“Canagliflozin, the other dual SGLT inhibitor, is more selective to SGLT2 than SGLT1 compared with sotagliflozin (250-fold vs 20-fold, respectively). “
It looks like Cana does have a smaller (order of magnitude less) effect on sglt1 than sotagliflozen. I don’t think the other popular SGLT2 inhibitors have any sglt1 inhibition. Is the the sglt1 effect important to the longevity benefits? I wonder…
However, according to SGLT inhibitors for improving Healthspan and lifespan: “Empagliflozin, dapagliflozin, and sotagliflozin are the agents in the SGLTi drug class with the strongest safety and efficacy for improving healthspan and lifespan.”
Thanks for the info. The last link you provided should be read by everyone on this forum. I had no idea of the wide range of benefits for Sglt2 inhibitors… and I’m taking one (Farxiga).
Based on surface under the cumulative ranking curve (SUCRA), the top ranked SGLT2i for reducing HFH were canagliflozin (95.5%), sotagliflozin (66.0%) and empagliflozin (57.2%). Head-to-head comparisons found no significant differences between individual SGLT2i in reducing CV death. “Add-on” SGLT2i reduced all-cause mortality compared with SoC alone, although only dapagliflozin was statistically significant. […] Among them, canagliflozin may be considered the preferred treatment for patients with diabetes and a history of heart failure, but it may also be associated with an increased risk of any adverse events compared to other SGLT2i. However, a sensitivity analysis focusing on HF-specific trials identified sotagliflozin as the most likely agent to reduce CV-death/HFH, followed by empagliflozin and dapagliflozin.
Where sotagliflozin will be adopted into the treatment of HF is unclear due to the evidence and benefits of already established SGLT2 inhibitors and the need for comparison with SGLT2 inhibitors. […] Given the limitations of currently available evidence, including difficulty in fully interpreting the trial results due to changes in primary endpoints, not adjudicating the events, and not reaching the original power calculations, more investigation is warranted to determine the benefit of sotagliflozin compared with SGLT2 inhibitors.
No differences were observed in the effect of empagliflozin and dapagliflozin on CV death (HRempagliflozin: 0.81; 95% CI 0.68-0.97, HRdapagliflozin: 0.88; 0.82-0.95, p=0.39) and all-cause death (HRempagliflozin: 0.86; 95% CI 0.73-1.02, HRdapagliflozin: 0.87; 0.78-0.97, p=0.94).
My two cents based on all the above: the differences don’t seem massive between the various SGLT2i, empa and dapa seem safer and as efficient if not more than cana, and sota is promising but hasn’t been tested enough.
FWIW:
"We found similar reductions in worsening HF with empagliflozin, canagliflozin and dapagliflozin. However, *empagliflozin was associated with a greater reduction in all-cause and cardiovascular mortality.
“Comparative efficacy of sodium-glucose cotransporter-2 inhibitors (SGLT2i) for cardiovascular outcomes in type 2 diabetes: a systematic review and network meta-analysis of randomised controlled trials”
Thanks. One caveat: it’s based on data “up to August 12, 2019”. Given how recent SGLT2i are (first approved in 2012 in the EU and 2013 in the US), newer papers may lead to different results.
I like this idea… I am shocked that the ITP only had 28 submissions last year, so I think we need to increase the suggestions given all the compounds we see that are interesting. It would be interesting to tease out the benefits of SGLT2 vs. SGLT1 inhibition in longevity.
And we should scrape our forums for other good compounds to suggest they test. We have about 3 months to do this.
I think 28 was the number of proposals that made it through the vetting process. Not sure how many ill-formed or poor quality proposals were tossed before consideration. Matt Kaeberlein probably knows.
You have to follow a certain format or template to be considered. Any researcher could probably provide it.
One listing all compounds suggested by the community, with links to detailed posts (below),
Then, for each of these drugs, one wiki post with the dossier defending the drug. The format is easy; it’s described in great detail here ( Application Instructions | National Institute on Aging ), so we could have an empty template for each compound that members would fill up with the required information.
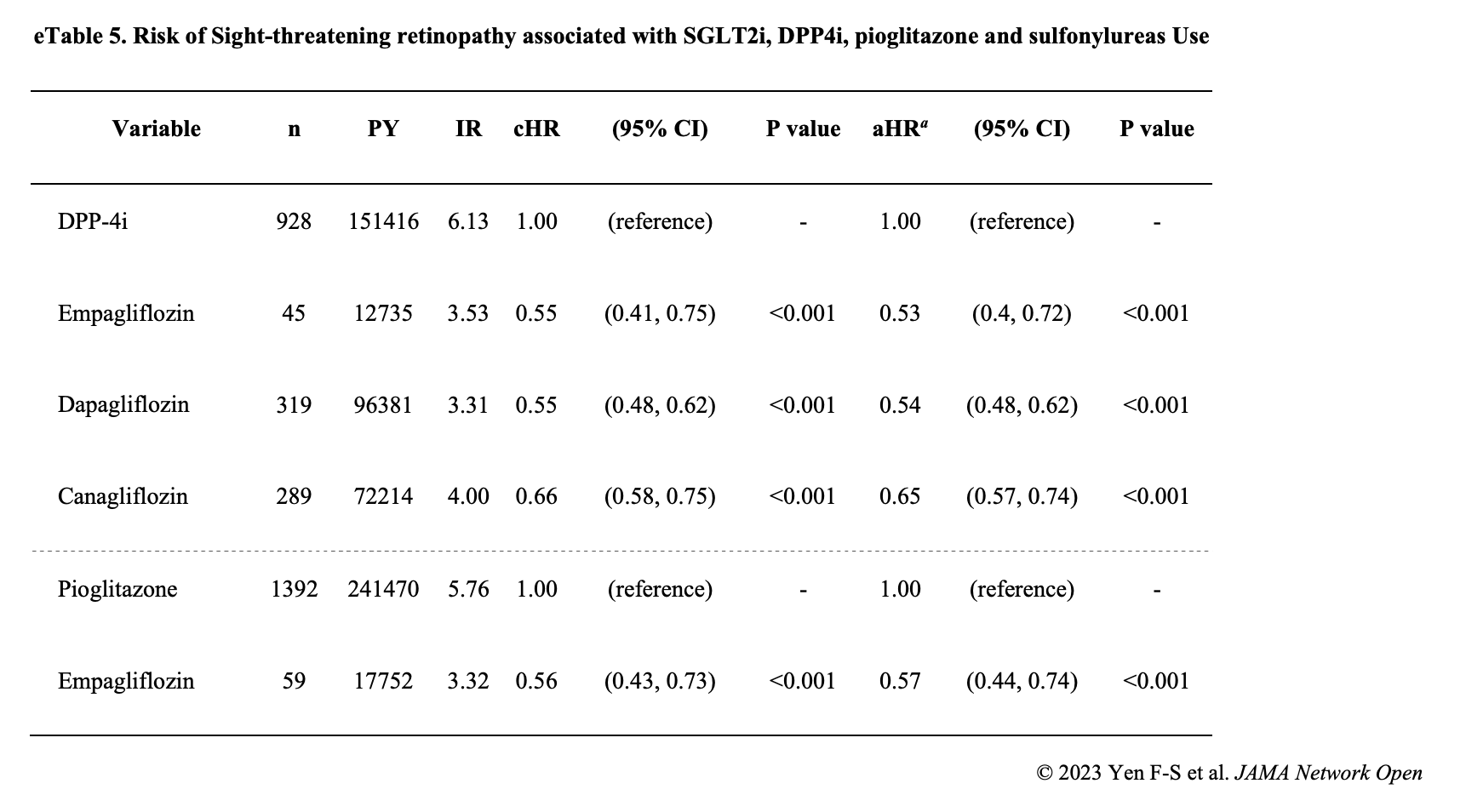
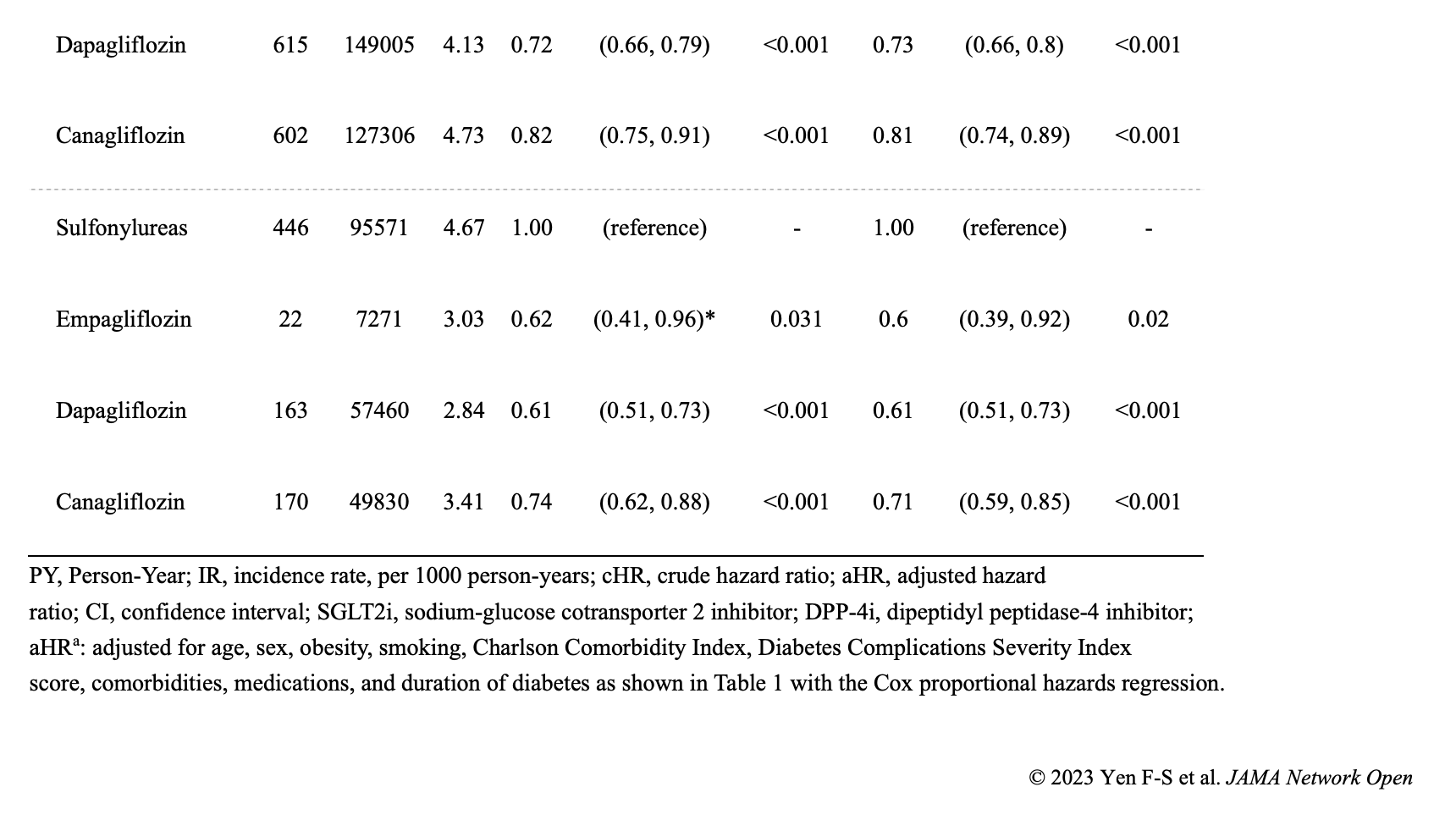
Sodium-glucose cotransporter 2 (SLGT2) inhibitor use was associated with a significantly lower risk of sight-threatening retinopathy than dipeptidyl peptidase-4 inhibitors, pioglitazone, and sulfonylureas among patients with type 2 diabetes (T2D), according to new research.1
Across the nationwide cohort in Taiwan, the potential protective role of SGLT2 inhibitors for sight-threatening retinopathy was observed across various subgroups of patients, including by age, sex, comorbidities, and medication use.
“In matched patients, empagliflozin, dapagliflozin, and canagliflozin were associated with a significantly lower risk of sight-threatening retinopathy than DPP-4i, pioglitazone, and sulfonylureas (eg, vs DPP-4i: AHR, 0.53 [95% CI, 0.40-0.72]; 0.54 [95% CI, 0.48-0.62]; and 0.65 [95% CI, 0.57-0.74], respectively; P < .001) (eTable 5 in Supplement 1). Also in the matched cohorts, SGLT2i compared with DPP-4I, pioglitazone, and sulfonylurea was associated with a significantly lower risk of dialysis (eg, vs DPP-4i: AHR, 0.05; 95% CI, 0.03-0.08; P < .001), hospitalizations for heart failure (eg, vs DPP-4i: AHR, 0.47; 95% CI, 0.41-0.52; P < .001), and severe hypoglycemia (eg, vs DPP-4i: AHR, 0.44; 95% CI, 0.38-0.51; P < .001) (eTable 6 in Supplement 1).”
“Another meta-analysis reported that ertugliflozin and empagliflozin could reduce the risk of retinal disease, whereas canagliflozin could increase the risk of vitreous disease.”
I dug a bit more, eTable 5 in Supplement 1 (“Supplemental content” tab) shows that empagliflozin and dapagliflozin are way more protective than canagliflozin to lower the risk of sight-threatening retinopathy. Empa and data are almost identical (except when compared to Pioglitazone, where empa is way better than dapa). However, empa has tiny numbers of users, although the results are still statistically significant, so I would not be surprised if, with larger numbers, empa was shown to be more protective than dapa.
Effect on fasting plasma glucose (FPG) reached after about 1 week
Effect on Hb A1c reached after about 2 months
Effect on weight loss reached after about 3 months
For FPG, Hb A1c and weight loss, dapagliflozin 10 mg was more effective than dapagliflozin 5 mg.
Over 24 weeks, the % of adverse events was lower in dapagliflozin vs placebo, while the % of serious AEs occurred in 1.5% (placebo), 3.9% (dapagliflozin 5 mg), and 3.0% of patients (dapagliflozin 10 mg). However, there were more genital infections and UTIs in dapagliflozin 10 mg compared to dapagliflozin 5 mg. So dapagliflozin 10 mg is overall more effective with fewer adverse events and serious adverse events than dapagliflozin 5 mg except for genital and urinary tract infections.
An Accidental Breakthrough: A Drug Designed to Treat Diabetes Appears to Slow Aging and Forestall Death
By mimicking the effects of fasting, SGLT inhibitors seem to broadly counteract age-related diseases and decline.
Dr. James O’Keefe is no pill-pusher.
As director of preventive cardiology at Saint Luke’s Mid America Heart Institute, O’Keefe has spent much of his career studying how a proper diet, exercise, and other tried-and-true health behaviors protect against the perils of aging.
During our past conversations, O’Keefe, who is also a professor of medicine at the University of Missouri-Kansas City, has bemoaned the sorry state of American healthcare, which he says is structured to treat illness rather than prevent people from getting ill in the first place. “The sicker the population, the better that is for hospitals, drugmakers — the whole system,” he says.
‘I’ve been a physician for 40 years, and I’ve never been so excited about a medication for human health and longevity.’
O’Keefe is an unlikely evangelist for a novel pill-based solution to the problem of age-related disease and infirmity. But he says that his personal experience treating patients with SGLT inhibitors — coupled with his own just-published research into the effects of these medications — has convinced him that they “are truly revolutionary.”
“If you look at how the survival curves separate for people on these drugs versus people on placebo — I have never seen anything like this in my career. Not even close,” he said of the once-daily pill’s apparent ability to extend life and prevent a range of age-related diseases.
“I have no doubt this therapy is going to change the landscape of aging and age-related disease,” he added.