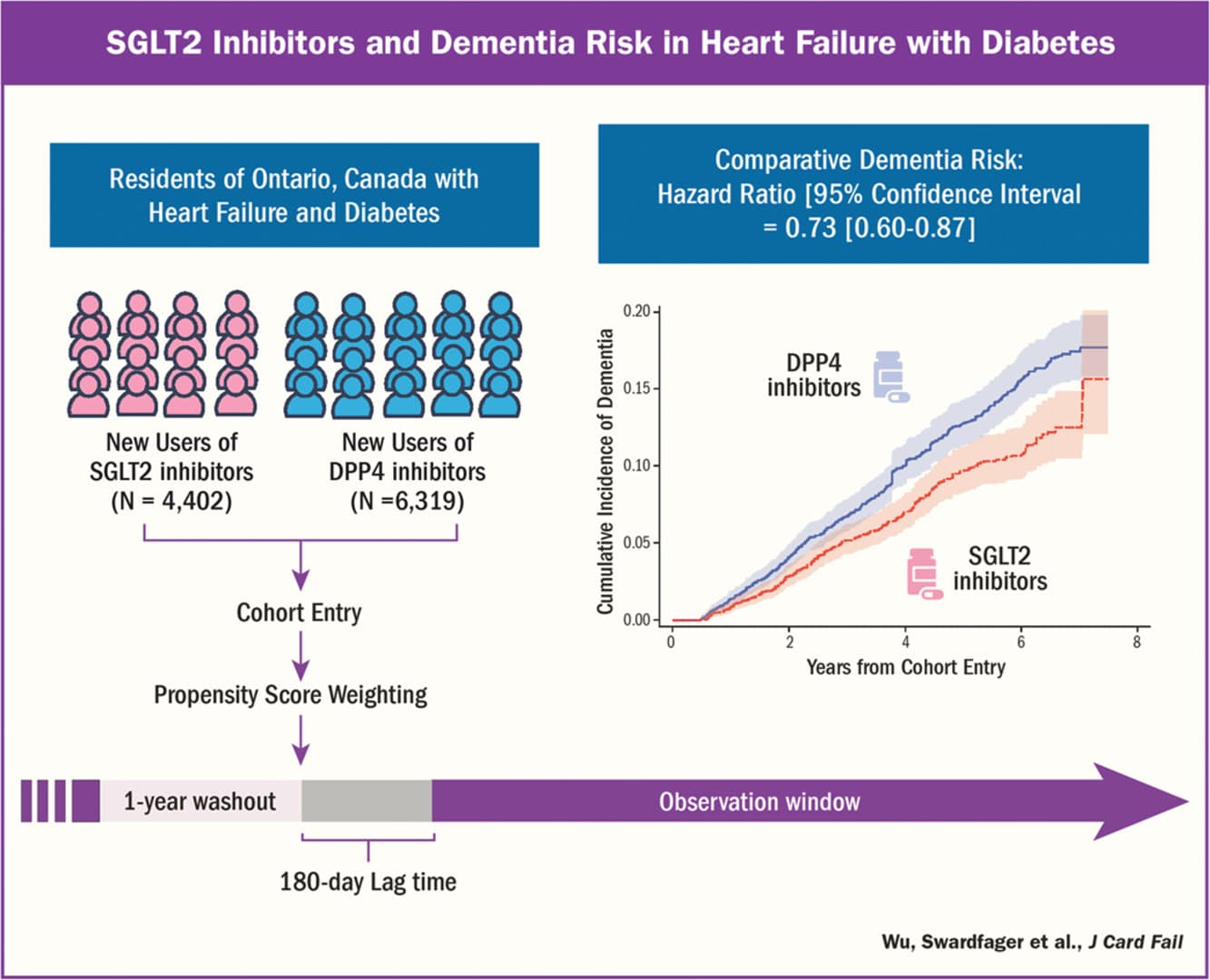
Findings: Over a mean follow-up of 3.04 years, SGLT2i use was associated with a significantly lower incidence of all-cause dementia (adjusted hazard ratio [aHR] 0.82, 95% CI 0.71–0.95) and unspecified dementia (aHR 0.75, 95% CI 0.62–0.90) compared with GLP-1 RA use. No statistically significant differences were observed for Alzheimer’s disease (aHR 0.96, 95% CI 0.73–1.26) or vascular dementia (aHR 0.77, 95% CI 0.53–1.12). Findings remained robust in competing risk analyses (aHR for all-cause dementia 0.84, 95% CI 0.73–0.98; unspecified dementia 0.77, 95% CI 0.64–0.93).
I’m pretty happy using both simultaneously for most individuals, unless there are contraindications. Also need to look at all cause mortality/morbidity and, if for example, a patient has a BMI of 35, I’d favor heavy on the GLP-1 as being the thing that will improve their outcomes the most, if their body weight is ideal, then the SGLT2-i would be favored.
I think the data looking at GLP-1’s and dementia vs. nothing looks good for benefit - it’s just the SGLT2-i has even more benefit.
Clearly there’s still a need for dedicated therapies and approaches for Alzheimer’s and vascular dementia. Taking care of CV health is likely helpful, but I keep thinking about Japan, where VD is at much higher comparative rate to AD as juxtaposed to the ratio in the West. And after all, Japan also has much lower rates of diabetes and CVD. Sure, these are epi statistics, but interesting nonetheless.
Just asking for advice as to wether to retry empagliflozin-have tried 2.5mg , 5mg //both just flattened me for 24hrs-no energy and peeing all the time. Is this something that goes away? I have never trued it for more than one day. I have 10mg tabs .
Your glucose levels are too low to keep up with your regular activity levels. That is something that your body could either get used to over a few months of using low dose empagliflozin or you need to deliberately eat more sugar.
Peeing all the time suggests to me that his glucose levels are quite high (thus lots of glucose being dumped and dragging water w/it into the urine). Someone with low glucose shouldn’t see much of an effect from an SGLT2I.
You need to get some bloodwork done before starting empagliflozin (or any drug). This is not a typical reaction. If a CGM works for you (tried repeatedly - it does not work for me) you might be interested to see how your blood glucose levels change with time of day/night, food intake, exercise - or use a glucose monitor (my current method). You need some baseline data before starting empagliflozin. Once you have that data you can monitor how empagliflozin impacts you and how it tracks with biomarkers.
So, I would start with getting baseline data: blood & urine tests, CGM (or glucose monitor) and only then start with a low dose empagliflozin 10mg/day and measure again.
I’m flattened by dapagliflozin, but don’t have the peeing all the time problem. I feel spacey and lightheaded. Eating sugar does not seem to help. Sometimes also get some sinus pain. I’ve tried a few times to no avail.
About to try a very low dose every other day to see if I can work up to it.
Currently I am taking a 100mg canagliflozin, but it seems like in this thread mostly are taking empagliflozin?
I’ve read some paper claim that canagliflozin shows better longevity result than empagliflozin
This reminds me of Bryan Johnson is trying empagliflozin though.
The present study found that sodium-glucose cotransporter 2 (SGLT2) inhibitor initiation was associated with a 27% lower dementia risk in heart failure with diabetes.
Have your weight dropped?
I’ve read some paper claim that SGLT2i may produce around 50-60 g of urinary glucose excretion per day. which is about 200 calories
If not, you might not be addressing the root cause based on your family history, and your personal fat threshold for causing type 2 diabates is lower than what you have currently.
If it’s an issue dieting on its own then a drug like wegovy (semaglutide) is a good idea for most.
You’re just addressing the symptoms, literally, with SGLT2 inhibitor.
Fantastic result, Chris, and very inspiring! I am 8 months into my empagliflozin journey - 3 months on 25mg/day - and Friday I’m again having a huge batch of blood tests done, so I’m curious to find out what my A1c and insulin will show. But I’ll keep you in mind as I keep taking the empa hoping for a similar result!
You’re treating (pre)diabetes not preventing it, it’s less effective, and it’s not going to last forever, rather than addressing the possible root cause.
People are sensitive about excess body fat (I shouldn’t maybe say that though).
That’s where wegovy (semaglutide) comes into the picture, only way reduce stigma of such things is to smash right through the stigma, or maybe not. Why don’t you take it?