It Crushes Visceral Fat, But the Scale Barely Moves!
I. Executive Summary
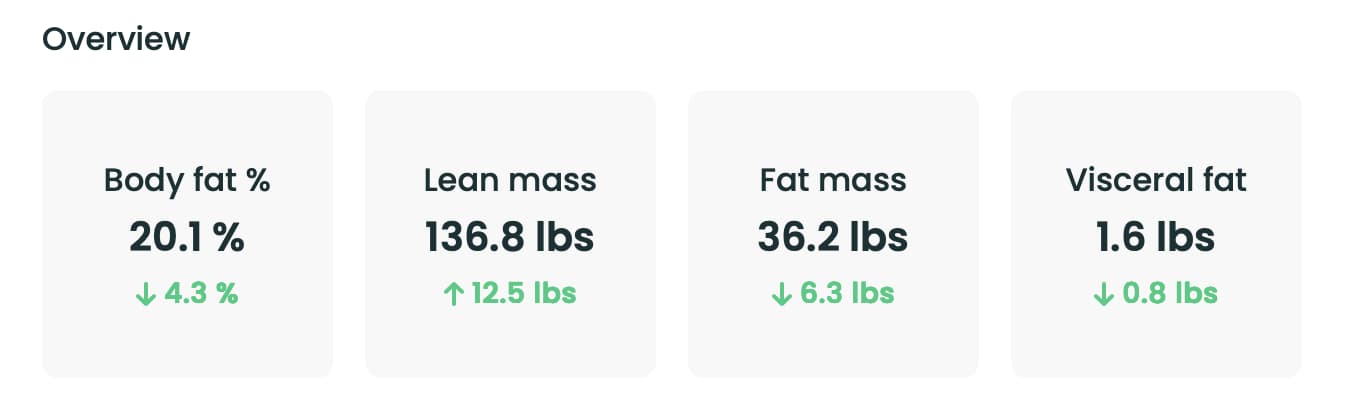
This video analysis by Physionic audits the clinical literature surrounding Tesamorelin (formerly designated TH9507), a 44-amino-acid peptide analogue of endogenous Growth Hormone-Releasing Hormone (GHRH). The central thesis is that Tesamorelin exerts a highly selective, targeted lipolytic effect on visceral adipose tissue (VAT) while leaving standard subcutaneous fat depots largely unaltered and whole-body mass on the scale stable. This weight-neutral body recomposition is mediated by a concurrent increase in total lean mass.
The historical data for Tesamorelin is rooted in HIV-associated lipodystrophy—a condition where early antiretroviral therapies induced severe, unwanted fat redistribution, characteristically presenting as pathological visceral fat accumulation. Visceral fat cells are highly sensitive to growth hormone metrics. Under normal conditions, hypothalamic GHRH binds to pituitary receptors, stimulating pulsatile Growth Hormone (GH) release. GH subsequently drives peripheral lipolysis by signaling fat cells to liberate stored fatty acids for metabolic clearance. In subclinical populations, or those undergoing specific pharmacological strains, this neuroendocrine cascade is impeded.
Tesamorelin acts as a synthetic GHRH mimetic, binding directly to pituitary somatotrophs to rescue and augment pulsatile GH secretion. Downstream, elevated GH prompts the liver to synthesize and release Insulin-like Growth Factor 1 (IGF-1), doubling or tripling baseline values. This rise in IGF-1 stimulates systemic cell growth and increases total lean mass. Appendicular lean mass measurements (excluding the trunk) indicate potential peripheral tissue accrual, though the exact ratio of muscle, bone, or water within this lean mass expansion remains unquantified due to gaps in the current literature.
While the majority of the 11 trials evaluated feature HIV cohorts, recent clinical data confirms these visceral-targeted lipolytic effects extend to non-HIV populations, including “TOFI” (thin outside, fat inside) phenotypes who carry dangerous abdominal fat despite a normal Body Mass Index (BMI).
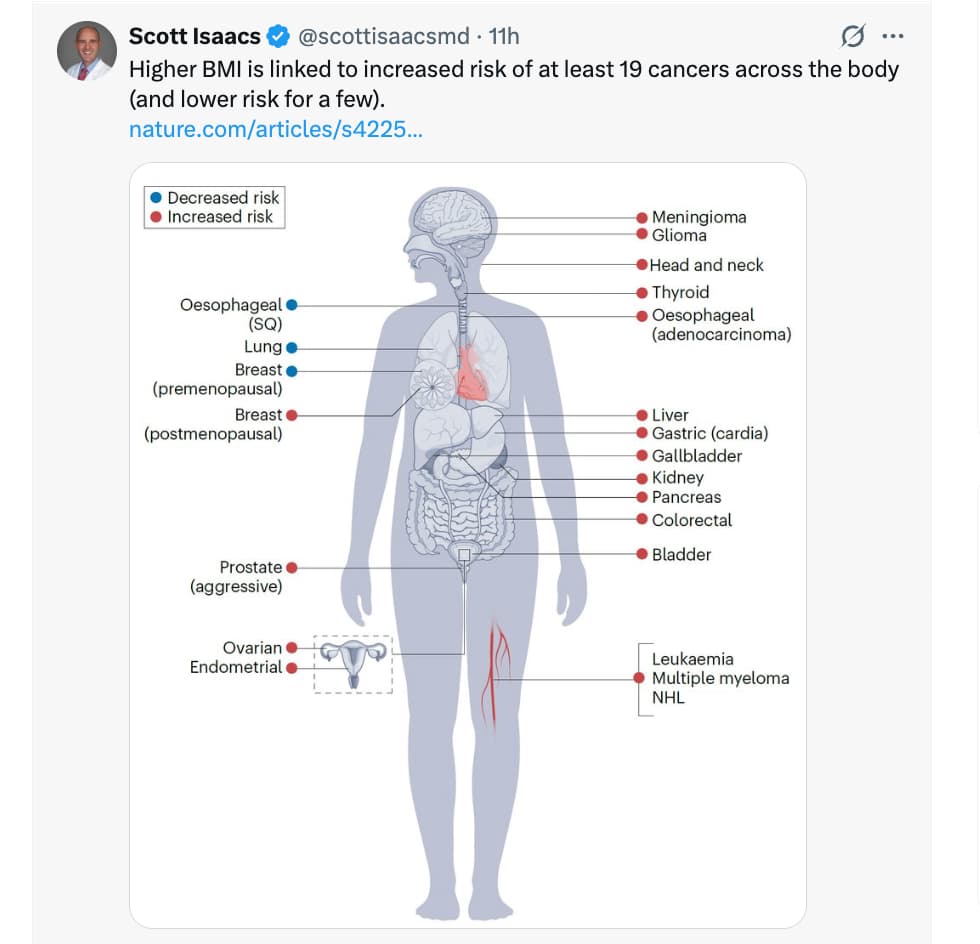
Safety data over a one-year tracking window demonstrates that Tesamorelin is generally well-tolerated, presenting minor side effects like localized injection-site erythema and transient musculoskeletal aches. However, the peptide induces mild, concurrent elevations in fasting blood glucose, and long-term human safety trials evaluating oncogenic risks remain absent. Although sustained elevations in IGF-1 warrant careful monitoring, current data shows that individual values stay within normal upper physiological ranges, suggesting that for select populations presenting with low growth hormone status or isolated visceral adiposity, the net health benefits of targeted VAT depletion outweigh the potential metabolic risks.
II. Insight Bullets
-
The Targeted Lipolysis Recomposition: Tesamorelin systematically depletes visceral adipose tissue without altering subcutaneous fat reserves or shifting total body weight on the scale, resulting in a targeted, weight-neutral body recomposition [[03:14], [03:24]].
-
Rescuing the Pituitary Cascade: As a synthetic GHRH analogue, Tesamorelin binds to pituitary receptors to rescue impaired neuroendocrine pathways, triggering a cascade of pulsatile endogenous growth hormone release [[04:14], [04:42]].
-
Growth Hormone-Mediated Lipolysis: Elevated GH actively signals visceral adipocytes to break down stored lipids, liberating fatty acids into systemic circulation to clear dangerous abdominal fat accumulations [[04:25], [04:34]].
-
The GHRH-Liver-IGF-1 Loop: Pituitary stimulation by the peptide prompts the liver to double or triple baseline production of Insulin-like Growth Factor 1 (IGF-1), a powerful molecule that stimulates cellular growth and protein synthesis [[05:11], [05:19]].
-
Lean Mass Expansion Context: The preservation of body weight during extensive visceral fat loss is mediated by a concurrent increase in lean mass, though the exact ratio of skeletal muscle to bone or water remains uncharacterized [[03:34], [05:01]].
-
The Appendicular Lean Mass Proxy: Volumetric measurements excluding the trunk (appendicular lean mass) demonstrate clear peripheral tissue growth, suggesting potential positive gains in skeletal muscle structure [[05:35], [05:44]].
-
The HIV Lipodystrophy Origin: Tesamorelin was originally developed to treat HIV-associated lipodystrophy, an endocrine complication where early antiretroviral drugs caused severe fat redistribution and lipolytic failure [[03:50], [03:57]].
-
The TOFI Phenotype Utility: Tesamorelin’s selective action makes it a highly effective tool for “TOFI” (thin outside, fat inside) phenotypes who present with low growth hormone status and high visceral adiposity despite maintaining a normal body weight [[09:32], [09:45]].
-
Baseline-Dependent Efficacy: Randomized, placebo-controlled data demonstrates a direct, linear relationship between a patient’s baseline visceral adiposity and their treatment outcomes; individuals carrying the highest initial visceral fat burden experience the greatest relative benefit from the peptide [[02:26], [02:41]].
-
Non-HIV Cohort Translation: Although the bulk of historical data focuses on HIV populations, recent clinical trials confirm that Tesamorelin’s selective visceral fat depletion translates successfully to non-HIV cohorts [[07:04], [07:19]].
-
Mild Glycemic Disruption: Tesamorelin use causes a small but consistent increase in fasting blood glucose levels, requiring routine metabolic monitoring during active treatment cycles [[08:31], [08:39]].
-
Transient Adverse Events: Documented short-term side effects are mild and include localized injection-site swelling, erythema, and transient musculoskeletal aches [[08:24], [08:31]].
-
The Long-Term Oncogenic Gap: Human clinical safety data for Tesamorelin is currently capped at a one-year testing window; consequently, the long-term safety profile and potential oncogenic risks associated with sustained IGF-1 elevation remain uncharacterized [[08:42], [08:47]].
-
Physiological Safety Boundaries: While Tesamorelin dramatically upregulates IGF-1 production, individual biomarker values generally remain within normal upper physiological ranges, reducing the immediate risks of pathological acromegaly [[08:56], [09:02]].
-
Targeted Patient Demographics: Due to its selective, weight-neutral mechanisms, Tesamorelin serves as a highly specialized prescription peptide for two distinct groups: individuals with verified growth hormone deficiency, and normal-weight patients seeking to clear dangerous visceral fat [[09:17], [09:32]].
IV. Actionable Protocol
High Confidence Tier (Backed by Level A/B Human Evidence)
-
Utilize Tesamorelin for Isolated Visceral Depletion: For individuals presenting with high visceral adiposity but a normal BMI (the TOFI phenotype), consider Tesamorelin as a targeted option to clear internal abdominal fat without causing further subcutaneous fat loss or muscle wasting [[03:24], [09:45]].
-
Establish Verified Growth Hormone Deficiencies Prior to Treatment: Do not self-prescribe Tesamorelin for general weight loss. Ensure a qualified physician runs a dynamic growth hormone stimulation panel to verify an actual neuroendocrine or pituitary deficiency before initiating therapy [[07:28], [09:17]].
-
Monitor Glycemic Stability Routinely: Because GHRH analogues induce a mild increase in fasting blood glucose, establish a baseline metabolic panel and regularly track your HbA1c and fasting glucose levels throughout active treatment cycles [[08:31]].
Experimental Tier (Translational Peptide Guidelines with High Safety Margins)
-
Track the IGF-1 Velocity Envelope: Monitor your systemic IGF-1 values every 8 to 12 weeks during treatment. Ensure that while the liver accelerates IGF-1 production to expand lean mass, individual values remain safely within normal upper physiological limits to mitigate off-target proliferative risks [[05:19], [08:56]].
-
Manage Injection Purity and Sterility: Because Tesamorelin is delivered via subcutaneous injection, follow strict aseptic techniques. Rotate your injection sites regularly and monitor local tissues for mild erythema or transient swelling [[08:24]].
Red Flag Zone (Claims Contradicted by Data or Lacking Safety Evidence)
-
Do Not Rely on Tesamorelin for Total Weight Loss: Avoid using Tesamorelin expecting significant drops on a standard bathroom scale. The peptide drives a weight-neutral body composition shift, replacing visceral fat mass with expanded lean mass [[03:14], [03:34]].
-
Avoid Unmonitored Use Beyond One Year: Do not extend Tesamorelin cycles past a 12-month window without direct oncological and metabolic oversight. Long-term human trials evaluating the potential cancer risks of sustained IGF-1 up-regulation are currently absent [[08:42], [08:56]].
-
Never Purchase Research-Grade Peptides Online: Absolutely refuse to buy non-regulated, “research-use-only” Tesamorelin from online chemical suppliers. Bypassing human-grade compounding pharmacy standards introduces severe risks of pathogenic contamination and heavy metal impurities [[24:04]].*
V. Literature Verification & Methodological Context
The endocrinological mechanisms, tissue-specific lipolytic responses, and safety tracking profiles associated with Tesamorelin are heavily validated across peer-reviewed metabolism and regulatory literature.
-
Visceral Adiposity Depletion in HIV and Non-HIV Cohorts: The clinical efficacy of Tesamorelin in targeting visceral fat is rooted in large-scale multi-center randomized controlled trials. Landmark studies published in The New England Journal of Medicine and JAMA confirm that 2 mg daily subcutaneous doses of Tesamorelin significantly reduce visceral adipose tissue (measured by CT scans) by an average of 15% to 18%, while preserving subcutaneous fat depots across both HIV lipodystrophy patients and non-HIV cohorts presenting with abdominal obesity (Falutz et al., 2007; Stanley et al., 2014).
-
The GHRH-GH-IGF-1 Signaling Axis: The molecular pharmacology of Tesamorelin as a stabilized GHRH analogue is well-documented. By resisting rapid enzymatic degradation by dipeptidyl peptidase-4 (DPP-4), Tesamorelin maintains a significantly longer half-life than native GHRH, allowing it to effectively stimulate pituitary somatotrophs to synthesize and release growth hormone, which subsequent drives hepatic IGF-1 expression (Mangili et al., 2006).
-
Glycemic Dynamics and Long-Term Safety Gaps: The warning regarding mild glycemic disruption is supported by formal FDA advisory briefings. Clinical trial endpoints show that intensive growth hormone upregulation can antagonize peripheral insulin signaling, driving minor elevations in HbA1c and blood glucose. Furthermore, while short-term data confirms values remain within safe physiological limits, the Endocrine Society notes that multi-year long-term safety data evaluating the downstream oncogenic risks of persistent IGF-1 elevations is still required (Spooner & Perry, 2011).
Methodological Caveat: While Tesamorelin is a highly effective, FDA-approved therapeutic for clearing dangerous visceral adipose tissue and improving lipid profiles in verified clinical cohorts, it functions as an artificial neuroendocrine modifier. It cannot replace foundational lifestyle habits, and cessation of the peptide without concurrent caloric and exercise management results in a rapid return of visceral fat to baseline levels.