Like all of these, pulsed dosing is probably best…
perhaps a good strategy would be to take the SGLT2 inhibitor for 5 of the 7 days, starting at the same time as the rapamycin dose, thus leaving day 6 and 7 with minimal mTORC1 inhibition…
Like all of these, pulsed dosing is probably best…
perhaps a good strategy would be to take the SGLT2 inhibitor for 5 of the 7 days, starting at the same time as the rapamycin dose, thus leaving day 6 and 7 with minimal mTORC1 inhibition…
Maybe but a total guess. That’s the frustration, flying blind. No idea how you can scientifically define “best” as it relates to our objective, longevity.
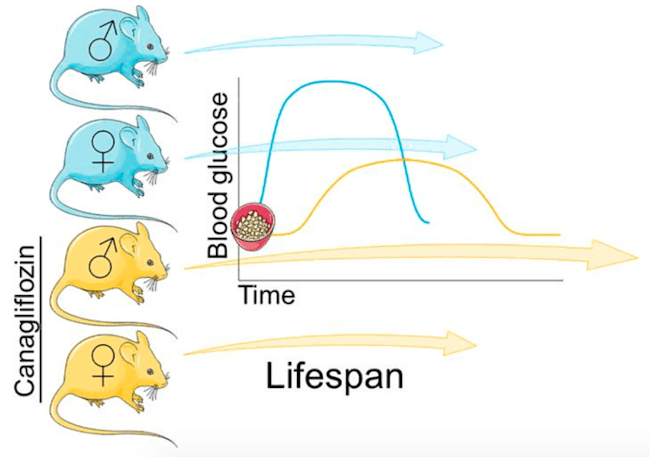
The agony of the early adopters… ![]()
Great paper on normal (non diabetic) wild type mice, but sadly, “tumorigenesis was inhibited or decelerated by this drug, though only in males”
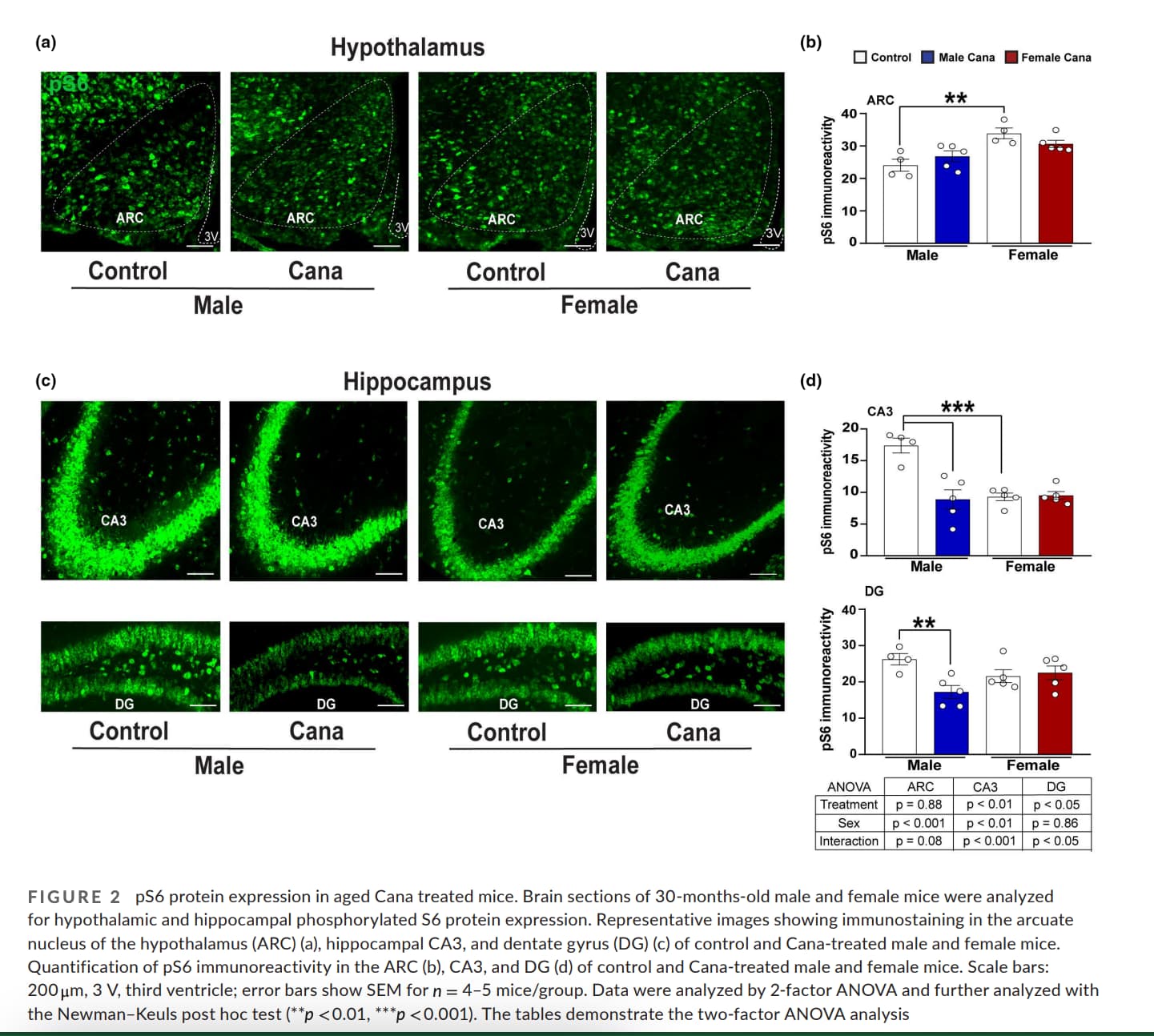
“In the current study, we show that Cana reduced hypothalamic gliosis in both sexes, which may contribute to improved whole-body metabolism. Cana treatment was associated with reduced pS6 in the hippocampus of 30-month-old male mice, implicating reduced mTOR signaling. Previous studies have shown that Cana’s effects on metabolic health were associated with suppressed mTOR signaling, as shown by reduced hepatic pS6 signaling accompanied by increasing AMPK activity in young animals”
Yet agin… > lower glucose > lower insulin signalling > lower brain mTOR > longevity/cognitive
Something to be aware of for people who may be going in for surgery…
Seems like SGLT2 inhibitors don’t mix well with anesthesia due to increased risk of ketoacidosis , note it seems it may also be an issue with concomitant use of SGLT2 inhibitors during prolonged fasting (so, it sounds best to avoid SGLT2 inhibitors during fasting, or if you are on a Keto Diet) … from a new academic conference its seems.
Details/discussion below:
Empagliflozin has been reported to protect endothelial cell function, regardless of diabetes status. However, the role of empagliflozin in microvascular protection during myocardial ischemia reperfusion injury (I/R) has not been fully understood.
Conclusions
These results demonstrated that empagliflozin can protect the microvasculature by inhibiting the DNA-PKcs/Fis1/mitochondrial fission pathway during myocardial I/R injury.
Full Paper:
“We’ve had a few normoglycaemic ketoaxidotic patients here.”
A “few” in just one reporting center?
Introduction: Non-diabetic ketoacidosis is a rare condition which can be caused by starvation. Lack of glucose can force the body into ketogenesis causing a metabolic acidosis. As previously reported in the literature, ketoacidosis might, on rare occasions, be caused by a diet with low carbohydrate content. However, to the best of our knowledge this is the first reported case in the literature of ketoacidosis, in a non-diabetic patient, associated with a combination of low carbohydrate, high fat diet and lactation.
Case presentation: A healthy non-diabetic, 32-year old white woman started a low carbohydrate, high fat diet when she was breastfeeding her son of 10 months of age. After 10 days she was admitted to our hospital with nausea and vomiting and a serum pH of 7.20 and base excess of −19. Clinical signs and blood samples were compatible with ketoacidosis. She was given fluids intravenously and insulin. No anamnestic or clinical signs of diabetes were found. She recovered quickly and was discharged 3 days later.
Conclusions: Ketogenic diets like low carbohydrate, high fat may induce ketoacidosis. Lactation might further aggravate the condition and can perhaps even be the trigger into ketoacidosis. Health services should be aware of the risks associated with ketogenic diets, and be able to recognize this serious condition when it is presented.
A lactating woman has a high demand of substrate to produce milk. A LCHF diet limits the amount of substrate and results in a negative energy balance. This kind of diet should thus be avoided during lactation.
Our case shows that medical services should be aware of the fact that a strict LCHF diet often leads to ketosis and in rare cases even into ketoacidosis which is a dangerous condition that must be immediately diagnosed and treated in order to reduce morbidity.
does SGLT2 inhibitors prevent the re-absorption of fructose?
Interesting that this SGLT2 inhibitor reduces cardiac mTOR
Conclusion
SGLT2 inhibition reduced left ventricular fibrosis in a murine model of cardiac hypertrophy. Mechanistically, this was associated with reduced cardiac insulin- and increased AMPK-signaling as a potential mechanism for less cardiac mTOR-activation with alleviation of downstream ER stress, UPR and apoptosis.
The 334-patient study tested the two-med combo against phentermine alone, canagliflozin alone, and a placebo. After 26 weeks, patients using the combo had lost 7.5% of their body weight, compared with 4.1% in those taking phentermine alone, 1.9% of those only taking canagliflozin, and 0.6% of placebo patients.
Also, almost two-thirds of the patients taking both drugs reduced their body weight by at least 5%, compared with 17.5% of placebo patients.
“The findings support the potential clinical impact that canagliflozin could have on the lives of people constantly having to manage their weight,” said Dr. James List, global head of cardiovascular and metabolism at J&J’s Janssen unit. "We are committed to pursuing transformational therapies and hope to grow our understanding of how canagliflozin can be used to help more patients in the future.”

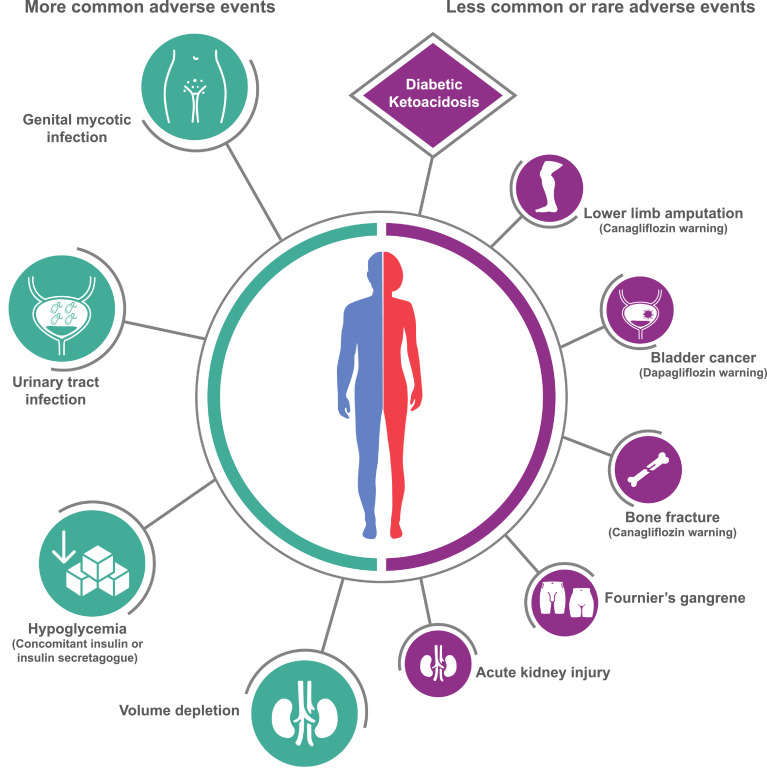
I don’t really like the sound of the risks and side effects even if rare. Also, azithromycin is not used for urogenital infections or cellulitis in the genitals (Fourier’s gangrene requires immediate surgery). I am scratching my head with Dr. Green’s Z pak thought process and I also cover why azithromycin can be potentially life-threatening dangerous given specific situations and risk factors commonly seen in this forum.
But going to research this one a bit more.
https://www.ajconline.org/article/S0002-9149(19)31179-8/fulltext
As you know blood glucose levels increase in the elderly, I am 81 and chose to use
empagliflozin instead of increasing my dose of metformin. This is from a source referenced by the source you provided. It looks to me that empagliflozin is pretty safe. Every drug and supplement from aspirin to rapamycin has risks. One always has to weigh the risk/benefit to decide whether or not to take a certain supplement. If you are young and healthy you probably don’t need any supplements other than rapamycin if you are seeking life extension.
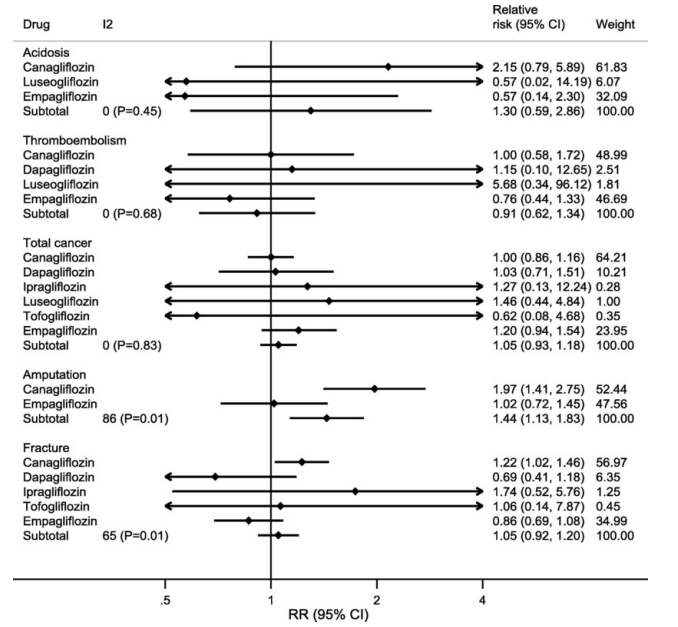
I really like the table.
The bold words are my emphasis.
"Conclusion
There are strong overall associations of SGLT2 inhibition with protection against major cardiovascular events, heart failure, serious decline in kidney function and all-cause death. SGLT2 inhibitors were also associated
with infections, volume depletion effects and amputation. Some associations appear to differ between compounds."
"Overall, use of SGLT2 inhibition was associated with favourable effects on major cardiovascular events, non-fatal myocardial infarction, hospitalisation for heart failure and all-cause death (Fig. 2). The I
2 statistic indicated a
high likelihood of differences between compounds beyond chance for cardiovascular death (I
2 = 80%) and a corresponding moderate likelihood of differences beyond chance for all-cause death (I
2 = 55%). There was no association of
SGLT2 inhibition detected for hospitalisation for unstable angina or stroke but for the latter there was a moderate likelihood of differences between compounds beyond chance (I
2 = 61%)."
"Effects of SGLT2 inhibitors on kidney disease outcomes
There were just two compounds with data describing effects on the renal outcomes of interest [10,47] and there were strong associations of SGLT2 inhibition with protection against progression of albuminuria and the renal composite outcome"
“Evidence of differences in protective effects was strongest for the outcome cardiovascular death, where empagliflozin appeared to provide a greater magnitude of protection. There was a corresponding, though less strong, finding for all-cause death that was probably driven by the effect on cardiovascular death”
"The association between amputation and use of SGLT2 inhibitors is a new finding that appeared to be restricted to canagliflozin.
The studies and summary risk metrics are using diabetics, not healthy persons. I guess you’re not altering your risk calculus considering how healthy you are at 81? Could some of these side effects increase in older persons, diabetic or not? Kidney function is a huge concern, IMHO. I didn’t look for any age stratification, albeit diabetic population.
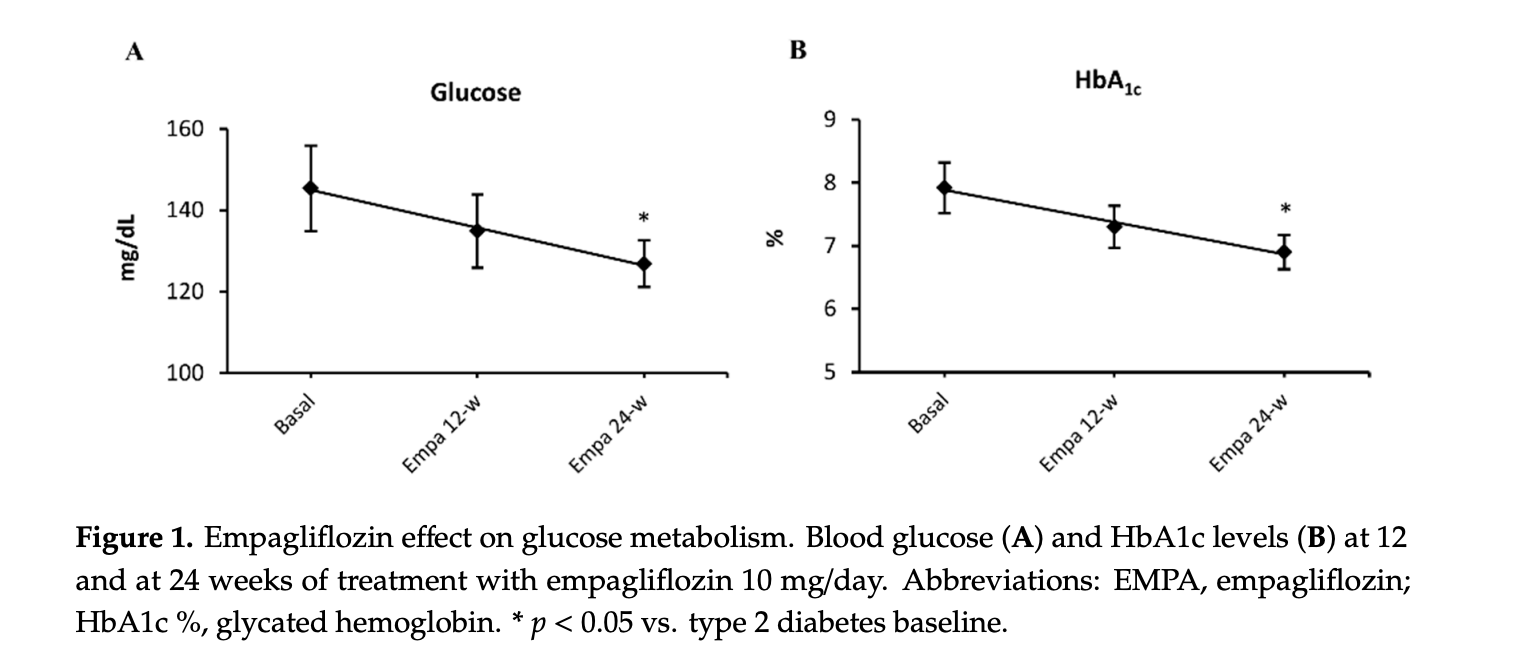
Looking at impact on glucose and hbA1c Empagliflozin @ 10mg/day, you would think diet/exercise could easily achieve these objectives? But then again, that’s why these people are T2D, lack of lifestyle control.
I am definitely in the low glucose AUC for longevity camp. I’ve taken a good axe hack at AUC glucose with strict keto. I for sure would go hypoglycemic taking one of these meds. Some days I veer into hypoglycemic (< 3.9 mmol/L).
I wonder how big this risk truly is (of hypoglycemia) for healthy people. I thought that one of the primary effects of this class of drugs (as with acarbose) is the just flatten the curve, thus reducing the blood sugar spike we get after consuming food / carbs., but with no change in the AUC. At the same time I wouldn’t recommend SGLT2 inhibitors to anyone on a Keto diet, due to the risk of ketoacidosis as identified in posts above in this thread.
“The risk of hypoglycemia associated with SGLT2 inhibitors is low, unless co-administered with insulin or an insulin secretagogue”. From the source above by @tongMD
Also, as a circumcised male, the risk of genital infections (especially for those of us who have never had such an infection ever before) seems extremely low (and this is the highest risk side effect I believe) and easily treatable in the low chance it does happen.
SGLT2 inhibitors are associated with an increased risk of genital mycotic infection, 5,6 particularly in patients with a history of genital mycotic infection and in uncircumcised males.1, 2,3, 4Genital mycotic infections occur more frequently in females than males receiving treatment with SGLT2 inhibitors, are generally mild or moderate in severity, and respond to standard antifungal therapy.
The other risk are UTIs. Again - in healthy, non diabetic males, with no previous history of UTI, it seems like a low risk:
Data on the potential SGLT2 inhibitor-associated risk of urinary tract infection (UTI) are less consistent, and published reports have provided conflicting conclusions. Some SGLT2 inhibitor studies suggested an increased associated risk of UTI, whereas others did not.
Its unclear to me why exactly anyone would think that the risk of serious side effects with SGLT2 inhibitors is unacceptably high for healthy, younger males with a low to moderate carb diet. I don’t see the specific risk factors that are high - especially when using SGLT2 inhibitors in a pulsed dosing fashion (My default right now is 5 days out of 7, so a two day “off” period each week.
My family has a history of type II diabetes, so in spite of my healthy life style, my glucose levels have risen over the years so I have to use drugs such as metformin and empagliflozin to keep my fasting glucose level under 100 mg/dL and my hemoglobin A1c under 5.7 % of total Hgb. Supplements such as berberine have had no detectable effect on my glucose levels.
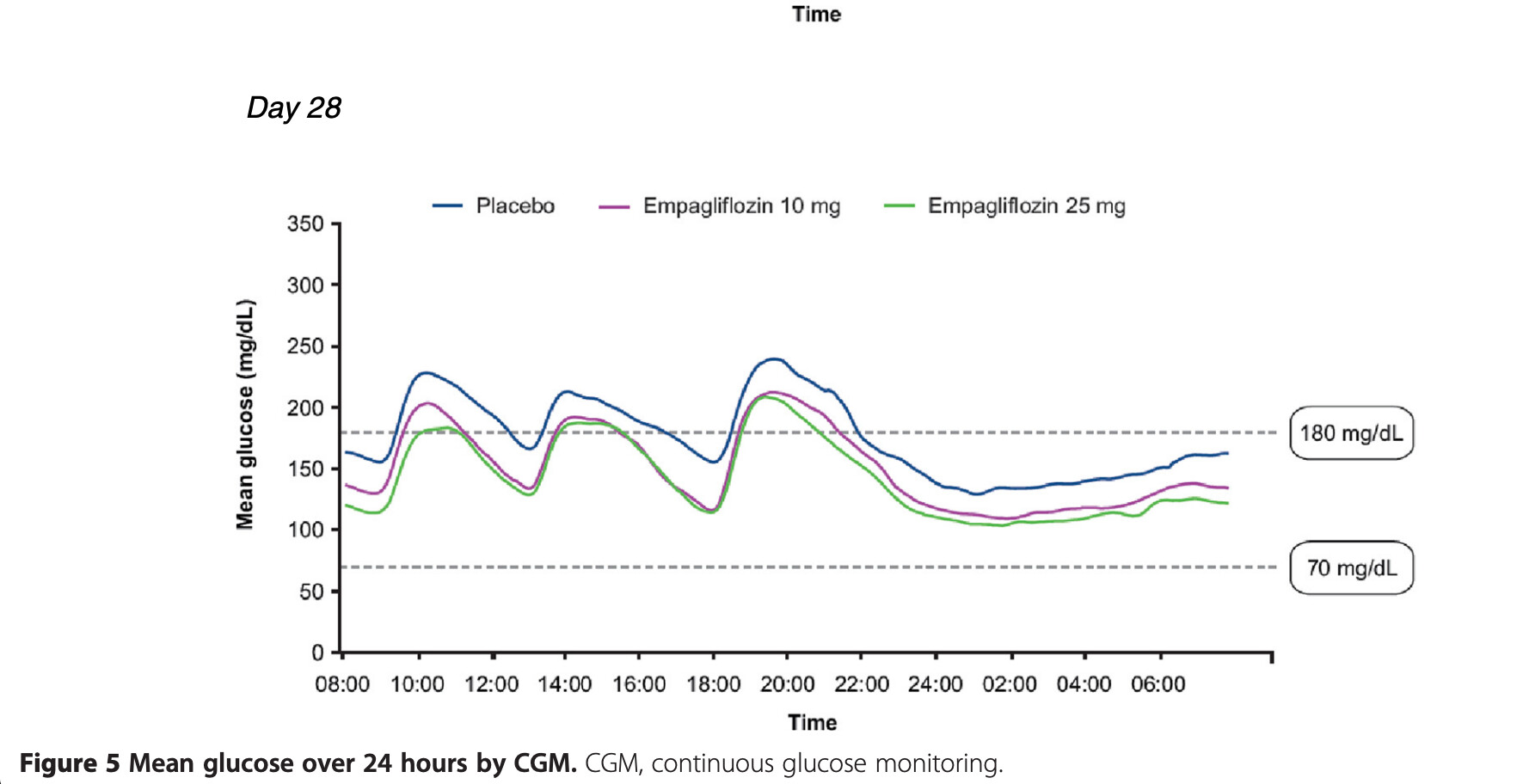
Not so, look at glucose with CGM vs placebo (human data). It takes (shifts) the entire glucose curve down with dosing. There is no flattening. The AUC (using 0 mg/dL as reference) is most definitely reduced.
Interesting…
That seems to contradict what Richard Miller and his team is reporting:
Admittedly - the ITP study is in mice not humans.
Though, in the study you just referenced: “Effect of empagliflozin monotherapy on postprandial glucose and 24-hour glucose variability in Japanese patients with type 2 diabetes mellitus: a randomized, double-blind, placebo-controlled, 4-week study” - the people are diabetic.
I wonder if there is any data on the blood glucose curve impact of SGLT2 inhibitors in healthy, non-diabetic populations? I will look.
Ah those mice and the ITP…translation to humans is massive leap.
I didn’t find first glance, but my guess…curve will be SAME, just perhaps the delta shift might not be as much.