Metformin and Empagliflozin together achieve better results for lowering HBA1C than taking either alone. Most T2D patients take both. Acarbose reduces glucose spikes. Berberine is a Metformin substitute (almost). The way to tell if you are doing to much is if you experience bouts of hypoglycemia. You may need a glucose monitor to detect if your glucose levels get too low.
Metformin can give you hypoglycemia. I have read that Empagliflozin will not. Acarbose will just give you gas.
Speaking of synergy, does anyone have experience with SGLT2 and DPP4 inhibitor combinations? I am considering Glyxambi (Empagliflozin/linagliptin) specifically.
In addition, my mother’s cardiologist prescribed Metformin and Empagliflozin. There must be a synergy otherwise they wouldn’t be prescribed to treat T2D.
See also:
The clinical data reviewed show that the combination of empagliflozin/metformin offers the potential to improve glycemic control in T2DM and reduces body weight and blood pressure, vs each agent individually,
At week 24, adjusted mean reductions in HbA1c from baseline were significantly greater for patients receiving empagliflozin/metformin twice daily than those receiving either empagliflozin once daily (P < .001) or metformin twice daily (P < .01). Significantly greater proportions of patients treated with combination therapy reached HbA1c <7.0% at week 24 compared with patients who received either agent alone (P < .05 for all comparisons).
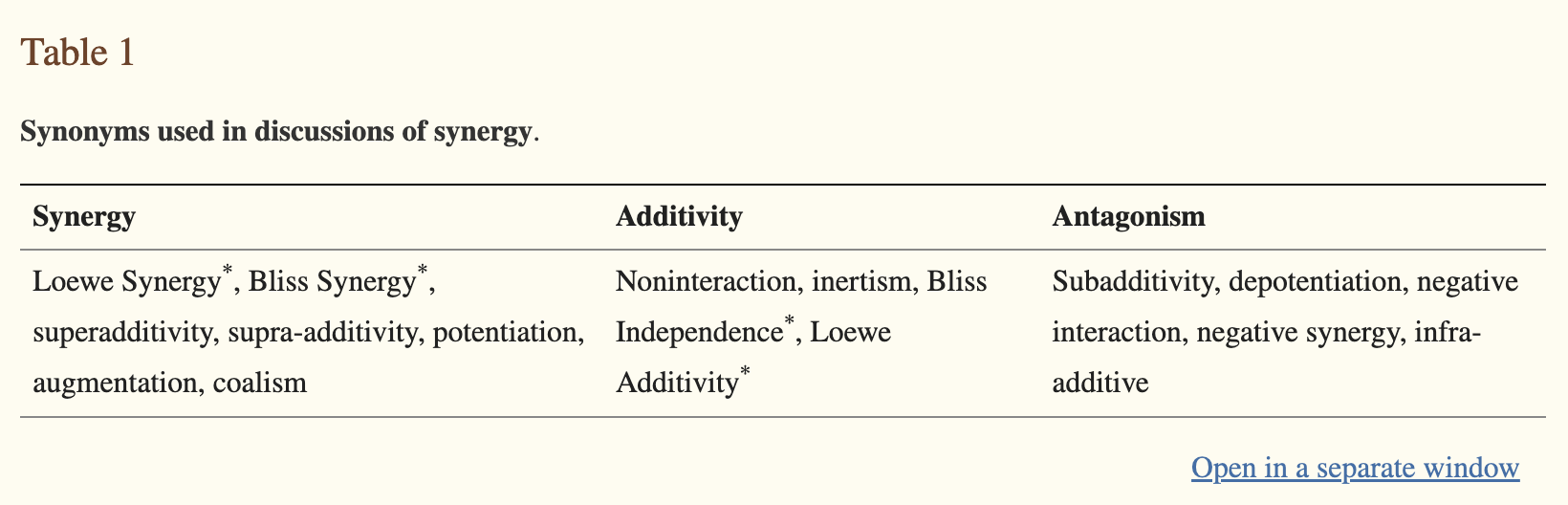
Synergistic means that the combination produces “a combined effect greater than the sum of their separate effects”
This is not the case of metformin + SGLT2. In terms of long-term outcome, the data I found (posted above) shows that metformin + SGLT2 does not do significantly better than metformin alone.
Yes, they may be subadditive, but taking both substances reduces HBA1C more than either one alone. So, yes, I guess they are not synergistic. However, when you are treating T2D, you are trying to get HBA1C back to normal ASAP.
I would argue that the majority of interventions we initiate for longevity are subadditive as well. However, that doesn’t mean it isn’t in our best interest to get whatever extra effects for lifespan or healthspan we can.
Highly unlikely IMO.
I have been using metformin for decades and have experimented with various dosing levels and have never experienced dangerously low blood glucose levels. Maybe people who have type II diabetes react differently to metformin.
The times when I have experienced hypoglycemia has been while taking a relatively high dosage of Metformin (1.5-2 g daily). I would get hit with hypoglycemia at around 4 pm on regular occasions. It feels like a heart attack but goes away in a few minutes if you take sugar. If I don’t take high levels of Metformin, I don’t experience the issue.
My doctor told me it was hypoglycemia, so that’s what I have assumed.
Well, actually I am looking more for “is there any synergies” or they both work on their own way. I tend to say things not so directly from time to time. Anyway, As far as interaction I don’t think there any interaction. Since we are on the subject does acarbose makes sense to be taken in addition to Jardiance?
I eat four meals per day. I take 10mg Empagliflozin with breakfast, then 50mg Acarbose with each of the following three meals (150mg total). I would imagine it’s synergistic. I believe they are prescribed together sometimes.
Another possible mechanism behind SGLT2 benefits is increased magnesium levels. I wonder if we can get away with consuming slightly less magnesium if we take an SGLT2, saving money on a magnesium supplement.
Sodium–glucose cotransporter 2 (SGLT2) inhibitors reduce the risk of kidney disease progression in people with or without diabetes as well as the risk of acute kidney injury and hyperkalemia.
SGLT2 inhibitors reduce the risk of cardiovascular death and heart failure hospitalization among people with type 2 diabetes mellitus and have beneficial effects on key heart failure outcomes irrespective of diabetes status or left ventricular ejection fraction.
SGLT2 inhibitors modestly lower systolic and diastolic blood pressure without a significant increase in risk of hypotensive episodes and have modest benefits for weight loss.
Other benefits of SGLT2 inhibitors include improvements in liver outcomes in people with metabolic dysfunction-associated steatotic liver disease, reduced risk of symptomatic kidney stone events, improvements in anaemia outcomes and potential reductions in the risk of new-onset atrial fibrillation and new-onset diabetes.
SGLT2 inhibitors have a generally favourable adverse effect profile but are associated with increased risk of genital mycotic infections and a small increased risk of diabetic ketoacidosis; they should be used with caution in people with unstable volume status owing to the risk of hypovolemia. Prescription of SGLT2 by clinicians and patient adherence are suboptimal despite strong evidence for the efficacy and cost-effectiveness of these therapies.
Strikingly, canagliflozin but not empagliflozin reduced fluid transport across cell monolayers, and dramatically inhibited endocytic uptake of albumin. These effects were independent of glucose and occurred at clinically relevant concentrations of drug.
Mice given a single dose of canagliflozin excreted twice as much urine over 24 h compared with empagliflozin-treated mice despite similar water intake.
Though sodium-glucose co-transporter-2 inhibitors (SGLT2i) increase the risk of mycotic genital infections (MGI) and possibly urinary tract infections (UTI), their cardiovascular benefits in patients with heart failure far outweigh those risks.
Currently, the mechanism of the protective effect of SGLT2 inhibitors on myocardial infarction is not yet understood. Mendelian randomization analysis uncovered a causality between SGLT2 inhibition and myocardial infarction.
Based on proteome-wide mendelian randomization, APOB and CCL17 were seen as mediators in the protective effect of SGLT2 inhibition against myocardial infarction.
In the study, the swimming performances of three groups of rats were evaluated by dividing them into control, sacubitril/valsartan and dapagliflozin groups. […] In the comparison of dapagliflozin and control groups, a statistical difference was observed starting from the 10th swimming session, and when the total and average swimming times were compared, the p values were <0.001 and <0.001. In triple analysis, a statistical difference was seen from the 9th swimming session until the end of the experiment. […] Our study showed a limited positive effect of sacubitril/valsartan on athletic performance. The impact of dapagliflozin on athletic performance was shown to be particularly significant.
The results show that DAPA promotes WAT “browning” and improves metabolic disorders. […] These findings provide a rational basis for the use of DAPA in treating obesity by promoting the browning of white adipose tissue.
Comparative analysis with other SGLT-2 inhibitors suggests dapagliflozin’s potential superiority in preventing heart failure. Compared to empagliflozin, it has more extended effects, contributing to stable sodium diuresis, reduced blood pressure fluctuations, and potentially lower cardiovascular disease risks. However, it leads to less urinary glucose excretion compared with canagliflozin.
Compared with GLP-1 receptor agonists, the SGLT-2 inhibitor-GLP-1 receptor agonist combination was associated with a 30% lower risk of major adverse cardiovascular events (7.0 v 10.3 events per 1000 person years; hazard ratio 0.70, 95% confidence interval 0.49 to 0.99) and a 57% lower risk of serious renal events (2.0 v 4.6 events per 1000 person years; hazard ratio 0.43, 0.23 to 0.80). Compared with SGLT-2 inhibitors, the GLP-1 receptor agonist-SGLT-2 inhibitor combination was associated with a 29% lower risk of major adverse cardiovascular events (7.6 v 10.7 events per 1000 person years; hazard ratio 0.71, 0.52 to 0.98), whereas serious renal events generated a wide confidence interval (1.4 v 2.0 events per 1000 person years; hazard ratio 0.67, 0.32 to 1.41).
In this cohort study, the GLP-1 receptor agonist-SGLT-2 inhibitor combination was associated with a lower risk of major adverse cardiovascular events and serious renal events compared with either drug class alone.