Here is some interesting info on sglt1 inhibition. Apparently sglt1 exists throughout the body including the brain. Perhaps a reason to pause on blocking uptake of glucose via sglt1. Your thoughts?
Does SGLT1 Inhibition Add Benefit to SGLT2 Inhibition in Type 2 Diabetes?
The SGLT2 (sodium-glucose cotransporter-2) inhibitors canagliflozin, dapagliflozin, empagliflozin, and ertugliflozin have been shown to improve cardiac and cardiorenal outcomes in patients with—and in some cases without—type 2 diabetes (T2D) who have heart failure or chronic kidney disease.1 The mechanisms associated with their beneficial effects remain controversial. Although the effects of SGLT2 inhibitors on cardiac and cardiorenal outcomes in both patients with and without T2D are both statistically and clinically significant, recent data from the SOLOIST (Effect of Sotagliflozin on Cardiovascular Events in Patients With Type 2 Diabetes Post Worsening Heart Failure)2 and SCORED (Effect of Sotagliflozin on Cardiovascular and Renal Events in Patients With Type 2 Diabetes and Moderate Renal Impairment Who Are at Cardiovascular Risk)3 trials with the dual SGLT1 (sodium-glucose cotransporter-1) and SGLT2 inhibitor sotagliflozin suggest that it may have important advantages compared with other SGLT2 inhibitors, at least in patients with T2D. Sotagliflozin provides greater inhibition of SGLT1 compared with all currently available SGLT2 inhibitors.
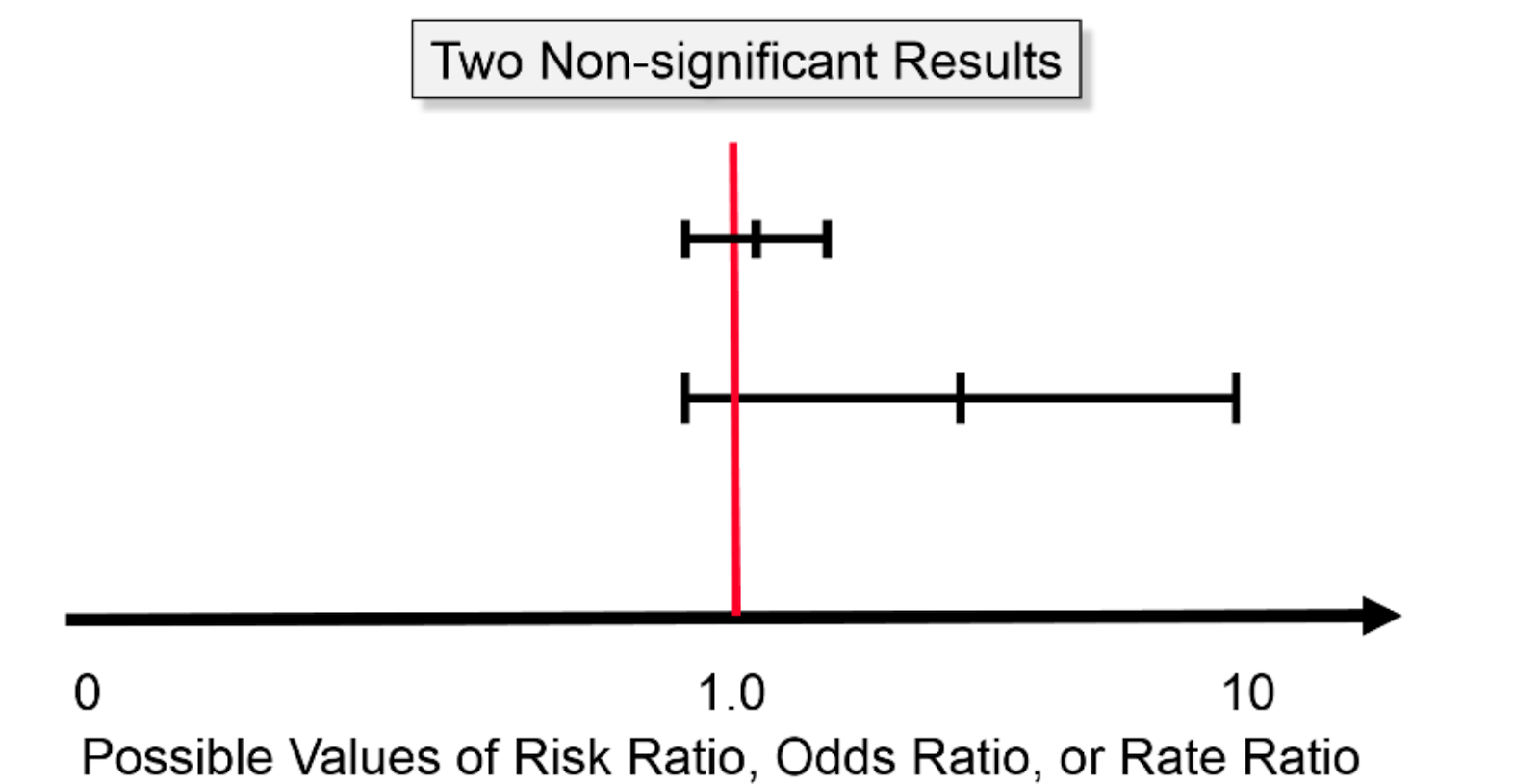
“For example, even if a huge study were undertaken that indicated a risk ratio of 1.03 with a 95% confidence interval of 1.02 - 1.04, this would indicate an increase in risk of only 2 - 4%. Even if this were true, it would not be important, and it might very well still be the result of biases or residual confoundin”
“The findings of this study indicate that dapagliflozin may offer greater lifetime economic value when compared with empagliflozin. Given that the current clinical practice guideline does not recommend one SGLT2 inhibitor over the other”
Bottom line I am currently taking empaglifozin, because that is what I have on hand.
Since dapagliflozin is cheaper, I will probably switch to dapagliflozin. This is the only argument that I can see for taking one over the other for people with no diabetes.
This is for patients with heart failure with reduced ejection fraction (HFrEF) only. (That being said, price is a valid argument, and I also use dapagliflozin…)
worth noting that there is another SGLT2 Inhibitor that is unique to india and in India it is dirt cheap. Possible to buy it alone or in combination pills with Metformin. Name is Remogliflozin sold 100mg
How much cheaper is it compared to dapagliflozin? I would not take a drug that was abandoned in the US, UK and Japan: Remogliflozin etabonate - Wikipedia
I use it because it is so cheap, it’s at least half the price of other SGLT2 inhibitors.
It was sold-on for financial reasons and probably because it’s a pro-drug with a poor half-life of 1.5-2hrs compared to 11-13hrs for others such as dapagliflozin, canagliflozin, etc.
Because it’s a pro-drug you have to take it before you want to kick-in, so I just take it with my immediate-release metformin an hour before meals.
" Remogliflozin is a recently launched candidate from the SGLT2 inhibitor class of drugs.17 The antidiabetic agent was shown to be effective, safe, and well-tolerated in a pivotal study.20 Remogliflozin demonstrated non-inferiority to existing SGLT2 inhibitor, namely dapagliflozin. The drug demonstrated comparable results in glycaemic, non-glycaemic, and safety parameters as compared to dapagliflozin…"
The price difference between empagliflozin and dapagliflozin from India is negligible. You should pick this med without considering price if buying from India.
It seems like it’s either empagliflozin or dapagliflozin for me.
My local pharmacy stocks both empaglifozin (Jardiance) and dapaglifozin (Forxiga) and seems that empaglifozin is cheaper, 34 EUR (both 10 and 25 mg) vs. 39 EUR (both 5 and 10 mg) for dapaglifozin. Empaglifozin is paid by insurance and dapaglifozin has a copay of 17 EUR. No generic dapaglifozin available yet.
What is your dapaglifozin dose? I assume you don’t take it for T2D…
I started on 5 mg/day and then switched to 10 mg/day after 1 month. I’m not diabetic, indeed. It was first recommended to my doctor to try treating my reactive hypoglycemia. It worked very well, and my doctor (who’s not a longevity doctor at all, just a normal 70yo doctor) said: “I’m happy to prescribe it to you for the rest of your life; it’s a very good drug, it’ll protect your heart and kidneys, but you’ll have to explain to people every single time you do a blood test why there’s glucose in your urine and why you’re taking it while not being diabetic.” Then I went down the SGLTi rabbit hole, and I’m now convinced of its longevity benefits and taking it for this reason (as well). So I’m a bit of a weird case.
The paper was not itself a study but contains 56 linked footnotes for its conclusions. Have yet to find anything negative about this drug except it’s short half life
Something to be aware of if taking urine tests and SGLT2i drugs:
SGLT2 Inhibitors and False Positive Toxicology Tests
A patient with diabetes who was taking empagliflozin, an SGLT2 inhibitor, had false positive urine screening tests for ethanol in a room-temperature sample, owing to bacterial fermentation of glucose that yielded ethanol.
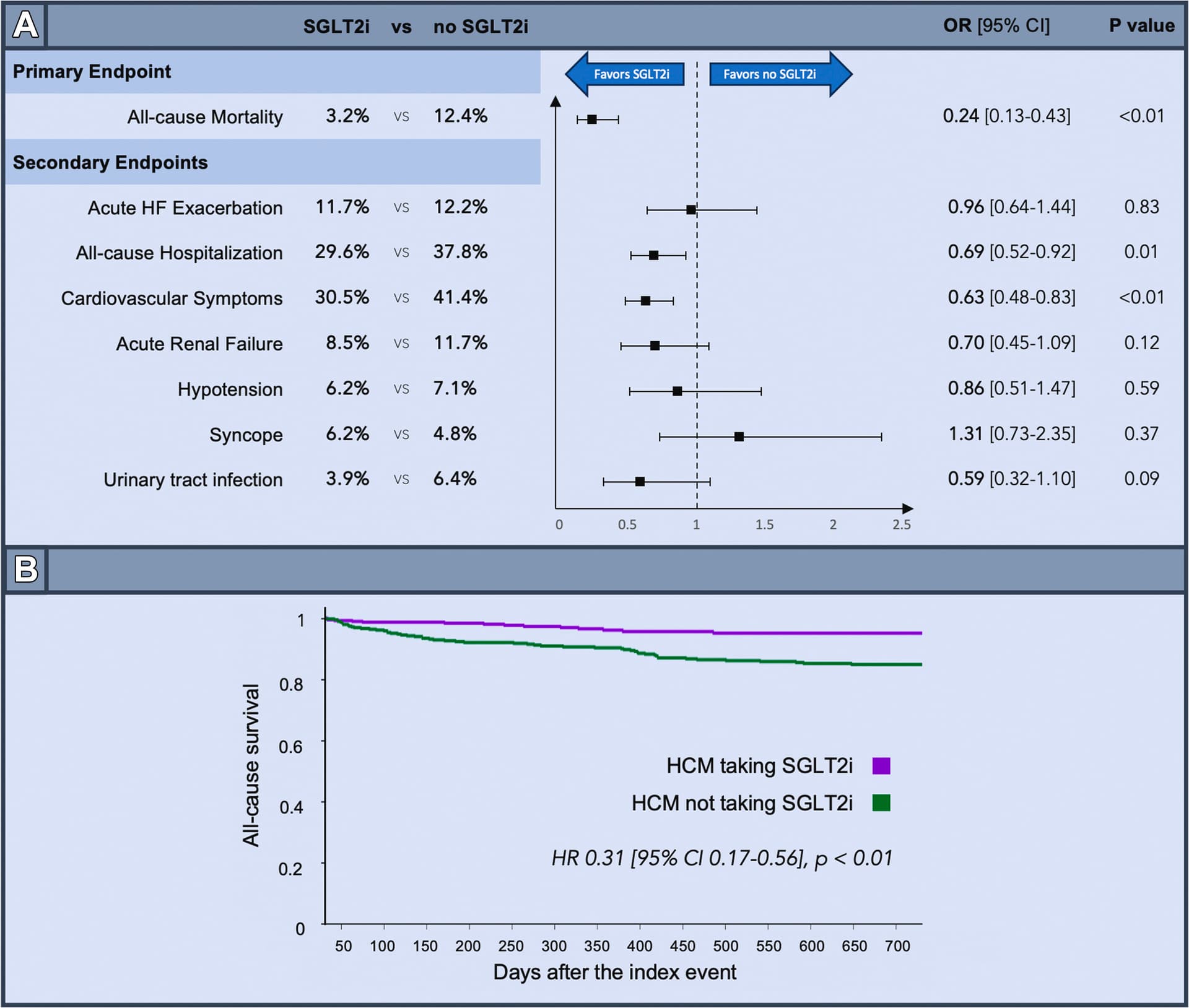
Over a 2-year follow-up period, HCM patients on SGLT2i had lower rates of all-cause mortality (OR 0.24, P < 0.01). Additionally, HCM patients on SGLT2i had lower rates of all-cause hospitalization (OR 0.69, P = 0.01) and cardiovascular symptoms (OR 0.63, P < 0.01) compared to propensity-matched HCM patients not on SGLT2i.
Zelniker et al. reported that dapagliflozin reduced the risk of atrial fibrillation and atrial flutter by 19% among the 17,160 patients with type-2 diabetes who participated in the prospective multicenter randomized DECLARE-TIMI 58 trial (Dapagliflozin Effect on Cardiovascular Events-Thrombolysis in Myocardial Infarction 58)
The mechanism for the association between SGLT-2 inhibition and the lower risk of atrial fibrillation or reduced recurrence of atrial fibrillation after catheter ablation is unclear. SGLT-2 inhibitors alter the activation of numerous genes in the heart, attenuating cardiac hypertrophy, inflammation, fibrosis, and apoptosis; activating antioxidant enzymes; decreasing the expression of hypoxia markers; and altering cardiac cell metabolism; all can affect the (re-)development of AF. As the expression of SGLT2 in the heart is negligible, it is probably not directly related to the inhibition of SGLT2 in cardiac cells. While alteration of expression and/or activity of mediators secondary to SGLT2 inhibition in the kidney or other organs or the alteration of metabolic utilization cannot be ruled out, the fact that favorable effects of SGLT2 inhibitors are seen in cardiac cells in in vitro models suggests the potential existence of yet an unidentified alternative target.
Despite the encouraging clinical results of various SGLT2 inhibitors in reducing atrial fibrillation risk, both challenges and research opportunities remain. Most existing studies are retrospective, which demonstrates the need for randomized and prospective studies to assess the impact of SGLT2 inhibitors on reducing the incidence or recurrence of atrial fibrillation in patients with or without heart failure, or type-2 diabetes. […] Thus, the jury is still out on the therapeutic effect of SGLT2 inhibitors on atrial fibrillation.
It is possible that, while SGLT2 expression is negligible in cardiac cells at baseline, de novo SGLT2 expression may exist in pathological conditions. Therefore, SGLT2 inhibitors could directly prevent atrial fibrillation–promoting mechanisms. On the contrary, if SGLT2 inhibitors have no direct effect on cardiac cells, this would further confirm that their role in ameliorating atrial arrhythmogenesis results indirectly from improved glucose metabolism and kidney function.
After matching, the use of DAPA in AMI patients was independently associated with a decline of AKI risk (OR 0.32; 95% CI, 0.19–0.53; P < 0.001) after hospital admission. Meanwhile, there were significant differences in mortality between the DAPA group and Ctrl group (2.5% vs. 7.6%, P = 0.012).
Changes in hematocrit and hemoglobin were the strongest mediators of empagliflozin’s kidney benefits in EMPA-REG OUTCOME participants with T2D and cardiovascular disease.
While I was very happy with Remogliflozin, but given the convenience and coverage of getting a far longer half life, and having found Dapagliflozin for 23 cents a pill within india (ADDII brand inside india Dartpapa 10) I just switched to it. I didn’t realize it could be found that affordably so thanks for bringing that up
Every single day we have new papers showing massive benefits for SGLTi users (among T2D, CKD, or HF => TBC if these findings extend to the general population):
Pooled data from seven observational studies revealed that SGLT2i use was linked to a lower risk of dementia in people with diabetes (OR 0.45, 95% CI 0.34–0.61; p < 0.00001, I2 = 97%).
According to this research, taking SGLT2i reduces the incidence of dementia in people with diabetes by having a beneficial neuroprotective impact. Randomized controlled trials (RCTs) are still required in order to verify the findings of our research.
After up to 5 years of follow‐up, SGLT2i use was associated with a significantly lower risk of incident dementia (hazard: 0.71, 95% confidence interval: 0.51– 0.98), particularly vascular dementia (HR: 0.44, 95% CI: 0.24–0.82). SGLT2i was related to reduced risks of AF‐related hospitalisation (HR: 0.72, 95% CI: 0.56–0.93), stroke (HR: 0.75, 95% CI: 0.60–0.94), and all‐cause death (HR: 0.33, 95% CI: 0.24– 0.44).
Compared with GLP-1RA, empagliflozin was associated with similar risks of MI or stroke [HR: 0.99 (0.92, 1.07); RD: -0.23 (-1.25, 0.79)], and lower risks of HHF [HR: 0.50 (0.44, 0.56); RD: -2.28 (-2.98, -1.59)], MACE [HR: 0.90 (0.82, 0.99); RD: -2.54 (-4.76, -0.32)], cardiovascular mortality or HHF [HR: 0.77 (0.69, 0.86); RD: -4.11 (-5.95, -2.29)], and ESKD [0.75 (0.60, 0.94); RD: -6.77 (-11.97, -1.61)]. Absolute risk reductions were larger in older patients and in those with baseline ASCVD/HF.