Is there anything unique about henagliflozin compared to all the others?
1 Like
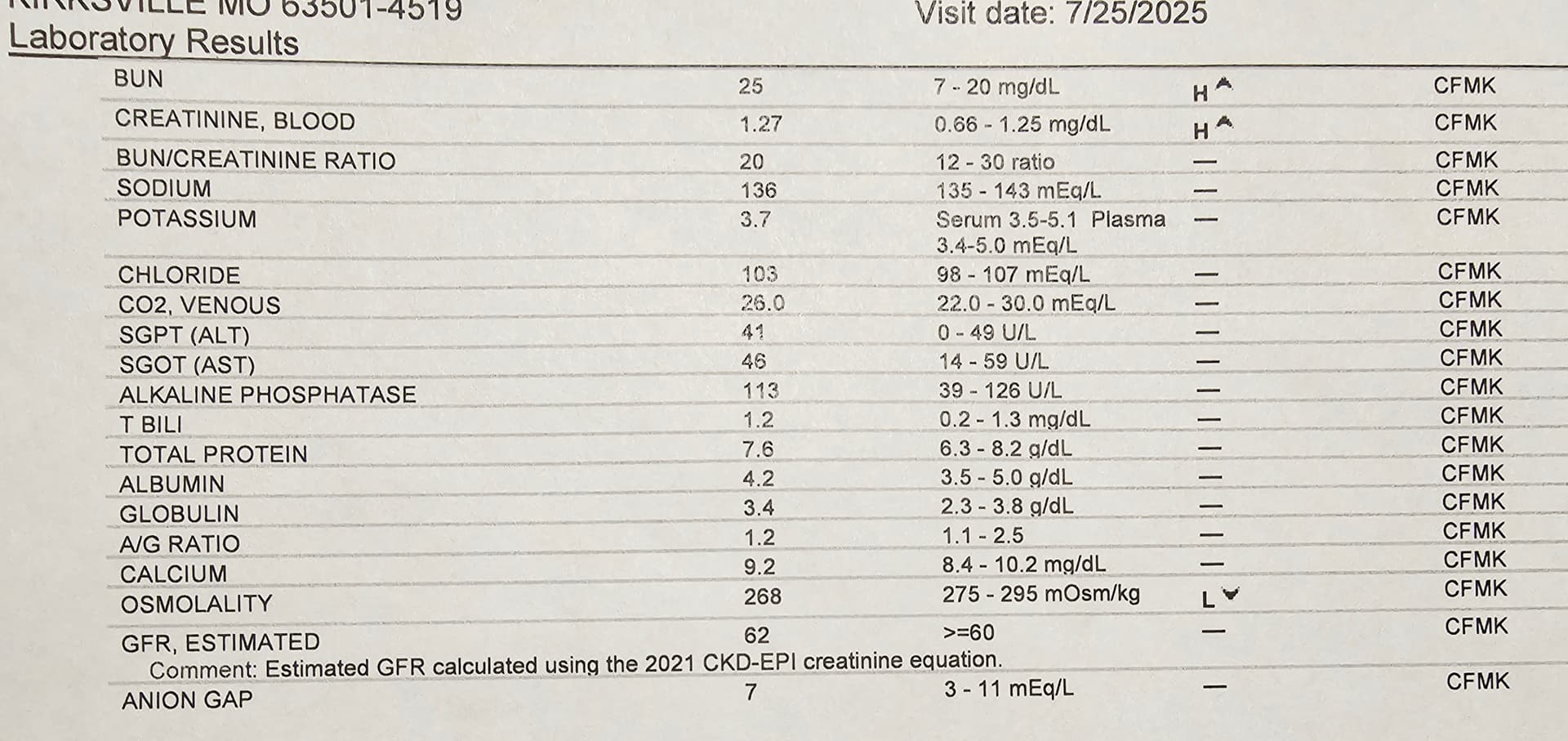
Based on the discussions, research and reports I found here on SGLT2i inhibitors for longevity, I was curious to give it a try… and consulted with my personal physician. He agreed it definitely could be helpful… my GFR at 62 at my end of July blood work… is just passable, maybe a SGLT2i could push me up.
Was totally gung-ho… but had sticker shock on Jardiance self pay about $900 per month. ![]()
My physician filed with my health insurance for kidney health. They approved with a co-pay of $60 per month. Much better. My pharmacist said Jardiance has a helping site for a discount to just co-pay $10 per refill. A few questions… nothing really medical. Odd. I got the discount. From $900 monthly to $10 monthly. Crazy.
If you can get your physician to sign off… even if insurance won’t cover it all. Go to this link for $10 co-pay: https://patient.boehringer-ingelheim.com/us/products/jardiance/type-2-diabetes/savings
Jardiance is the brand name for the prescription drug empagliflozin, an oral medication used to treat type 2 diabetes, heart failure, and chronic kidney disease in adults. It is part of a class of drugs known as sodium-glucose cotransporter 2 (SGLT2) inhibitors.
How Jardiance works
Jardiance works by targeting the SGLT2 proteins in the kidneys. SGLT2 is responsible for reabsorbing glucose (sugar) from the urine back into the bloodstream. By blocking this protein, Jardiance increases the amount of glucose that is excreted in the urine, which helps lower blood sugar levels. This process can also lead to modest weight loss.
I have been on Jardiance for a few weeks… no issues… I seem to pee just a bit more often… that’s it.
I am looking forward to seeing my GFR score in 6 months
7 Likes
Here is an ai summary
Here’s your updated table, now including henagliflozin (SHR-3824), with all key molecular target metrics aligned in one place:
| Drug | Primary target(s) | SGLT2 IC₅₀ (nM) | SGLT1 IC₅₀ (nM) | Selectivity (SGLT2 over SGLT1) | Notable notes / secondary targets |
|---|---|---|---|---|---|
| Canagliflozin | SGLT2 » SGLT1 | 4.4 | 684 | ~155× | More SGLT1 cross-inhibition; also inhibits SGLT6. |
| Dapagliflozin | SGLT2 » SGLT1 | 1.6 | 803 | ~502× | Highly selective; minimal SGLT1 inhibition clinically. |
| Empagliflozin | SGLT2 » SGLT1 | 3.1 | 8,300 | ~2,680× | Among the most SGLT2-selective. |
| Ertugliflozin | SGLT2 » SGLT1 | 0.877 | 1,960 | ~2,235× | Very potent and highly selective. |
| Bexagliflozin | SGLT2 » SGLT1 | 2.3 | 5,600 | ~2,435× | Highly selective. |
| Ipragliflozin (JP) | SGLT2 » SGLT1 | 7.38 | 1,876 | ~254× | Moderate selectivity. |
| Luseogliflozin (JP) | SGLT2 » SGLT1 | 2.26 | ~3,990 | ~1,765× | ~1,770-fold selectivity reported. |
| Tofogliflozin (JP) | SGLT2 » SGLT1 | 2.9 | 8,444 | ~2,912× | Strong human and rat selectivity. |
| Remogliflozin etabonate (IN) | SGLT2 » SGLT1 | ~14 | ~1,100 | ~79× | Least selective; also inhibits SGLT5. |
| Sotagliflozin (dual) | SGLT2 & SGLT1 | 1.8 | 36 | ~20× | Intentionally dual-action; gut SGLT1 inhibition prominent. |
| Henagliflozin (CN) | SGLT2 » SGLT1 | 2.38 | 4,324 | ~1,818× | Highly selective; ≥800-fold SGLT2 vs SGLT1 selectivity reported. |
Notes on Henagliflozin
- Origin & Approval: Henagliflozin (SHR-3824) is developed in China and approved there for treating type 2 diabetes.
- Selectivity: In vitro data indicate IC₅₀ ≈ 2.38 nM (SGLT2) and ≈ 4,324 nM (SGLT1), yielding a selectivity ratio of roughly 1,800-fold. Some reports simplify this as “≥ 800-fold” selectivity.
Summary Insights
- Most SGLT2-selective: Empagliflozin, ertugliflozin, bexagliflozin, tofogliflozin—all showing high selectivity (≥ ~2,200×).
- Henagliflozin fits strongly into this high-selectivity group (~1,800×), similar to luseogliflozin (~1,700×).
- Lower selectivity: Canagliflozin and remogliflozin have much less SGLT1 selectivity, which may influence GI glucose absorption and side effect profiles.
- Dual SGLT1/2 blocker: Sotagliflozin (~20×) intentionally targets both transporters—and is the least selective in the list.
Let me know if you’d like more detail on secondary targets, assay methodologies, or how these differences impact pharmacodynamics or clinical outcomes like heart failure or renal protection.
4 Likes
Did you ever get your cystatin C checked? If not, you are probably worrying about your GFR for no reason. If you take creatine monohydrate and lift weights, your creatinine-based GFR is going to be falsely decreased. Cystatin C should give you a much better GFR estimate.
That being said, IMO Jardiance is great to add to a longevity/health stack IF your hematocrit doesn’t get too high. Testosterone and SGLT2i both raise hematocrit, also GH and GH-releasing peptides can raise it as well.
8 Likes
I threw my blood test results (pdf) into ChatGPT and asked it to compare my blood levels with what are considered “optimal levels” based on Peter Attia’s medicine 3.0 standards. Very interesting results. I encourage others to do the same.
Your eGFR is low according to Attia:
Renal Function
- eGFR: 67 mL/min/1.73 m² — While “normal” is >59, Attia’s optimal is ≥ 90 for healthy adults without kidney disease.
3 Likes
Periodic reminder that labcorp cystatin c is garbage, get tested at quest.
3 Likes
I’ve switched all my blood work from LabCorp to Quest. At least in my area, the difference in service is night and day better w/Quest. LabCorp is overbooked, understaffed, and getting my results is like pulling teeth. Quest automatically releases each test result as it comes in, whereas LabCorp waits until ALL results have come in before releasing anything unless you go to their website and request special permission EVERY TIME to get “preliminary results”. ![]()
4 Likes
Considerations when choosing an SGLT2 inhibitor:
for day-to-day glucose control, dual SGLT1/2 (e.g., sotagliflozin) hasn’t proven superior to highly selective SGLT2 inhibitors on A1c, though it does blunt post-meal spikes more. Here’s what the evidence shows:
- A1c lowering with SGLT2 inhibitors (class effect): Meta-analyses of approved SGLT2i show mean A1c drops ≈0.5–0.7% vs placebo; small differences among individual drugs, with canagliflozin 300 mg sometimes ranking slightly higher, but clinical differences are modest. PubMedPMC
- Dual SGLT1/2 vs selective SGLT2 (head-to-head): In a randomized, double-blind trial (8 weeks) directly comparing sotagliflozin (SGLT1/2) vs empagliflozin (SGLT2-selective), overall glycemic control was comparable; the dual inhibitor reduced breakfast post-prandial glucose and insulin more (consistent with intestinal SGLT1 blockade), but this effect waned later in the day. PMC
- Mechanism for the post-prandial benefit: Human studies show SGLT1 inhibition delays intestinal glucose absorption, lowers post-meal glucose and insulin, reduces GIP, and raises GLP-1, explaining the breakfast spike blunting seen with sotagliflozin. PMCPubMed
- Any proof that SGLT1 adds more A1c reduction? Not convincingly. Reviews and meta-analyses of sotagliflozin emphasize cardiorenal outcomes; on glycemia, A1c benefits look similar to SGLT2-only agents, with the extra benefit mainly in post-prandial excursions, not a clearly larger A1c drop. PMC
- Safety nuance: Because SGLT1 is intestinal, dual inhibition more often causes GI effects (e.g., diarrhea) than SGLT2-selective drugs, although most events are mild. New England Journal of Medicine
Practical takeaway
If your goal is lower A1c, either approach works similarly on average. If a patient’s main problem is post-meal spikes(high PPG despite reasonable fasting readings), a dual SGLT1/2 agent may offer an added PPG benefit—but not necessarily a bigger A1c reduction—and with a bit more GI side-effect risk.
8 Likes
I take 5 g of creatine monohydrate daily and my egfr has not fallen much. It’s at 108. Cystatin C is 0.85. Both are great.
I also take 12.5 mg of empagliflozin daily as I want to keep my kidneys in great shape going forward.
Many people think about taking a flozin when their kidneys are in trouble. That’s like not changing the oil in your car until you hear clunking noises from the engine.
I’m taking empagliflozin proactively to keep my kidneys in top condition. It’s like changing the oil every 3 months. It may be a little too much, but I’m not going to freeze up my engine.
9 Likes
How is the pricing on quest? I’m moderately satisfied with labcorps, because in my area they seem to have more tests, and they are cheaper. I also use fitomics, which has just started adding more tests to choose from.
You’re right David…I am doing 10 mg creatine. 5 mg morning… 5 mg more end of day before gym workout.
Doing weekly 200 mg 1 ml cypionate too.
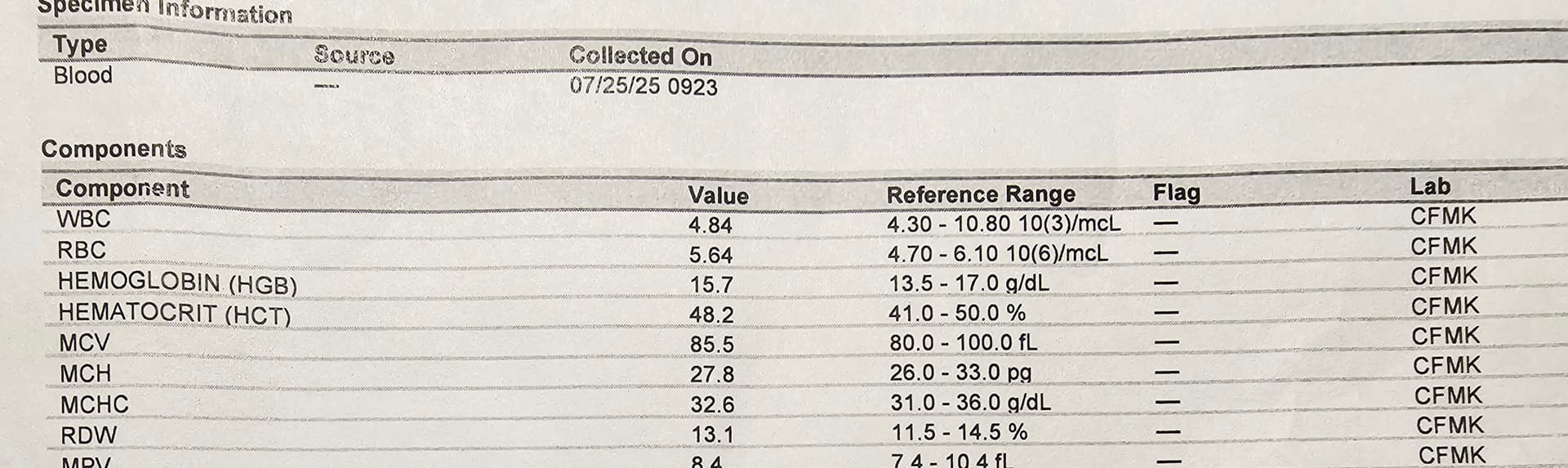
My Hematocrit is good- last blood test 48.2 high normal. I will keep an eye on it now that I am using an SGLT2 inhibitor.
2 Likes
I’m doing Fitomics as well. I haven’t really gone and compared the prices between Quest and LabCorp directly, but either way I’m sticking w/Quest due to the factors I mentioned above.
2 Likes
Really not sure what makes Henagliflozin special. From what I can see it’s a typical “me too” drug, but of course, I might have missed something. Approved in China and not many other places doesn’t make me enthusiastic unless there’s some independent studies outside of China. But it seems fairly new, so probably not many studies. Not sure why we should be excited over it, but hey, the more the merrier, options are always good.
5 Likes
The effect is probably not limited to henagliflozin. So that’s good news for all SGLT2i users.
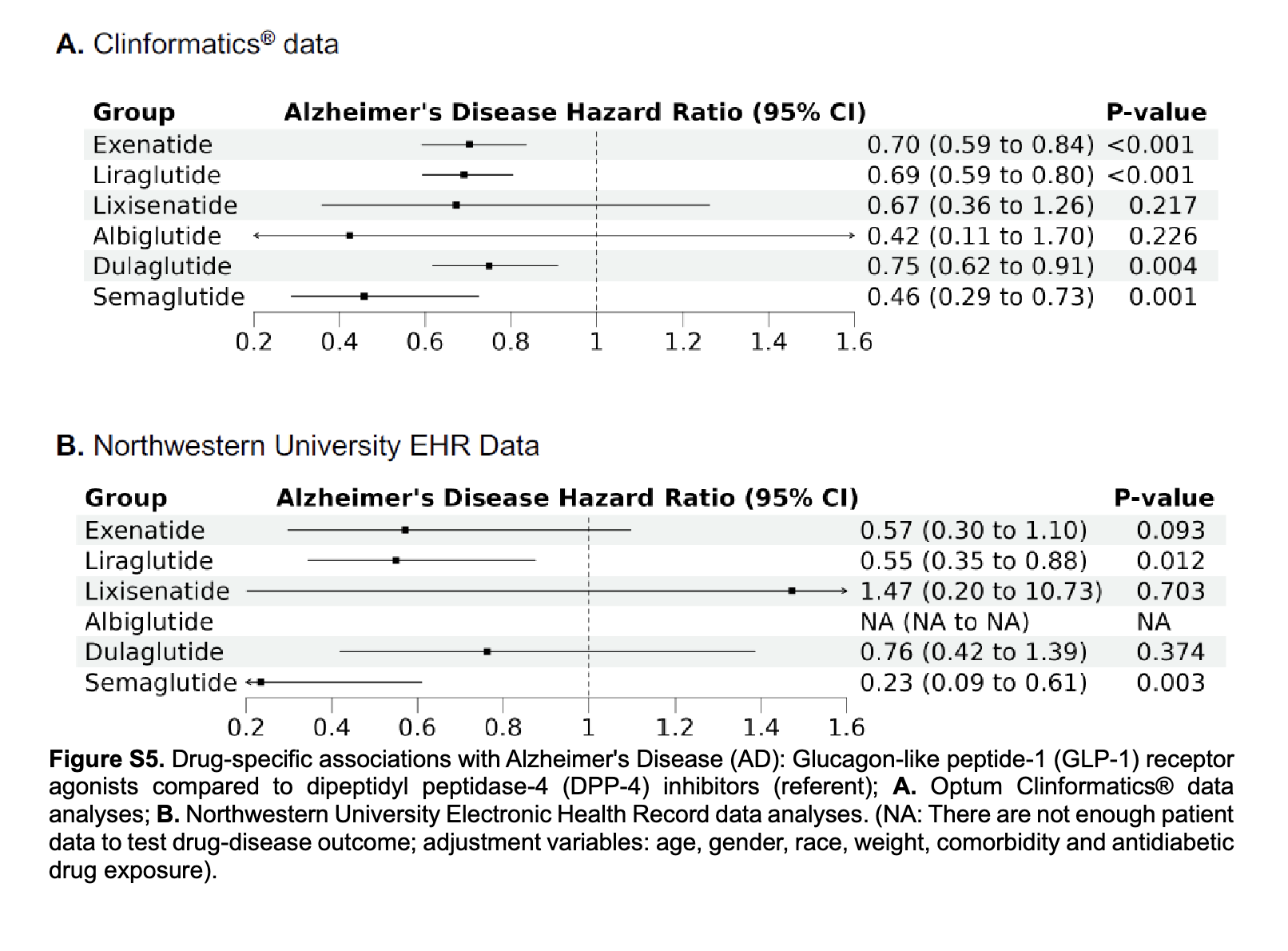
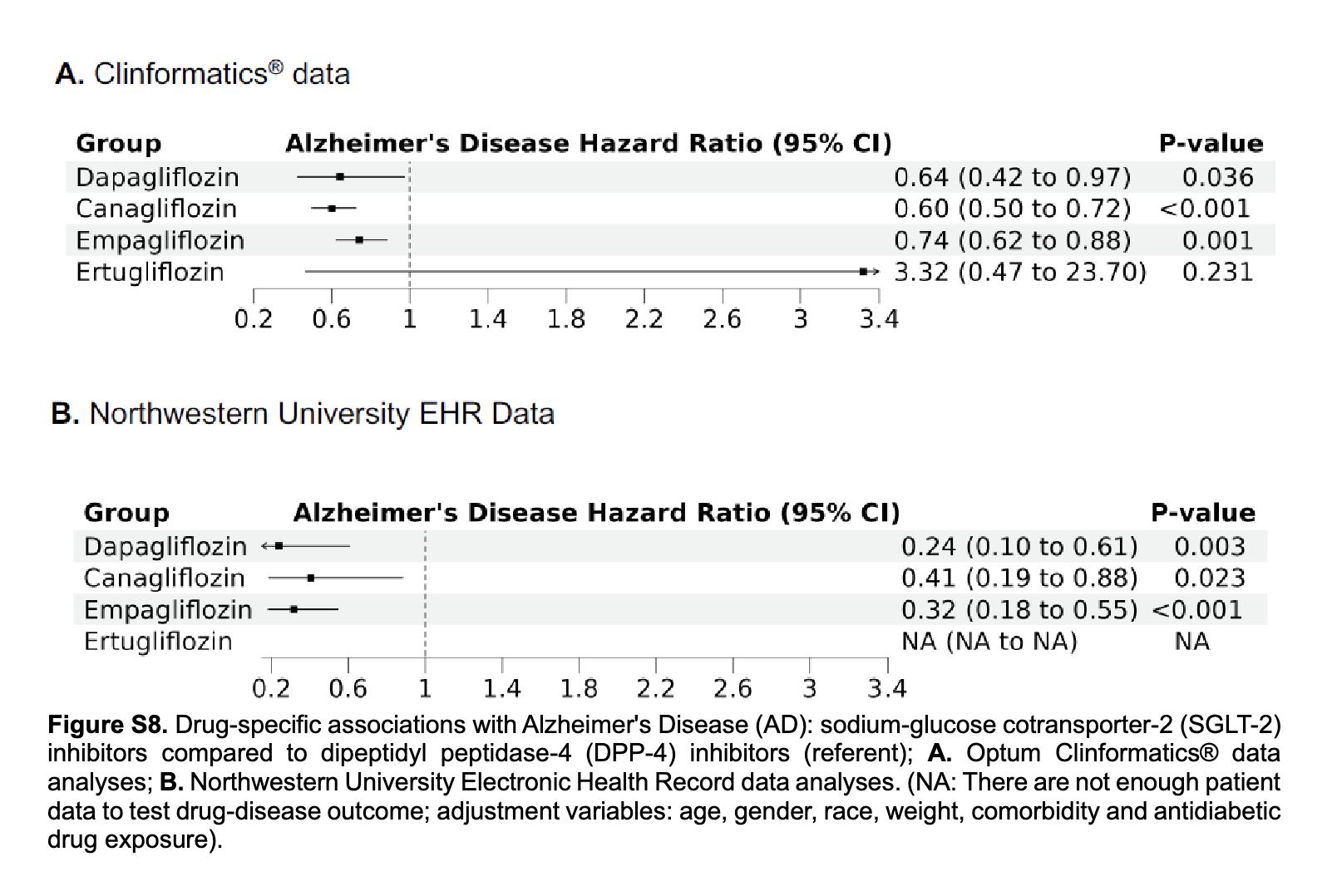
We identified GLP-1 receptor agonist initiation compared to DPP-4 inhibitors initiation was associated with a reduced risk of AD (hazard ratio [HR] ≤ 0.69 and P value < 0.001) and SGLT-2 inhibitor initiation compared to DPP-4 inhibitor initiation was associated with a reduced risk of AD (HR ≤ 0.67 and P value < 0.001).
Two GLP-1 receptor agonists (liraglutide and semaglutide) and three SGLT-2 inhibitors (dapagliflozin, canagliflozin, and empagliflozin) are associated with a reduced risk of AD in drug-specific sensitivity analyses.
6 Likes
I’ve switched all my blood work from LabCorp to Quest. At least in my area, the difference in service is night and day better w/Quest. LabCorp is overbooked, understaffed, and getting my results is like pulling teeth. Quest automatically releases each test result as it comes in, whereas LabCorp waits until ALL results have come in before releasing anything unless you go to their website and request special permission EVERY TIME to get “preliminary results”.
I recently used Quest (through Ulta) for the first time and that was my experience as well. Ulta also offers a greater variety of tests and at better prices compared to Marek
7 Likes
Semaglutide is looking good, but what the heck is going on with ertugliflozin, some kind of artifact(?) - wide CI bars.
And from the paper:
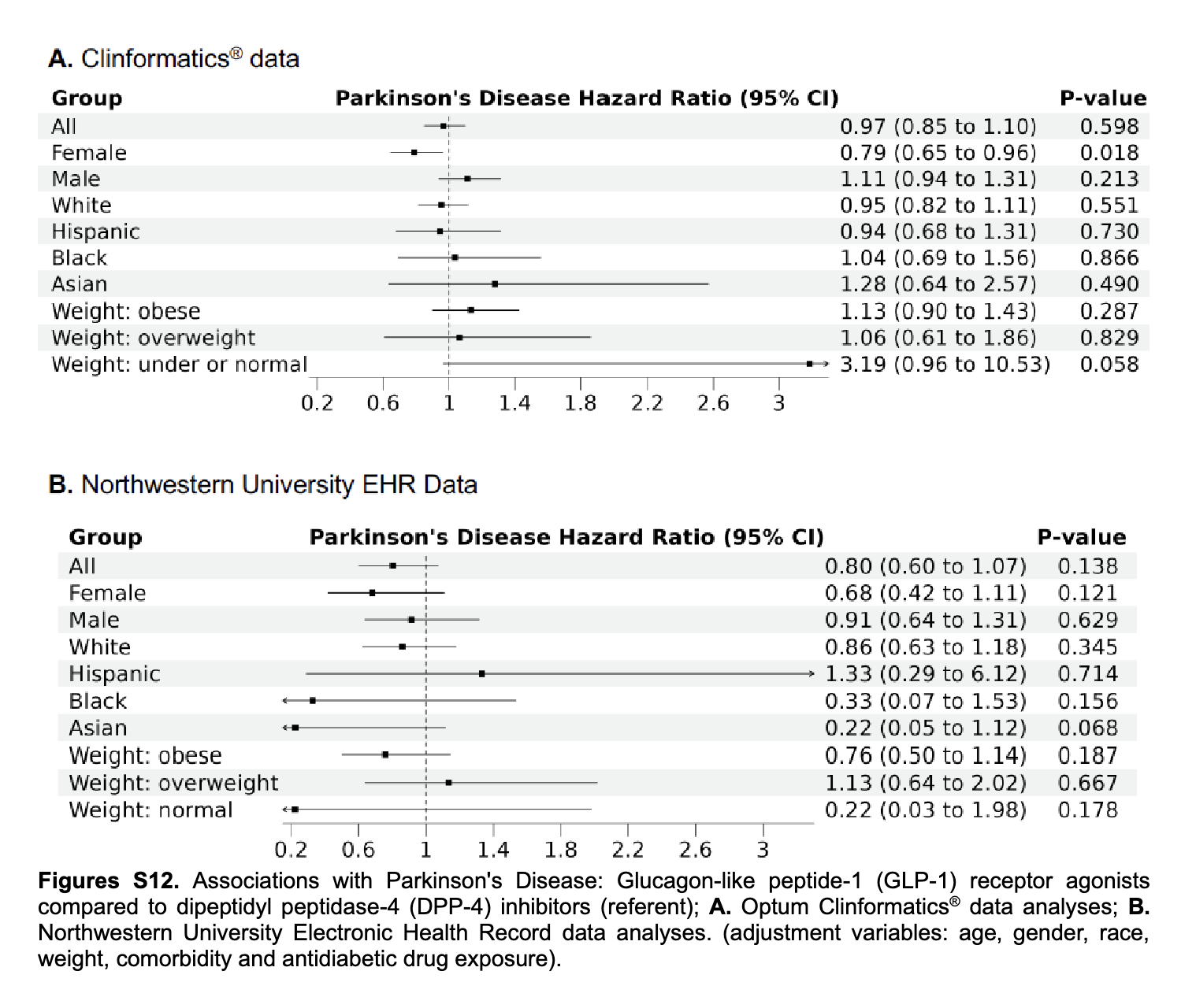
“The effects of GLP-1 receptor agonists, SGLT-2 inhibitors, and DPP-4 inhibitors in AD and PD remain inconclusive in subgroups.”
What subgroups are they talking about wrt. PD?
Also looking at Fig. 3A, in “under or normal weight” SGLT2 was not protective for AD (in contrast to 3B), though wide CI bars, maybe the difference between 3A and 3B is the inclusion of “under” in 3A (Clinformatics).
Let’s keep in mind, these were older cohorts, understandably for AD (prevalence), but a pity no younger cohorts for PD. Also generally disappointing for PD.
1 Like
Subgroups are for AD and PD. I assume they meant “obese”, “diabetic”, “young”, “old”, etc.
3.4 Other results
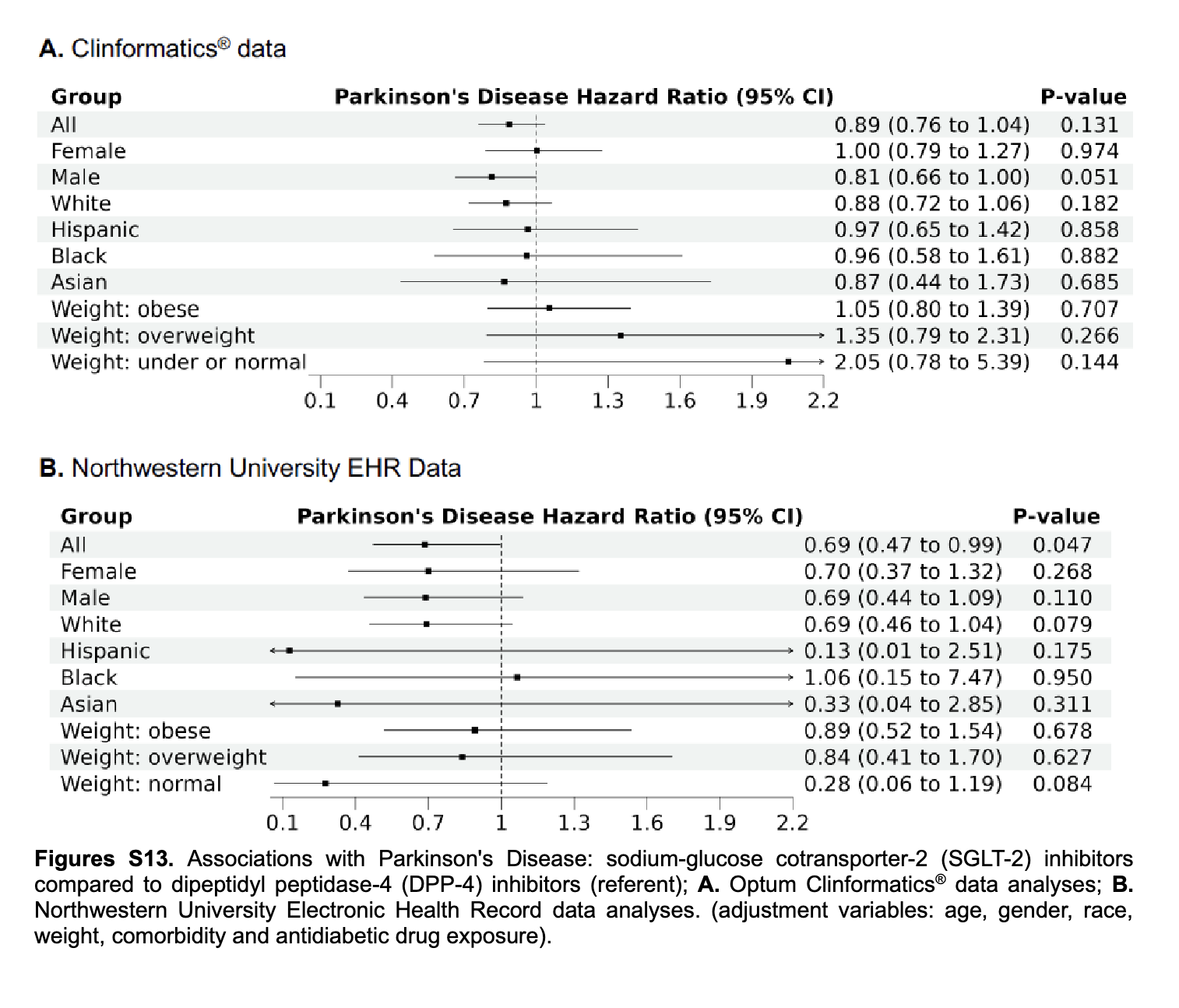
For PD, no consistent differences were observed in all comparisons (GLP-1 receptor agonist vs. DPP-4 inhibitors, SGLT-2 inhibitors vs. DPP-4 inhibitors, and GLP-1 receptor agonists vs. SGLT-2 inhibitors; Figures S12–S15 in supporting information). Full results of Cox models in overall analyses of Clinformatics data are presented in Tables S5–S7 in supporting information.
SGLT2 actually look quite good (0.69 [0.47–0.99], p=0.047 in “all”, might be even better in normal weight white males?):
2 Likes
Dapagliflozin effect on anemia outcomes in patients with diabetes and CKD 2025
Dapagliflozin was associated with significant improvements in hemoglobin levels and anemia correction in patients with T2DM and CKD. However, an increased risk of IDA, particularly in female patients, warrants careful monitoring. The protective effects of dapagliflozin against ESA initiation highlight its potential role in anemia management. However, due to the observational design, causality cannot be definitively inferred.
Both SGLT2Is were associated with highly significant improvement in kidney function as well as IIEF-5 (P < 0.001 in all).
6 Likes
This. Just like ApoB and GGT, Cystatin-C shoulder be on all standard lab tests. Maybe in 20 years.
0.85 is good. No need to worry about numbers like eGFR with a Cystatin-C like this. EGFR fluctuates by 10-20 for me depending on the lab draw but my Cystatin C is 0.64 so I know it’s most likely hydration related if I’m seeing screwy eGFR or BUN/Creatinine numbers.
I also love proactive approach. I use it more with cardiovascular prevention in mind since I know my kidneys are in good shape.
3 Likes
Fasting insulin too!