chatgpt might help in the case
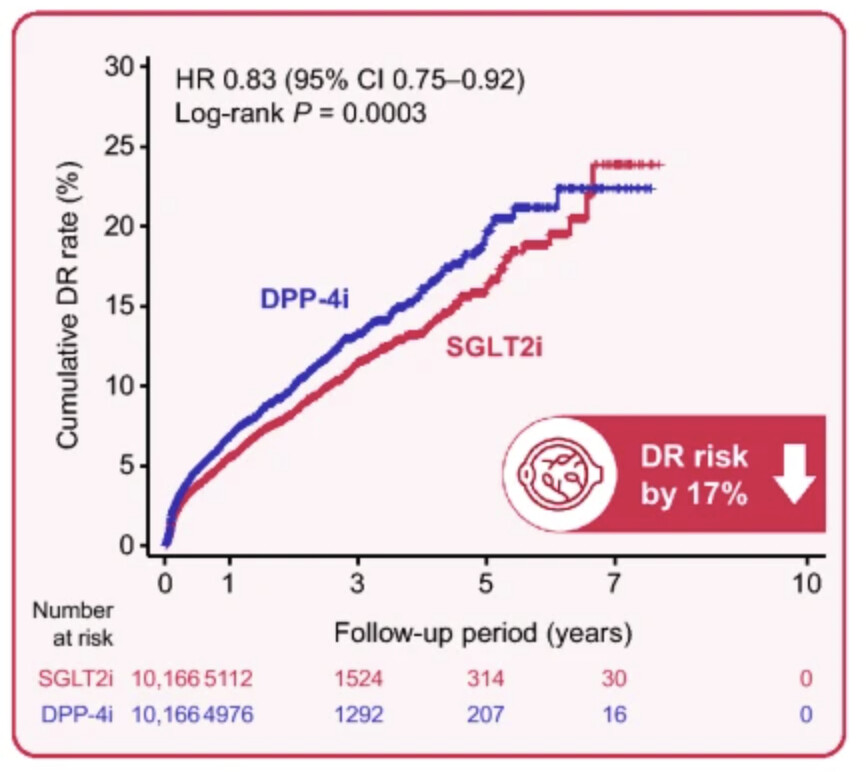
The IR of DR diagnosis was 46.23 and 57.12 per 1000 person-years in the SGLT2i and DPP-4i groups, respectively, with a significantly lower risk in the SGLT2i group than in the DPP-4i group (HR 0.83, 95% CI 0.75–0.92, P = 0.0003).
Pakistani article (not of the highest quality, FWIW…): Relationship between SGLT2 inhibitor use and specific cancer types: a systematic review and meta-analysis 2024
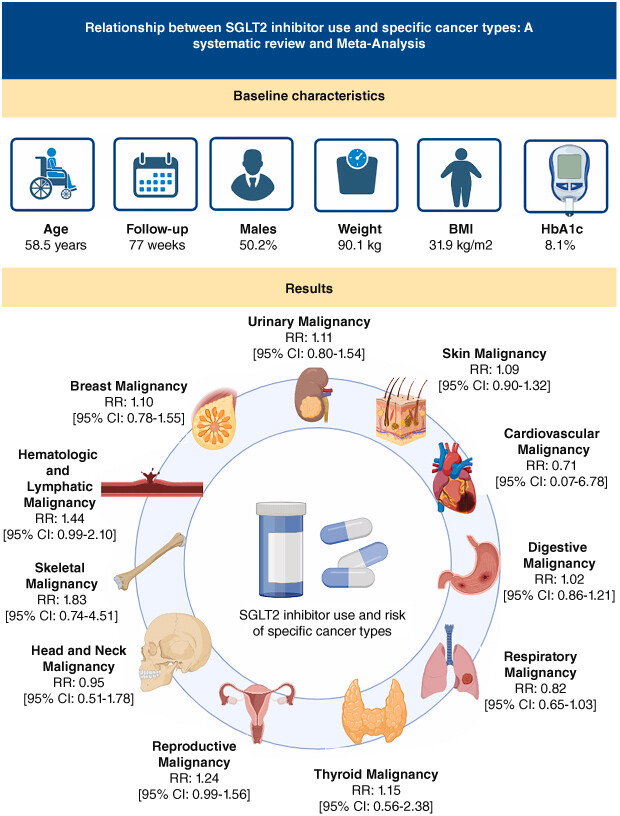
(nothing statistically significant)
5 Likes
There’s a Discours AI Summarize plugin that allows you to summarize a whole thread: Discourse AI - Summarize - Site Management - Discourse Meta (poke @RapAdmin ) However, it has a cost…
8 Likes
Its in the plans - but we have other custom plugins that are not supported on newer updates of discourse - so its complex… but at some point, yes, we’ll implement it.
2 Likes
This increase in Iron may be fine for diabetics, but perhaps not so good for healthy people taking canagliflozin for longevity:
I don’t think so:
Koshino and colleagues found canagliflozin was associated with a 2.1% increase in total iron-binding capacity (95% CI, 0.4-3.8) and an 11.5% decrease in ferritin (95% CI, 7.1-15.7), without affecting serum iron or transferrin saturation.
So canagliflozin (and all SGLT2i) improves iron metabolism.
5 Likes
Is it all SGLT2i class effect, or cana specific (I’m thinking that cana is different insofar as partially affecting SGLT1 inhibition).
1 Like
![]() (and 20 characters)
(and 20 characters)
2 Likes
There is this warning about empa:
“Ketoacidosis can also happen in people who: are sick, cannot eat or drink as usual, skip meals, are on a diet high in fat and low in carbohydrates (ketogenic diet), take less than the usual amount of insulin or miss insulin doses, drink too much alcohol, have a loss of too much fluid from the body (volume depletion), or who have surgery.”
I’m curious, do folks that take SGLT2 inhibitors here worry at all about this?
I wonder if this only applies to keto diet or if people who eat a lower carb but not keto diet (for example, ~130g of carbs per day = or about 0.75g per pound of bodyweight) and fast for ~13-14 hours (early dinners) should also take any precautions.
For example, do you ensure you eat a minimum amount of carbs (or did you increase the amount), check your ketones periodically, or watch out for any symptoms?
2 Likes
I think taking an SGLT2 inhibitor when you are on a Keto diet would be redundant; your blood sugar level is not going to be spiking like it would on a more carb-oriented diet, so why would you take an SGLT2 inhibitor? That would seem to make no sense.
I have a vegetable-heavy diet with lots of fish. I’m healthy metabolically, exercise 4 to 6 hours a week, and I have had no concerns about (or issues with) either Ketoacidosis, or UTIs (which are more common). I don’t worry about these potential issues.
2 Likes
I’m less interested in keto diets (typically <30g carbs per day) as I don’t follow one, but in whether similar precautions would apply to people who eat a relatively low carb diet (let’s say ~130g carbs per day) and have early dinners (resulting in 13-14 hour fasting periods).
(see the note about “skipping meals” in the empa warning)
While eating this amount of carbs, I often see 0.2 ketones (without taking SGLT2 inhibitors and without intentionally trying to get into ketosis). I train 7+ hours a week.
1 Like
I’ve been battling the data on Empa vs. Cana. the past couple weeks. Beyond glucose control, CV and preventive kidney protection- cancer prevention and generalized, degenerative autoimmune attacks may be a bigger fish to fry, only when comparing to “superior” kidney protection between the two.
My concern is the clinically significant inhibiting of mitochondrial complex 1 with canagliflozin; which is hosting the cancer and autoimmune benefits will also decrease quality of life and increase some risks having an additive effect on mitochondrial dysfunction.
The generalized autoimmune effects are of a particular interest as it is a direct cause of various diseases. Empa does not inhibit complex 1 of the mitochondria so I’m not confident we’d see equal outcomes that were produced with the ITP.
I may start a thread in regards to get some inisight from others in the field.
7 Likes
My diet is 50% carbs, I don’t worry at all.
1 Like
@adssx any thoughts on this? It does seem like Empa (and Dapa) may not affect complex 1 in the same way as Cana?
Based on this, I plan to continue taking Empa until I get a cancer diagnosis, then switch to Cana. I plan to get an annual whole body MRI scan (SimonOne for $650 for cancer only scan, $1250 with MRA and NeuroQuant and higher-res Prostate/Ovarian cancer scan SimonOne Pricing) so I get early warning.
3 Likes
In theory that would seem to make some sense:
3 Likes
I have no idea sorry.
1 Like
No, I came to this website as this is the place to do it. Empa and other SGLT2 do not share the same direct effect on complex-1. It’s an independent and personal hypothesis that I’ve been thinking about the past 18 months. My business is seasonal, I’ve just finished up so I have time to review the data.
Mitochondrial Respiratory Complex I is a target for specific types of cancer research and it looks promising. Empa and other SGLT2 inhibitors targets AMPK, and cancer outcomes are less impressive to say the least. To note, canagliflozin targets AMPK at a significantly higher level- It will be a no brainer when I specify the mechanism- inhibiting mitochondrial function, complex 1. As we all know, mice are vulnerable and prone to cancer; humans having much more complex systems than mice so far from equal models for ITP outcomes, but the cancer specific outcomes in humans are measurable.
Beyond, autoimmune targets for age-related, generalized autoimmunity is of interest as we currently cannot target the aging immune system in all its complexity- increasing immune responses is a problem leading to many diseases- presently, canagliflozin but not other SGLT2 inhibitors have shown to target adaptive related modulating effects rather than suppressing.
Empa has numerous benefits for mitochondrial function and metabolic functions increasing ATP etc. which are primary reasons for its efficacy in HF. Numerous other targets of course.
We have been blindly taking Empa for aging indication based on the fact that it has more promising data in humans for numerous drug indications, which in some context “aging is the sum of all diseases” but fundamentally I question it’s efficacy compared to Cana for aging indication. It looks like Cana can meet primary end-points for some adaptive related autoimmunity downstream >mTOR1 and the cancer target of complex 1 while benefiting CV, CKD and HF but not to the degree of Empa.
We know that preventive measure is the best measure and I think that’s what cana can provide, possibly more than other molecules in the class. That’s my hypothetical Interpretation as how it can increase healthspan.
@RapAdmin Would you like to start a thread on this and move this over? I’m failing to discuss various other details that are involved and many could benefit from the discussion.
4 Likes
Empa’s benefits have been clinically proven.
Canagliflozin’s impact on cancer and autoimmune regulation is so far only a hypothesis underlined by some ex vivo cell tests. It is not even clear if clinical relevant concentrations could be achieved in the T-cells in vivo for example.
I will happily switch to Canagliflozin if the hypothesis turns out to be true, but so far I will stick to Empa.
Or maybe I will take both alternatively then.
6 Likes