely accepted clinical target of <70 mg/dL provides a false sense of security, allowing for the silent, continuous accrual of subclinical plaque.
Recent trial data from 2026 provides unequivocal evidence that aggressively lowering LDL-C to ultra-low targets (~40–55 mg/dL) yields profound cardiovascular mortality and morbidity benefits. The VESALIUS-CV trial demonstrated that high-risk primary prevention patients (diabetics without macroscopic plaque) achieved a 31% reduction in major adverse cardiovascular events when LDL-C was driven to a median of 44 mg/dL using PCSK9 inhibitors. Similarly, the ES PAVE trial reported a 33% relative risk reduction in major events when targeting <55 mg/dL versus the standard <70 mg/dL. Furthermore, imaging data from the PESA study indicates that atherosclerotic progression initiates at a plasma LDL-C threshold of approximately 50 to 60 mg/dL.
Achieving these targets does not strictly require cost-prohibitive biologics. The generic agent ezetimibe, which operates synergistically with statins by blocking intestinal cholesterol absorption, remains staggeringly underutilized, prescribed to only 6% of eligible patients. Ultimately, the data demands a proactive, aggressive shift: lipid-lowering intervention must occur earlier in the disease etiology, and physicians must titrate dual-therapy pharmacology to drive ApoB-containing lipoproteins well below conventional targets to successfully arrest atherogenesis.
II. Insight Bullets
The physiological baseline for healthy LDL-C is far lower than clinical guidelines suggest; loss-of-function PCSK9 mutations result in lifelong LDL-C levels as low as 14 mg/dL with zero observed pathology.
Natural genetic absence of the PCSK9 protein confers an approximate 88% reduction in lifetime coronary heart disease risk.
Atherosclerotic plaque genesis and subendothelial lipid retention initiate linearly starting at an LDL-C threshold of roughly 50 to 60 mg/dL.
Conventional LDL-C targets of <70 mg/dL provide false reassurance; nearly 20% of acute myocardial infarction hospitalizations occur in patients who are “at target” below this threshold.
Waiting for atherosclerosis to visibly declare itself on imaging before aggressively treating LDL-C surrenders the critical primary prevention window.
In diabetic patients without significant pre-existing atherosclerosis, driving LDL-C to a median of 44 mg/dL reduces the composite risk of heart attack, stroke, and cardiovascular death by 31% (VESALIUS-CV).
Early intervention with PCSK9 inhibition revealed an exploratory 24% relative reduction in all-cause mortality, underscoring the compounding benefit of early plaque prevention.
For secondary prevention, pushing the LDL-C target from <70 mg/dL down to <55 mg/dL results in a 33% relative risk reduction in major cardiovascular events.
A mere 10 mg/dL absolute drop in LDL-C (from 66 to 56 mg/dL) translates to more than halving the rate of subsequent non-fatal myocardial infarctions.
Driving LDL-C to ultra-low levels (<55 mg/dL) presents no clinical signals of harm, with no increased rates of hepatotoxicity, new-onset diabetes, or myopathy over multi-year horizons.
Even in completely asymptomatic adults with zero conventional risk factors, LDL-C levels in the 100-130 mg/dL range correlate with a high probability of subclinical atherosclerotic plaque.
Ezetimibe is a highly effective, off-patent pharmaceutical lever that is actively neglected by clinicians, with a usage rate of only 6% in established cardiovascular disease cohorts.
Dual-therapy lipid lowering (statin + ezetimibe) is the most pragmatic, real-world pathway for patients to reach the <55 mg/dL target without requiring expensive injectable biologics.
High-intensity statin monotherapy often suffers from diminishing returns; adding ezetimibe provides severe synergistic LDL-C suppression with lower total toxicity risk.
Soluble dietary fiber, notably psyllium husk, exerts a modest, clinically validated cholesterol-lowering effect by binding bile acids in the gut, forcing hepatic cholesterol consumption.
III. Adversarial Claims & Evidence Table
Claim from Video
Speaker’s Evidence
Scientific Reality (Current Data)
Evidence Grade
Verdict
PCSK9 inhibition dramatically lowers LDL-C and prevents MACE in high-risk primary prevention (diabetics without known atherosclerosis).
VESALIUS-CV trial (subgroup analysis presented March 2026)
Verified. A 2026 subgroup analysis of the Phase 3 VESALIUS-CV trial demonstrated that evolocumab reduced 3-P MACE by 31% (HR 0.69) in high-risk diabetic patients without ASCVD. Marston et al., TCTMD 2026
Level B
Strong Support
Lowering LDL-C below 55 mg/dL is vastly superior to the 70 mg/dL target for secondary prevention.
ES PAVE trial (South Korea, 2026)
Source unverified in live search for full direct publication link, but trial data directly aligns with ACC 2026 abstracts detailing a 33% relative risk reduction in major events at the 55 mg/dL target.
Level B
Strong Support
Plaque formation strictly begins at an LDL-C threshold of approximately 50-60 mg/dL.
PESA Study (subgroup analysis)
Verified. Progression of Early Subclinical Atherosclerosis (PESA) study data indicates that subclinical atherosclerosis progression is rampant at conventional levels and ceases only when LDL is driven below the 50 mg/dL range. PESA Study, JACC
Level C
Plausible
Ezetimibe is cheap, effective, and severely underutilized (6% prescription rate).
Anecdotal / General cardiology statistics
Verified. A 2025 meta-analysis confirmed combination statin plus ezetimibe yields a 19% reduction in all-cause mortality over statin monotherapy, yet broad utilization remains clinically inadequate. Mayo Clinic Proceedings 2025 data
Verified. A 2025 dose-response meta-analysis confirms psyllium supplementation significantly decreases LDL-C (Weighted Mean Difference: -8.55 mg/dL). Genes & Nutrition, 2025
Level A
Plausible
IV. Actionable Protocol (Prioritized)
High Confidence Tier
Target the Biological Minimum: For individuals with established ASCVD or high-risk primary prevention profiles (e.g., diabetics, strong family history), target an LDL-C of <55 mg/dL rather than the conventional <70 mg/dL or <100 mg/dL.
Deploy Dual-Therapy Baselines: Implement generic Ezetimibe (10 mg) in tandem with maximally tolerated statin therapy. This circumvents hepatic upregulation of cholesterol absorption (a common resistance mechanism to statins) and allows patients to hit ultra-low LDL-C thresholds without incurring extreme biological or financial costs.
Early Biomarker Screening: Do not wait for cardiovascular events or calcium scores to dictate therapy. Assess ApoB or LDL-C profiles in early adulthood and intervene aggressively to prevent the initiation of the plaque-building cascade.
Experimental Tier
Soluble Fiber Supplementation: Introduce daily Psyllium Husk (5-10g) to achieve modest, dose-dependent reductions in LDL-C and improve gut motility. It possesses a high safety margin but is insufficient as a standalone monotherapy for high-risk patients.
Monitor Oral PCSK9 Inhibitors: Keep watch on Phase 3 clinical trials for orally bioavailable PCSK9 inhibitors. Once approved, these will eliminate the logistical barrier of subcutaneous injections, democratizing ultra-low LDL-C access.
Red Flag Zone
Complacency with “Normal” Ranges: Accepting an LDL-C of 100-130 mg/dL as “healthy” is biochemically flawed. This range passively permits the silent accrual of subclinical atherosclerosis over decades.
Monotherapy Maximalism: Pushing statins to extreme, high-toxicity doses before attempting a dual-pathway approach (adding ezetimibe) often increases myopathy and hepatotoxicity risk with severely diminishing returns on LDL-C reduction.
V. Technical Mechanism Breakdown
PCSK9 Inhibition (Proprotein Convertase Subtilisin/Kexin Type 9): PCSK9 is a hepatic protease that binds directly to the epidermal growth factor-like repeat A (EGF-A) domain of the low-density lipoprotein receptor (LDLR). This binding effectively flags the LDLR for lysosomal degradation rather than allowing it to be recycled back to the cell surface. By antagonizing PCSK9 (via monoclonal antibodies like evolocumab), LDLR density on the hepatocyte surface is massively preserved and upregulated, resulting in a profound acceleration of the clearance of circulating ApoB-containing lipoproteins.
NPC1L1 Inhibition (Niemann-Pick C1-Like 1): Ezetimibe localizes to the brush border of the small intestine and directly antagonizes the NPC1L1 sterol transporter. This severely blunts the intestinal absorption of both biliary and dietary cholesterol, reducing the delivery of intestinal cholesterol to the liver. The resulting hepatic intracellular cholesterol depletion forces the upregulation of LDLR expression to pull more cholesterol from the plasma. This mechanism operates highly synergistically with HMG-CoA reductase inhibitors (statins), which suppress endogenous hepatic cholesterol synthesis.
Atherogenesis Concentration Thresholds: Endothelial transcytosis of LDL particles and their subsequent retention and oxidation in the subendothelial intima initiates the inflammatory macrophage-foam cell cascade. The PESA and ES PAVE trial data imply that the pathogenic concentration gradient necessary to physically drive ApoB particles into the intima effectively neutralizes only when plasma LDL-C drops below the 50-60 mg/dL threshold. Above this level, the gradient favors intimal accumulation.
Statins + ezetimibe has been very effective for me. On august 2025, my LDL was 89mg/dL on 10mg rosuvastatin, 6 months later, my LDL is 27mg/dL on a combination of 10 mg rosuvastatin and 10mg ezetimibe.
I have been in the lower is better camp for a long time. Nice to see some justification
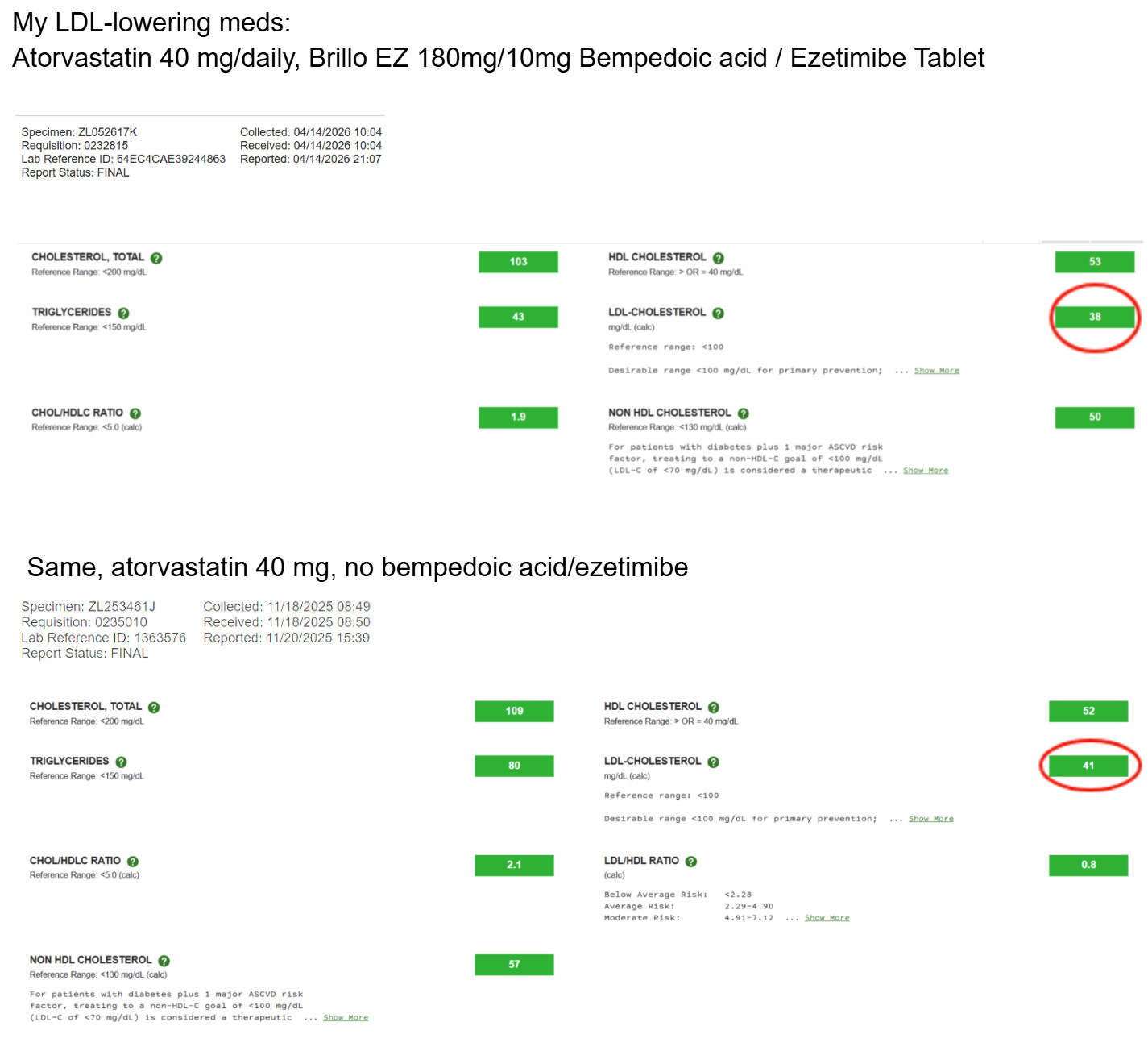
IMO: Body weight and exercise do lower LDL, but their effects are modest, and genetics typically dominates the picture for where someone’s LDL actually sits. I believe diet is secondary to these. (Except your diet must allow you to maintain a low BMI.) So take Brillo EZ first, and if that doesn’t do the trick, add a statin.
Unfortunately, I don’t have access to records going back to when I started on atorvastatin, which was decades ago. I stopped using Brillo EZ just because I ran out and forgot to order some more. I recently ordered some more Brillo EZ from India, and I will start taking it again.
Your doctor measures cholesterol. They don’t measure the molecule that drives most of the remaining risk for heart disease.
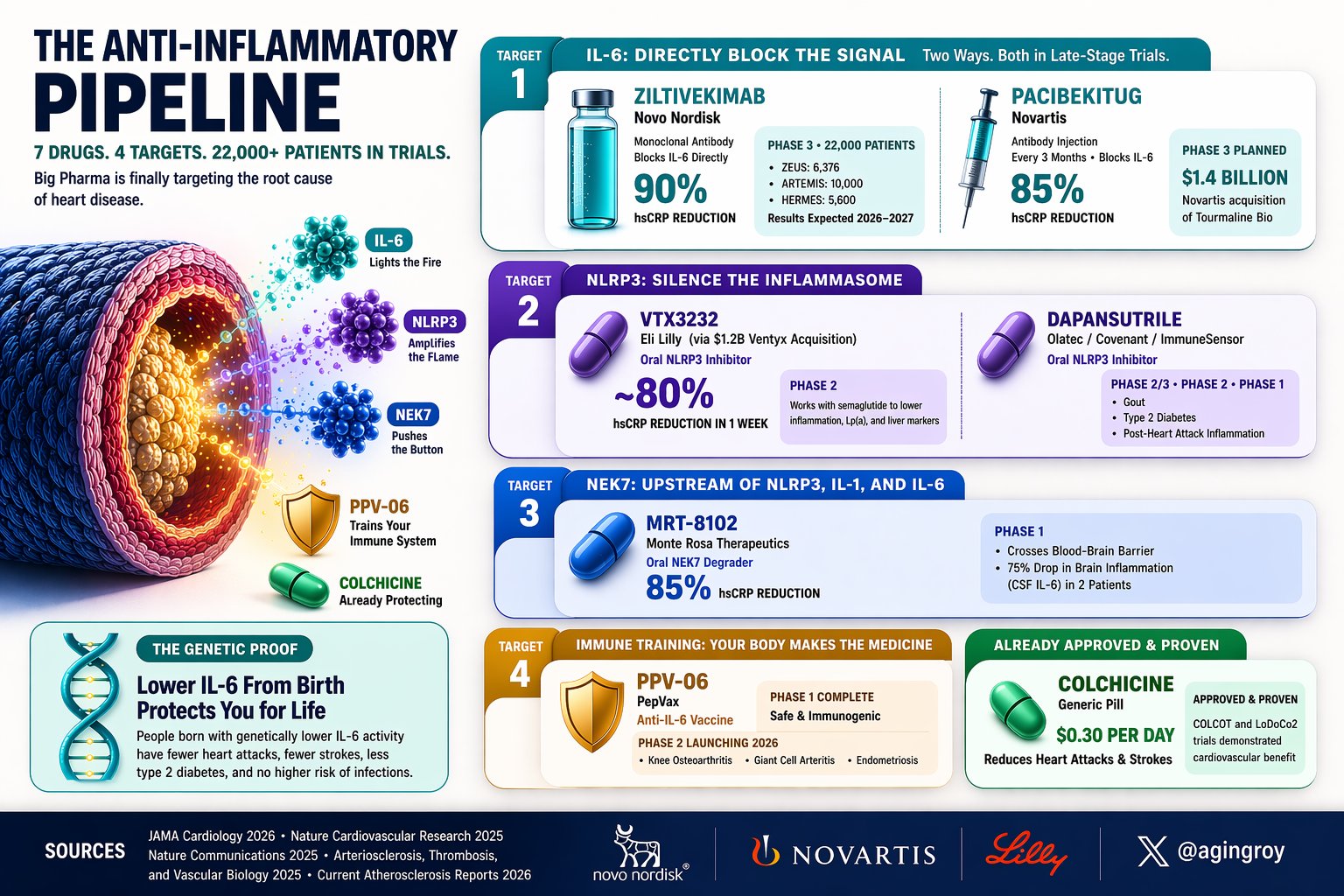
It’s called IL-6. It fuels chronic inflammation. For the first time, drugs targeting it are in massive trials. 7 programs. 4 biological targets. 22,000+ patients enrolled.
The injectable IL-6 blockers:
→ Ziltivekimab ([@novonordisk (https://x.com/novonordisk)) drops hsCRP by 90%. Three Phase 3 trials running (ZEUS, ARTEMIS, HERMES), 22,000 patients. Results 2026-2027.
→ Pacibekitug ( @Novartis , $1.4B Tourmaline acquisition) cuts hsCRP 85% with one shot every 3 months.
The oral pills:
→ VTX3232 ( @EliLillyandCo, $1.2B Ventyx acquisition) is an NLRP3 inhibitor. Reduced hsCRP ~80% in the first week. Combined with semaglutide, it beat GLP-1 drugs alone on inflammation and Lp(a).
→ MRT-8102 (@MonteRosaTx) degrades NEK7, upstream of the whole cascade. 85% hsCRP reduction. Crosses the blood-brain barrier, dropping brain inflammation 75% in two patients.
→ Dapansutrile: another NLRP3 inhibitor, Phase 2/3 for gout, diabetes, and post-MI inflammation. The wildcards:
→ PPV-06 isn’t a drug. It’s a vaccine that trains your immune system to make its own anti-IL6 antibodies.
Phase 2 launching 2026.
→ Colchicine: already approved, $0.30/day. Proven to reduce heart attacks (COLCOT, LoDoCo2). Most cardiologists still don’t prescribe it.
The genetic proof: Mendelian randomization (Nature Cardiovascular Research, 2025) shows people born with lower IL-6 have fewer heart attacks, fewer strokes, less diabetes. No increase in infections.
Your DNA running a lifelong clinical trial. The next risk factor your doctor will test isn’t cholesterol. It’s inflammation.