My goal is to maintain BG in a normal healthy range without SGLT2 inhibitors or Metformin only through diet and lifestyle. So far so good.
1 Like
Some people report elevation of blood lipids with SGLT2i. Perhaps tofogliflozin might be of interest in this context.
Tofogliflozin long-term effects on atherosclerosis progression and major clinical parameters in patients with type 2 diabetes mellitus lacking a history of cardiovascular disease: a 2-year extension study of the UTOPIA trial
“Tofogliflozin is an SGLT2 inhibitor with high selectivity for SGLT2. Suzuki et al. measured the sodium-dependent glucose uptake in SGLT2-overexpressing cells and evaluated SGLT2 selectivity against SGLT1, expressed as the ratio of inhibitory concentration 50 (IC50) for each compound. Their study showed that tofogliflozin (2900-fold) was highly selective compared to dapagliflozin (610-fold), canagliflozin (290-fold), ipragliflozin (860-fold), empagliflozin (1100-fold), and luseogliflozin (1600-fold) [8]. Tofogliflozin also has a short elimination half-life (5–6 h) with a high level of urinary excretion [9], which reduces the risk of nocturnal hypoglycemia [10]. In addition to its effect on glycemic control, tofogliflozin improves high-density lipoprotein cholesterol (HDL-C) and triglyceride (TG) levels, decreases body weight and blood pressure, and elevates circulating adiponectin levels [11]. We previously investigated the effect of tofogliflozin on carotid artery intima-media thickness (IMT) [12], which is a marker of atherosclerosis [13], arterial stiffness [14], and patients’ quality of life (QOL) [15], in the “Using TOfogliflozin for Possible better Intervention against Atherosclerosis for type 2 diabetes patients (UTOPIA)” trial. Although tofogliflozin did not delay the progression of IMT thickening, it significantly improved glycemic control, body weight, body mass index (BMI), abdominal circumference, systolic blood pressure, HDL-C, arterial stiffness, and treatment-related QOL [12, 14, 15] during the 2-year intervention period.”
2 Likes
My BG elevates significantly after I taking high GI meal, sometimes it would elevate to prediabetic level.
I agree with you, I don’t want to take drug to control BG.
Because metformin has negative effect on testosterone and muscle mass to me.
Haven’t try SGLT2 but my BMI is only 22, I am afraid SGLT2 would have similar effect like metformin.
Berberine does not show much BG control effect on me.
Acarbose once caused me liver injury.
So I replace all my starchy food to quinoa, lentils and sweet potato, now my BG is much better. Low GI, high fiber food really amazing.
4 Likes
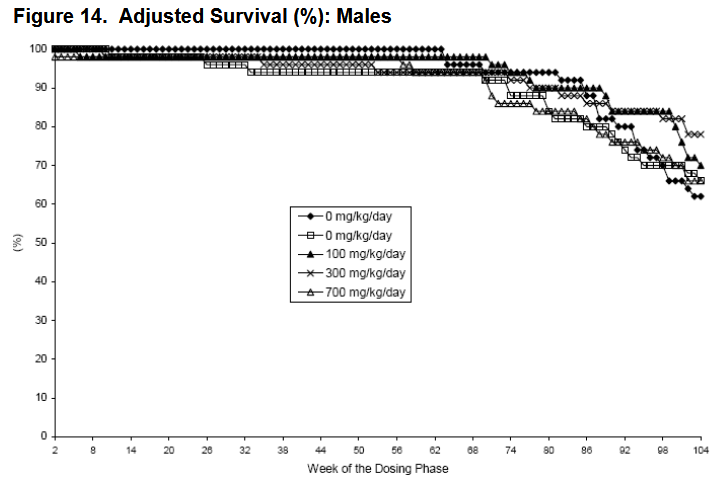
Good find! What’s the difference between the two “0”? And do we have the % difference in average and max lifespan? P-value?
I’m not sure, they seem to combine the 0 groups together for the final survival rate. It’s a large document and I haven’t looked at it carefully, I’m unsure if they have other data or where to get it, maybe the FDA has it (I started looking after this tweet by Alex Kesin: Should every drug go through mouse lifespan studies? - #5 by AnUser, drug developers probably have many such sources of information).
Unless I’m mistaken the high dose groups are doing better, but it doesn’t look like that on the graph to me. Higher dose groups had much lower body weight, as well, so could be a confounder.
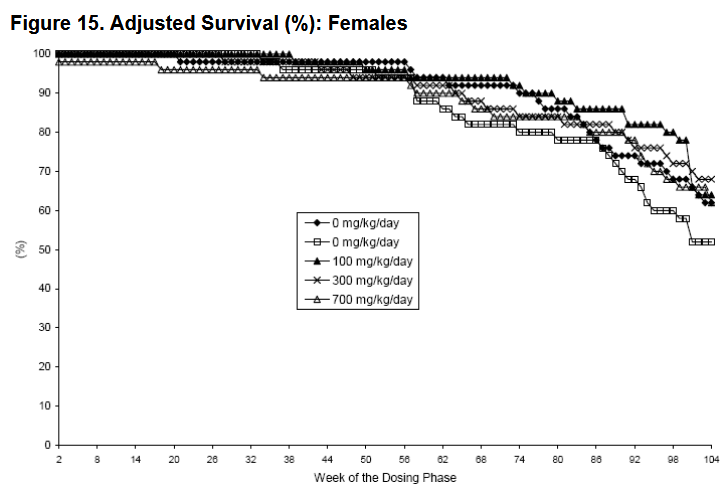
At termination the survival rates were 64, 70, 78 and 66% in males
and 57, 64, 68 and 62% in females in 0 (groups 1 and 2 combined), 100, 300 and 700
mg/kg-treated groups, respectively
Dapagliflozin
4 Likes
I’m not sure the higher dose group were doing better.
Page 99:
"Appropriateness of Test Models
The sponsor chose empagliflozin doses of 0, 0, 100, 300 and 1000 mg/kg/day based on the recommendations of the ECAC. Overall treatment was well tolerated and the results showed no dose-limiting toxicity, except for excess mortality in the high dose male group which was terminated at week 97. As all high dose males and females were terminated at weeks 97 and 102, respectively, the high dose was considered adequate for tumor assessment and statistical evaluation. Exposure at the high dose (700 mg/kg) provided approximately 45x and 62x the maximum recommended human dose (MRHD) in males and females, respectively, based on total exposure (AUC0-24h)."
Page 100:
"Mortality
Decreased survival was observed in the 1000 mg/kg males that resulted in early termination for this group at week 97 (see sponsor’s figure below). At study termination 16 males and 17 females were present in the high dose (HD) group. Although, a submission to the Division and ECAC was not made to request early termination of the HD male group, it is likely ECAC would have concurred if the number of survivors had reached 15 or less, prior to week 100 of the study. increased mortality observed for the HD male group was due to urinary tract dilatation. Given that all HD males and females were terminated at week 97 and 102, respectively, the HD group is considered adequate for tumor assessment and statistical evaluation."
Page 101:
“In the males the most common non-neoplastic cause of death was attributed to urinary tract dilatation that showed a treatment-related increase in the low, mid and high dose males (see sponsor’s table below). These lesions account for the early termination of the HD male group, and were described as dilated renal pelves, distended urinary bladder and/or uteral dilatation and renal tubular cysts that were observed macroscopically with renal/uretal dilatation and chronic progressive nephropathy. All other causes of death were not dose related (sponsor’s table below).”
Also, the bodyweight story was more complicated and sex dependent. Page 102:
"Body Weights
Treatment with empagliflozin had no effect on the mean body weight in both males and females at the end of treatment (see table below). Mean body weights were, however, statistically significantly (ss) reduced in all empagliflozin-treated males for weeks 12 to 78, and did not correlate with the observed increased food consumption (vehicle 1 and 2 were combined for the analysis). The reduced mean body weight ranged from 5-10% and was not dose-dependent. Mean body weights were also ss reduced 3-7% in the 100 and 300 mg/kg males from weeks 86-94, respectively. Similar final body weight at the end of the study appears due to a downward trend in body weight of both control groups, rather than a change in the dosed groups.
In contrast, there was a statistically significant increase in body weight at weeks 2-26 in the 1000 mg/kg females (data not shown but see sponsor’s figure below). The increase in body weight ranged from 5-12% and was associated with increased food consumption. However, overall body weight for the duration of the study was not statistically significantly increased. Mean body weight was also ss increased at weeks 4-13 and week 18 in the 300 mg/kg females. The increase in body weight was of a lower magnitude compared to the high dose females and ranged from 3-7%."
2 Likes
So the survival rate was 64% in control, 70% for 100 mg/kg, 78% for 300 mg/kg, and 66% for 700 mg/kg for male rats?
3 Likes
Well, most seems at the 300 mg/kg dose and drops off at 700 and higher (1000). But note early termination, not favorable trends. Dose, poison etc. Some sex differences.
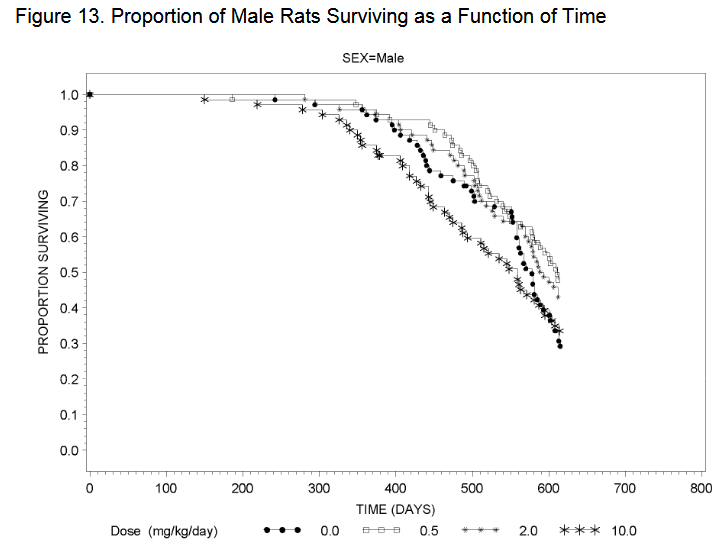
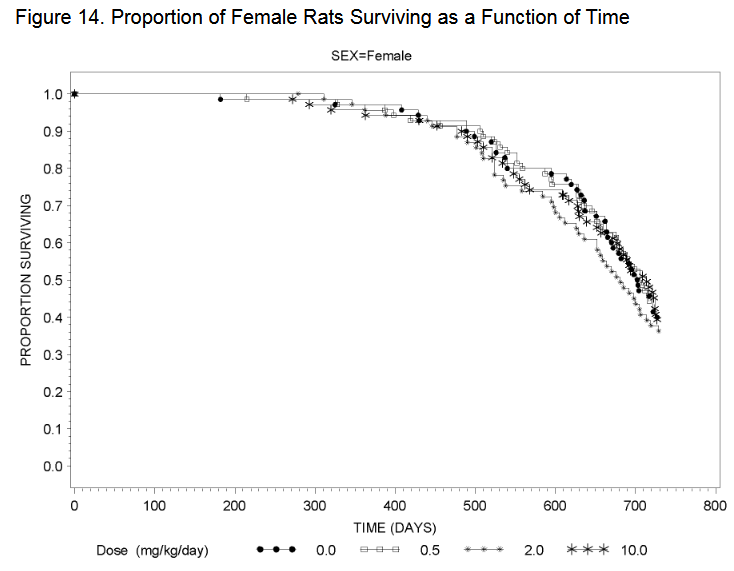
Amazing, thanks for sharing. So dapagliflozin and empagliflozin also increase lifespan in male mice. (We already had one Chinese paper on empagliflozin confirming that.) So it’s not only an SGLT1 effect @Neo.
Using the FDA conversion guide, 100 mg/kg = 650 mg/day, in a 80 kg human. The maximum approved dose is 25 mg/day. So there is no risk. But do empa and dapa also increase lifespan at these low doses?
7 Likes
Our findings uncover a novel molecular mechanism through which dapagliflozin improves myocardial mitochondrial injury under diabetic conditions, suggesting SORT1 as a potential therapeutic target for treating myocardial injury in diabetes.
3 Likes
Can you talk more to this?
1 Like
Will take a look.
@A_User @adssx - Is this a 2013 packet? But the result was never published in a paper?
2 Likes
That’s from the 104 week (2-year) carcinogenicity rat or mouse study that it seems most drugs have to do.
See this post:
3 Likes
blsm, I think of exercise as being 4 to 5 zones with a level 2 being a steady walk (and talk) for a mile or two before moving into a fast walk with very limited conversation as zone 3. From there it’s jogging (level 3) and sprinting (level 4). Can you describe your zone 2? I ask because I’ll be trying Empagliflozin soon, but I hate to think that it could mess up my exercise routines.
1 Like
Did you see Matt K’s comment on the other thread:
”(2) Lifespan studies are not carcinogenicity studies. Perhaps that wasn’t what the comment intended, but this is what it sounded like.”
What are your thoughts? I’d rather believe your point that this FDA packet provided longevity data - but is Matt saying that it is not that helpful? Or did he not understand the packet?
1 Like
I think Matt was addressing a separate point as
“… at relativley low cost (compared to the cost of moving an unworthy drug forward) in less than a year by starting in 24 month old mice.” and
“… assuming the goal is a geroprotector, not an incremental disease drug.”, etc, sound to me that Matt believes they were carcinogenicity studies in name only, basically what those studies are called.
The everolimus study I posted in that thread seems to have had a nice +25% effect on 104 week lifespan compared with control, and decrease in age-related effects, statistical significance testing aside, if you can take a look and if you agree.
2 Likes
Sure, I can’t decide if this change is good or bad yet. At first I was leaning towards good but now I’m not so sure. Here’s a little background and caveats: I’m a 55 y/o female, not an athlete or very knowledgeable about fitness but I’m pretty active. Fitbit fwiw gives me an excellent cardio fitness score of 43-47.
I average 10k steps per day, do sprint intervals for 15 minutes 1x/week, ruck for @40 minutes with 10-25% of my body weight 4-5x/week and lift weights 2-3x/week. I could easily achieve my goal of 40 total zone minutes per day without having to try before starting dapagliflozin. Fitbit breaks them down into moderate, vigorous and peak and around 75-80% of my zone minutes would be moderate and the remaining 20-25% vigorous/peak. I also wear a 10% weighted vest around doing my normal daily activities for a minimum of 2-4 hours daily but sometimes more.
I used to at least be in zone 2 or moderate for most of the time anytime I rucked and now doing the same thing I may not get my heart rate above 100 at all or for less than 5 minutes. I ruck on uneven terrain with small hills. I did discover recently that I can get into zone 3 or higher fairly easily on a stationary bike at the gym so perhaps it’s coincidental that I noticed this shortly after starting dapagliflozin and I’m simply adapted to rucking and needed a new challenge?!?!
It seems to be doing something good for my cardiovascular system so far where I have to work harder than I used to get into zone 2 or higher but perhaps I’m interpreting things incorrectly? I’m considering getting a more detailed tracker and I’m trying to learn and understand all of this more. I didn’t really start working on my fitness until 5 years ago and didn’t really need to understand it much to see results until recently. My husband says I’ve plateaued. I hope that long winded rambling helps!
3 Likes
Fitbit fwiw gives me an excellent cardio fitness score of 43-47.
I average 10k steps per day, do sprint intervals for 15 minutes 1x/week, ruck for @40 minutes with 10-25% of my body weight 4-5x/week and lift weights 2-3x/week.
Just had to comment… pretty impressive! Finding the time to do all that is part of the difficulty. I do a walk the dog ruck that helps kill two birds.
I think the Attia/Inigo San millan crowd defines exercise routines into three zones. Zone 1 is (I believe) similar metabolically to zone 2 but not maxing out the pathway. Zone 2 is defined as the point where you are maximizing your mitochondrial respiration for the production of ATP and generally corresponds to somewhere around 80% of maximal heart rate. Thus you are burning fats and getting maximal ATP from the process and not producing a lot of lactic acid. As you hit the next zone 3 you are unable to keep up with the activity using respiration so you begin using less efficient but more readily available energy substrates that are converted to ATP by anaerobic pathways and you begin to accumulate lactic acid.
2 Likes
Thank you! I’m trying to understand all of the better! @Joseph_Lavelle has been very helpful as well! I love this place.
1 Like