Of course, if you are relatively young (compared to me at 85) and healthy, why would you feel any positive effects if nothing is broken? Why would you expect to see any significant change in your blood work?
One would expect the effects of rapamycin to show up in later years in the form of greater healthspan. We do not know if rapamycin affects human lifespan. But the increased healthspan would result in a lower death rate for the individuals taking rapamycin, producing an apparent median life extension.
I have been taking rapamycin for almost five years, and I feel much better since taking rapamycin. My blood work is excellent, especially for someone my age. The only negative impact on my blood work occurred when I first started taking rapamycin at large doses. It raised my fasting glucose and lipid levels slightly. I addressed this by taking medications to lower them.
The thing that surprises me the most is how virtually pain-free I am. Even my lower back pains have all but disappeared. In the last five years, as I previously posted, I have had no illnesses. No colds, flu, etc. So I believe this cannot be a placebo effect, and the immunosuppressive effect of weekly pulse dosing is nearly non-existent. You think someone getting a pimple on his nose after taking rapamycin is proof. No more evidence than my N=1 of never having gotten a pimple or mouth sore. It could just as likely be a coincidence or placebo effect because he has been reading other people’s reactions to rapamycin. As many as 30-40% of people will experience a placebo effect good or bad.
It is still way too early in the game for people to stop taking rapamycin because they feel no subjective or measurable effect.
I’ve been following this group for 2 years now. I’m still in the planning phase of my potential rapamycin journey.
I’m almost 64. My current conclusion is that starting around 65 years of age and using it for just a few years and then stop might be the optimal tradeoff between benefits, costs and caution, especially until we have human data and especially for otherwise healthy and fit people.
I think this strategy seems to work in mice. Start late in life and take it for a relative “short” period to get most of the longevity benefits
Some here seem surprised that Verdin, a leading longevity researcher, stopped taking rapamycin, but maybe he’s following a similar plan?
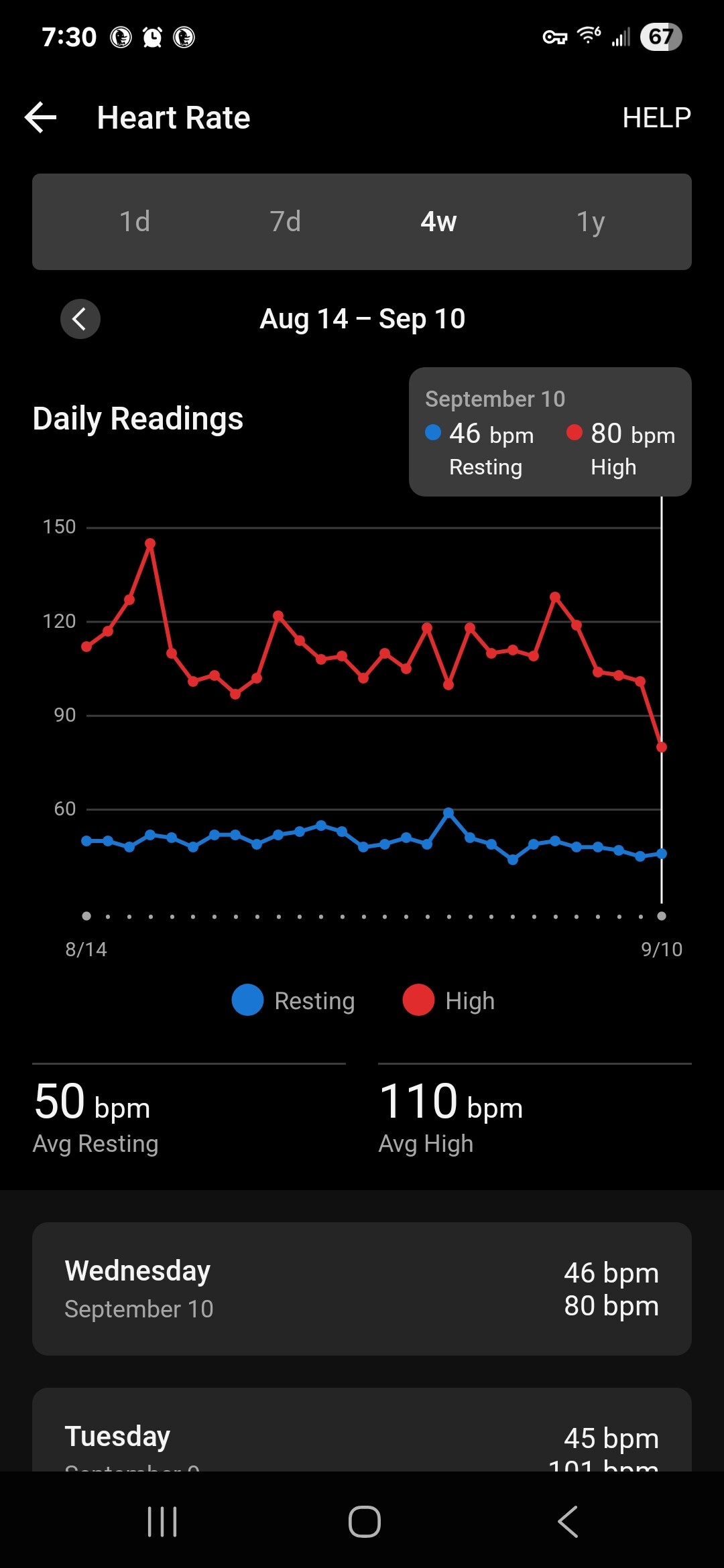
When I was up there for the Longevity Summit conference I met a lot of the Buck researchers and many of the younger people were already taking rapamycin. Like anywhere you get a varying view on risk/reward.
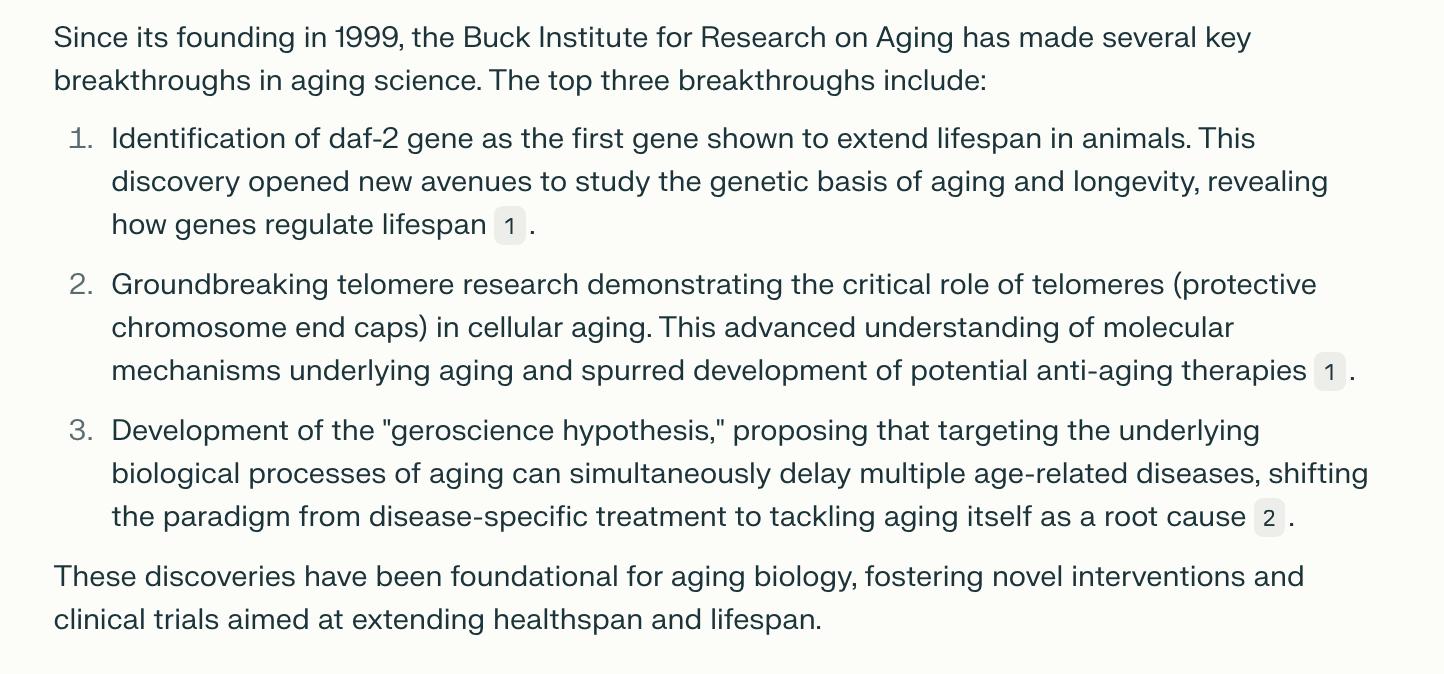
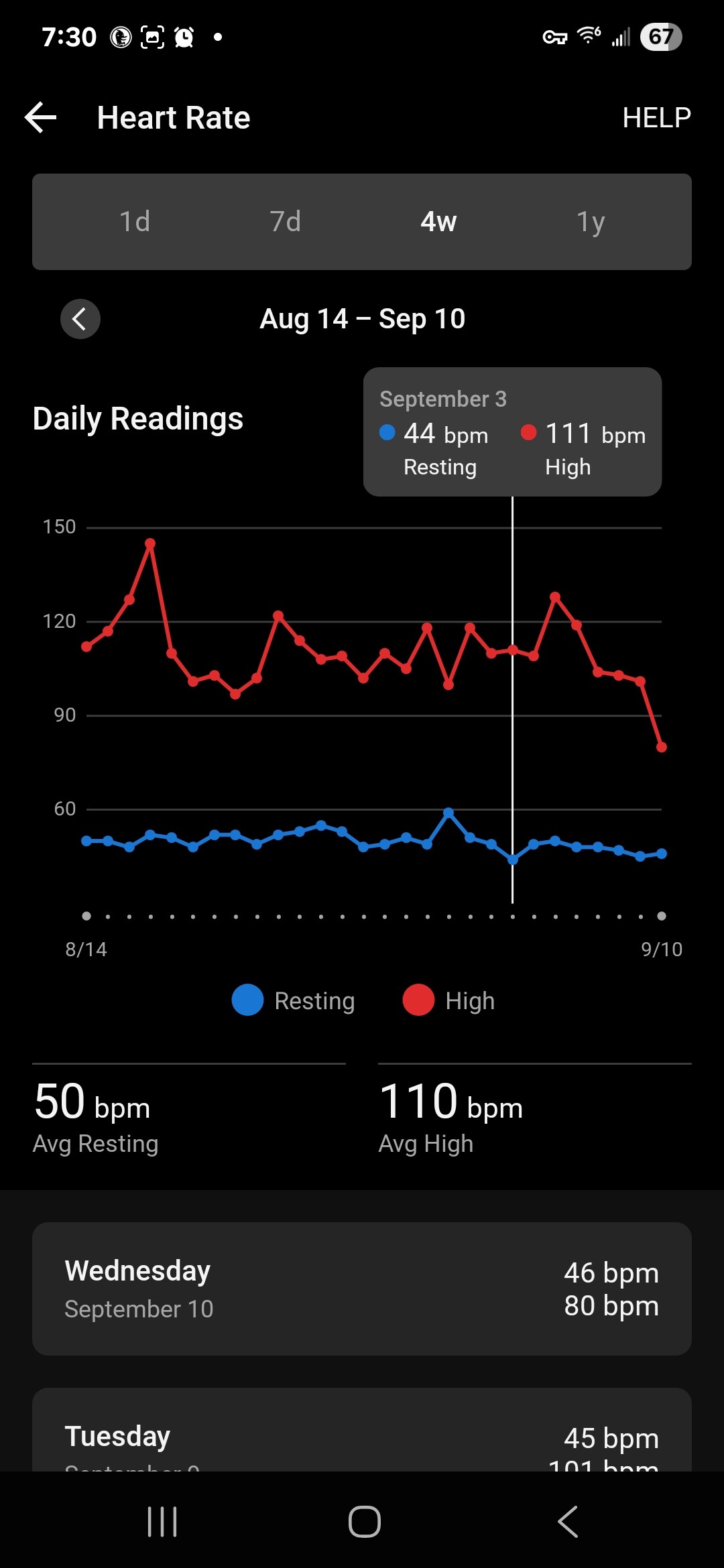
One of the reasons BJ stopped Rapa was that he was alarmed that his RHR was up. While we know of little howbhe arrived at that conclusion.
I couple my weekly Rapa dosing with 24-36 hr caloric fast, I never had RHR as low as this now
RHR depends on lots of things and is not purely a sign of aging. I accept that having a low RHR is generally a good thing. However, if I have been binge drinking for 4-5 days and my RHR has crept up (on fitbit) to say 60 I know that is purely linked to the drinking and when I go on the wagon it will drop down again.
Of course, RHR depends on many factors such as sleep, stress, alcohol(which affect RHR primarily through its effects on sleep), timing and type of meal, meditative practices, medications ( beta blockers, vasodilators). When l consume alcohol, mine usually is 52-53.
I dont think that BJ deviated much from his Blueprint Protocol. I recall when he announced that he was discontinuing Rapa, he cited rising RHR as the reason. Although he didnt put forth sny plausible link between Rapa and RHR.
So, I had been closely tracking mine to see my RHR is trending up.So, far no indication.
I think Eric Verdin’s reasoning is ok, and he explained pretty clearly IMO. He did make the point that the translation of animal studies into humans is pretty poor, which we can hopefully all agree on.
One of the most interesting things he mentioned is the link between body size and longevity. Usually smaller animals have faster life cycles, reproduce quickly etc. Interestingly, humans are a big outlier and we live much longer than we “should” (even biologically/naturally, without medical intervention). He kinda indicated that maybe mice are in a hyper-mTOR activation state, which is normalised by Rapamycin, whereas humans may not be in that state.
So his point is that what applies to mice (inhibiting mTOR, extending life) may not translate to us.
He also laid massive praise onto GLP-1RAs, and said that they are geroprotective.
What we need to do is a Rapamycin trial with naked mole rats. That would put the question to bed. Although it might take 40 years to do the study…
I think the marmoset results are better than the mouse ones as they are long-lived (10+ years).
You also have to remember that there have been 164 studies on Rapamycin across all the model organisms, and they all produced longevity gains. It’s hard to believe that humans would be the outlier. However, it hasn’t been tested in a truly long-lived cohort outside of marmosets, and I doubt it ever will be due to the amount of time and resources it takes.
The question is, is the data good enough to take Rapamycin?
IMHO, yes, it is. I see two probable scenarios.
Human longevity is extended the same as all the other model organisms, leading to an 8-25% (25% hopefully ) life expectancy gain.
Human longevity is not extended, and there is no lifespan gain.
I doubt there would be any detriment, and 1. seems highly probable as we know that CR works via a similar mechanism to Rapamycin and does produce human longevity gains.
So, it’s kind of a no-brainer to take Rapamycin, epigenetic age be damned.
I make no secret that I’m not a Bryan Johnson fan. However in this case I must stand in his defense. Rapamycin works - but even in rapa trials, not all individuals benefit. CR, perhaps the best studied and validated LE intervention, is well known for having a percent of the cohort actually shorten their lifespan. Somebody has to be in that statistical minority where a given drug/intervention doesn’t work or is actually deleterious. Bryan Johnson might unluckily be one for whom rapamycin is a net negative.
I have not delved into the exact reasons why he quit rapamycin, but if his data and/or MD team think quitting rapamycin is the right move for him, I can only applaud his decision. I might have a quibble if based on his n=1 experience he makes a global claim that rapamycin is a negative for all humans looking for LE, but I don’t know the exact nature of his claims.
Bottom line, however, is that rapamycin is not for everyone, and given my general opinion of his approach to LE, I’m actually relieved that he’s hopped off the rapa train so publicly - if one day his whole experiment comes crashing down at least he won’t drag rapa down with him. So I say, bravo Mr. Johnson, you are no longer taking rapamycin! Vaya con Dios, and please don’t come back!
Well, I think he referred to the same (unpublished, right?) data that we’ve heard about.
Lol, he put out a Youtube video where the thumbnail said Rapamycin was poison… so yeah
But I do agree with your point, and I would assume somebody like BJ who is on CR, eats within a small window, probably has very low mTOR activity anyway.
Whos the Number One here? What is ART therapy? Arthritis therapy? What is it and may it be beneficial for a person without arthritis?
Or its art-therapy like painting with fingers?
When I communicated with him in September he said the following:
We are almost complete with lifespan, but the pathology data is taking a bit longer to get generated.
Hard to say on when lifespan will be published, depends a bit on generating those data