It’s low blood pressure. That’s my doctor’s opinion.
Maybe the stock market stress played into it as well. Maybe some dehydration as well.
Thank you for all your well wishes and I have to be even more careful of maintaining my sugar levels.
It’s low blood pressure. That’s my doctor’s opinion.
Maybe the stock market stress played into it as well. Maybe some dehydration as well.
Thank you for all your well wishes and I have to be even more careful of maintaining my sugar levels.
So sorry to read that. Hopefully the doctor will be able to confirm the source of the problem. Hypoglycemia is a good guess. Citrulline has a short half-life (2-3 hours) so it’s more likely to lead to blood pressure variability than telmisartan (24h half life). Even more so if the dosing is not exactly identical every day and/or if it’s a supplement (there are often big differences between the stated dose and the actual dose).
You mean from making a fortune? Big movements in the broad market means a huge earning opportunity, especially on the options side. Congratulations, you must be really raking it in. And it was such an easy call, too! DJT announced exactly what he was going to do and when, and everyone knew what the market reaction would be! The easiest call in the last 50 years. All you had to do is go all in. Which of course you did. Congratulation! Although I know it must have been stressful to see such huge amounts of $ flowing into your accounts! I read about the guy who fainted when he realized his lottery ticket was a winning one. It can be stressful🤣!
No. I wish. I was playing defensive. I didn’t want to short the market as Mr. Trump has usually backtracked quickly on his tarrifs and I didn’t want to get whipsawed. I’m coming out of this whole fiasco with a small 1.7% loss YTD. Prior to the tarrifs announcement it was a positive 4.1%.
Yes, I should have just gone with options strangles that would have made me lots of money if the markets moved greatly in either direction. By the time the realized ‘Oh shit!’ moment occurred, volatility was sky high and strangles were no longer cheap.
You don’t need to hit a home run every time. Not losing your shirt in this market can be good enough. Now’s the time to figure out where the bottom is going to come in at.
My sources say a minimum of 8% more should be expected with the possibility to be much worse if Trump stays in denial.
I hope you did well. It seems you recognized the winning strategy ahead of time!
Well, I can’t take much credit for what was obvious to many. But here’s the wrinkle. I actually believe you did what a ton of people did - market behaviour was saying “we don’t believe DJT is serious”. Because if the market believed that he was serious, we should have been seeing steady market declines for awhile now. The fact that the market plunged after that announcement tells us that it came as a shock/surprise to most sellers… so you can’t beat yourself up too much, because you thought what the general market thought😎.
And I go by the advice “when people tell you who they are, believe them”. DJT has been obsessed with tariffs for decades. I fully believed he’d go nuclear - the guy has a history of recklessness.
But hey, win some, lose some. As long as you live to play another day.
The market is looking for a bottom, sure. Unless there’s some exceptions that will be carved out, look at where for example Apple is headed. Lost almost 10% in one day. Now imagine costs go up like crazy, earnings tank. What happens when institutional investors like big pension funds start dumping positions. Another 8% might be optimistic. The way it’s worked since the last 30+ years, is buying dips, so the bottom was reached pretty fast. But if the whole economy tanks, it may not work like that anymore - people have forgotten what a bear looks like, lol.
OK, enough of this, it’s really off topic. I’m done.
That is fascinating - thank you for posting this, and as usual, with a fair bit of reference materials.
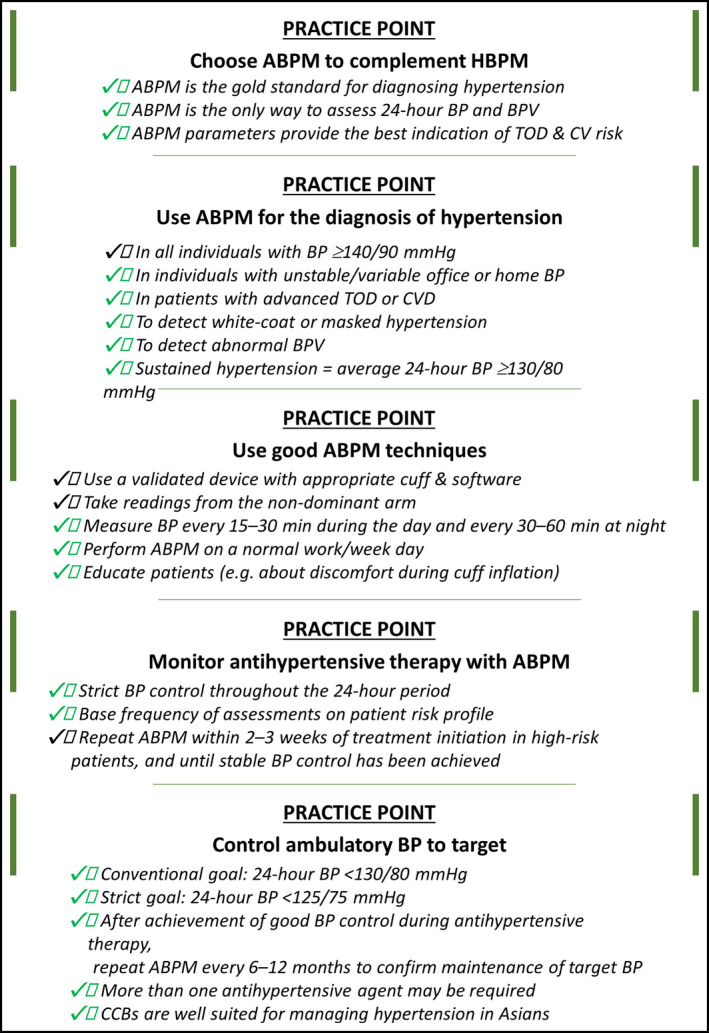
The “gold standard” of looking at BP is a 24 hour ambulatory measurement. Almost never done in practice. I’d suggest that doing this repetitively over time is of value. I have one of these devices, and not free - but <$200 to own one.
Sorry to hear of all this happening. I’d get a 24 hr ambulatory blood pressure monitor.
Hypoglycemia - unless very severe doesn’t cause loss of consciousness, and certainly not suddenly.
As much as BP in someone who usually is looking at average SBP of 125 mmHg might feel a little off with a SBP in the 90’s it won’t cause loss of consciousness.
Syncope (loss of consciousness) is pretty much always loss of cardiac output sufficient to keep the brain functioning. So EKG, CBC, BMP is reasonable. Brain scans not - as there is nothing you can see on a brain scan that would cause syncope. It sounds like there was nausea - which is possibly the bigger clue - most likely this was a vaso-vagal syncope due to the nausea.
Sure, need to get it checked out - but not over investigated. The ER workup for syncope, unless there are other factors where we think it was syncope (e.g. seizure) should be a limited workup, in general, unless there are other features involved that might indicate an ongoing risk (e.g. palpitations, chest pain, fever, breathlessness).
Obviously, you are seeing a physician who will look into this, but in general if a basic workup is normal, I’d generally not be too excited.
Thank you @DrFraser Your comments, as always, are invaluable.
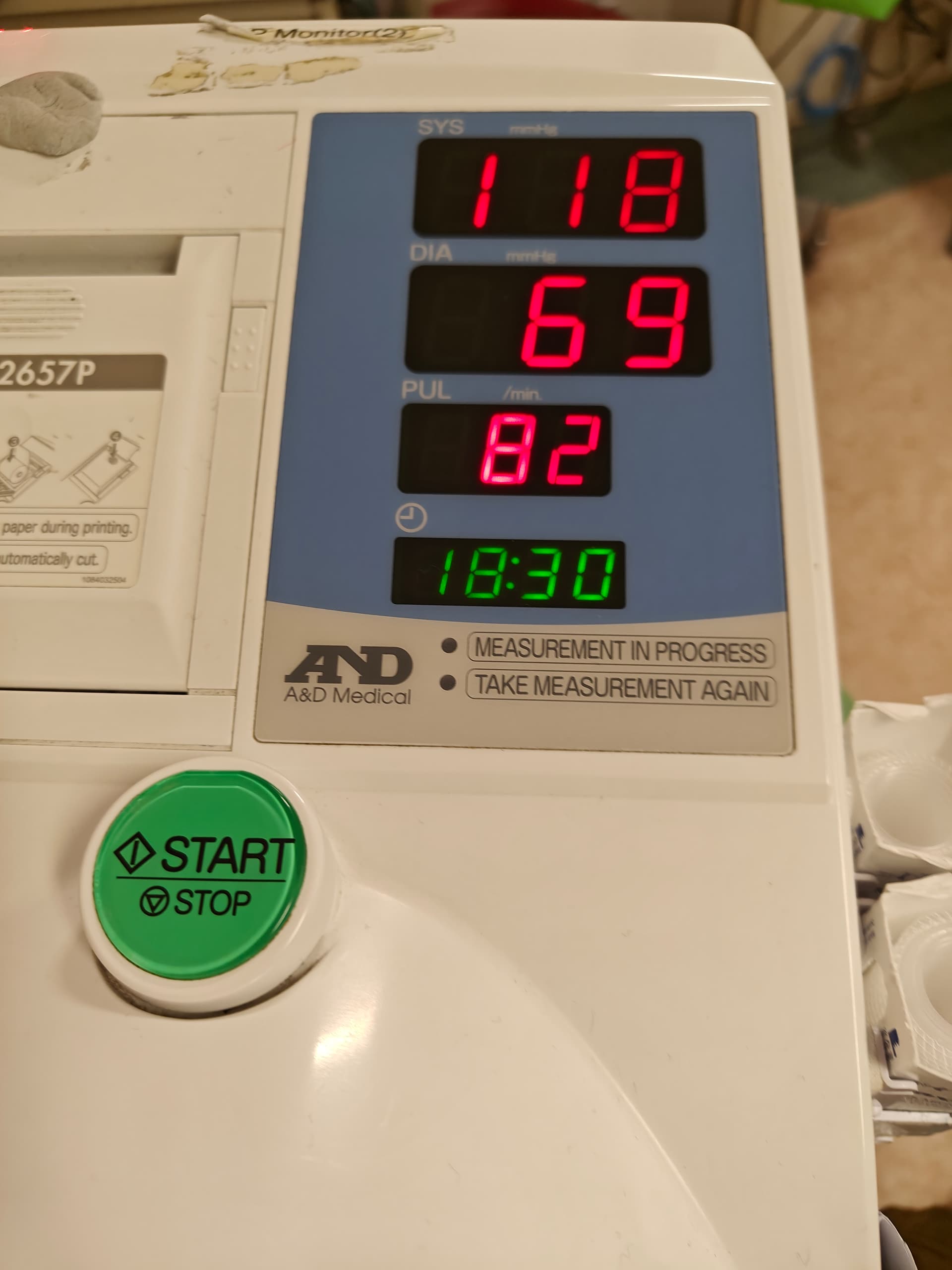
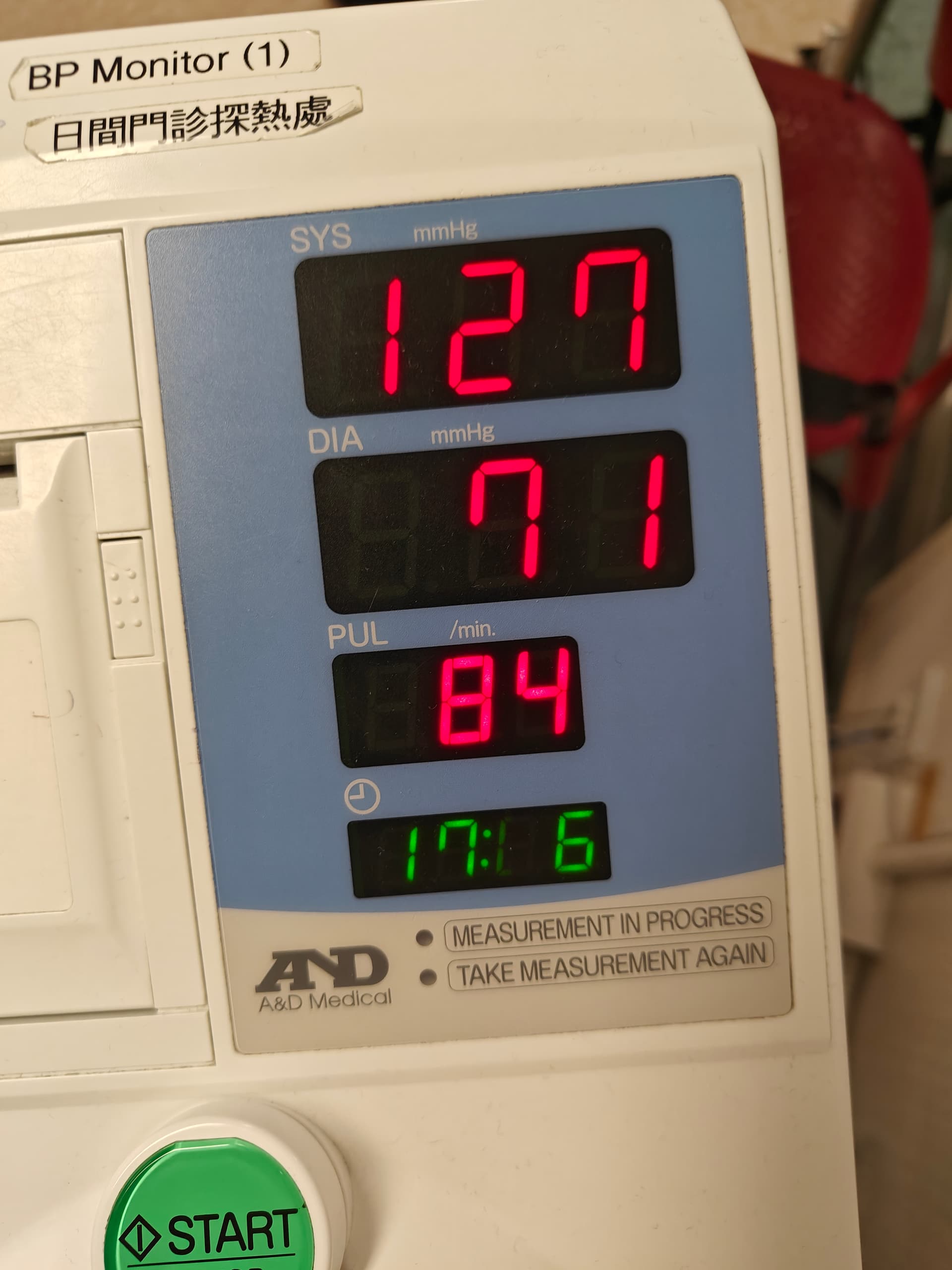
So should I stop taking Telmisartan? I posted what my BP readings were above. I’ve also had 2 more in the 115 range while at the hospital.
They did a brain CT scan for me to see if there was hemorrhaging or a tumor. Here’s hoping I have a clean bill of health!
115 mmHg in normal individuals won’t cause symptoms. Now if you usually run a SBP of 220 mmHg and we suddenly put you down to 115 mmHg - that can cause problems. In general for individuals who are running BP in the 120’s - it’s going to take SBP<<70mmHg to see a loss of consciousness.
When I see someone who has low blood pressure in the ER - passing out is just not a thing unless the BP is profoundly low. We also like to get standing BP/HR just to make sure it isn’t low with that (e.g. postural hypotension).
The doctor and I now believe it is low blood pressure. Probably caused by the Telmisartan 40 mg.
Now the question is whether to dial it down to 20 mg or stop it altogether. What do you think, @DrFraser
What verified measurements have been recorded showing BP low enough to cause or risk loss of consciousness?
My home BP monitor read 96 SBP 4 hours after the incident. That would be an all time low. However, I am not sure how trustworthy that monitor is. The readings at the hospital were all around 115. Those were 12 hours after the incident.
I guess what I should do is take my Telmisartan and then measure BP in the middle of the night to verify. Thanks for the great idea.
You may want to collect data properly and grab something like a Contec ABPM50 and wear it without any meds, then consider slowly adding the medication back (with your doctor’s agreement) and track the data.
A blood pressure of 96 mmHg systolic doesn’t cause loss of consciousness … not in your situation. Now it if was 50 or 60 systolic maybe. Additionally you’d need to know your BP with standing - as I presume you were standing - and the 24 hr monitoring will give solid data to act on with your doctor’s advice.
Wouldn’t an Aktiia monitor be good in your case as well?
Since you’ve already blacked out once maybe it’s important to be careful and not lower it too much, or it might be something else as well.
I just got my Contec BP monitor. It’s saying my SBP is around 116-123/76 while I’ve been using Telmisartan 20 mg daily. That doesn’t sound too bad to me. Surely nothing that would cause me to blackout. It must have been tied to the nausea.
Nausea commonly causes a vasovagal reaction, which can drop blood pressure and heart rate.
I obviously didn’t assess you - but we see this frequently in the ER - actually treated one of these yesterday.
The good thing is you can also look at your BP variability and whether it has a normal pattern overnight, etc. I think doing a 24 hour ambulatory if on BP meds (or not) is sensible quarterly.
BP is usually higher during the day (or periods of wakefulness) and lower at night (or periods of sleep). The expected physiological fall in nighttime BP is > 10% (dipping), whereas a reduction of < 10% in BP at night is defined as non‐dipping; patients with a riser (or reverse dipping) pattern show an increase in BP during sleeping hours to levels (BP fall is < 0%) that may be higher than those during the day (ie, nocturnal hypertension). 34 Extreme dipping refers to patients who show a marked (>20%) nocturnal fall in systolic BP (SBP) and or diastolic BP (DBP), or have a night/day SBP or DBP ratio of < 0.8. 20 Given that the circadian rhythm of BP is predominantly determined not by awake‐sleep behavior rather than the day‐night cycle, 35 the nocturnal dipping status of shift workers should be determined by awake BP (during nighttime) and sleep BP (during daytime).
Nocturnal BP may be the most reproducible and reliable ABPM parameter for risk stratification. 36 Nocturnal hypertension (BP ≥ 120/70 mmHg) could indicate the presence of comorbidities such as obstructive sleep apnea (OSA), and the riser pattern of nighttime BP is associated with a particularly poor prognosis with respect to the occurrence of stroke and cardiac events. 37 , 38 , 39 Stroke risk also appears to be increased in elderly hypertensive patients with an extreme dipper pattern. 40 Another important BPV parameter is the morning BP surge (the difference between the lowest nighttime BP and morning BP measured 2 hours after awakening). Early morning BP surge is associated with an increased risk of cardiovascular and cerebrovascular adverse events, especially hemorrhagic stroke. 41 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 , 50 , 51 , 52
Excessive BPV could result in large dynamic surges that have the potential to trigger adverse cardiovascular events (the resonance hypothesis), and the risk of these events is exaggerated in high‐risk patients with vascular disease. 53 Greater variability in SBP is a significant independent predictor of mortality. 54 , 55
Aktiia (Hilo) isn’t useful for this right now because it’s inaccurate at night.
Related: