I’m continuing my deep dives into the genetic pathways to get actionable insights as the previous ones have been incredible precise and useful. This time I’m looking at Alzheimer’s and other dementias genetic pathways.
Here is the general description of the pathways and their variants. I will put the finding about my own genome below it as an example of what useful and actionable insights you can get.
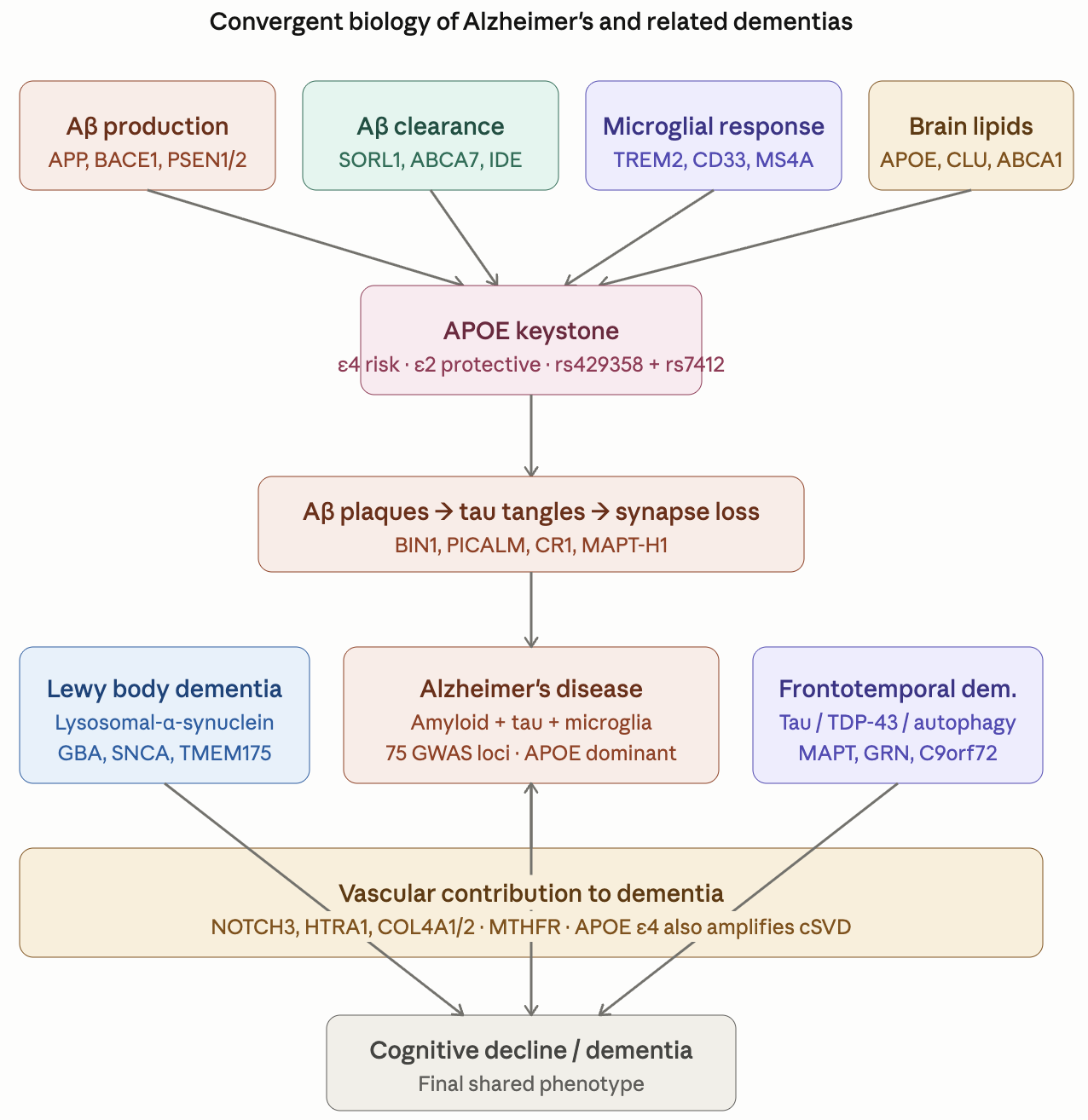
Dementia_Genetic_Pathway_Reference.pdf (540.0 KB)
The pdf report above is valid for everybody but here is the summary of the findings I get when I apply it to my own genome. The full detailed report is 24 pages long.
Dementia Genetics — Top 10 Findings
Report date: April 2026 (updated) • Source: 60× WGS, GRCh38 • Companion: Dementia_Genetic_Report.docx
1. APOE ε3/ε3 confirmed (favorable)
Verified at BAM level (50× and 63× read depth, zero non-reference reads at rs429358 and rs7412). Population-baseline AD risk — no ε4 amplifier and no ε2 protection. This single finding caps the magnitude of everything else in the report.
2. CR1 triple homozygous risk (rs6656401, rs3818361, rs679515 — all 1/1)
Strongest single common-variant signal in this profile. Three independent CR1 fine-mapped tags all homozygous for the risk allele. Per-allele OR ≈ 1.18 → homozygous ≈ 1.35 for AD. Microglial complement-dependent Aβ clearance impaired. The recently added Avmacol ES (sulforaphane) directly supports microglial polarization toward the protective DAM phenotype — this is the most mechanistically aligned regimen item for this finding.
3. ABI3 S209F homozygous (rs616338 1/1) — needs confirmation
Population homozygous frequency ~0.012% — the call is high-confidence (DP 51, MQ 60, GQ 99) but unusual. Worth a confirmatory clinical genotype because if real, OR ≈ 1.43 per allele (Sims 2017 Nat Genet). Microglial cytoskeletal regulator.
4. ABCA7 rs4147929 homozygous risk + double CLU het + ABCA1 R219K het
Brain lipid-handling axis: moderate residual signal even with ε3/ε3. Reinforces case for DHA-specific intake — Boston Heart Fatty Acid Balance shows DHA is currently borderline LOW (84.3 µg/mL) despite the substantial omega-3 stack.
5. TREM2 wild-type, GBA wild-type, MAPT wild-type, NOTCH3 wild-type, no autosomal-dominant AD/FTD
The high-impact rare-variant tier is clean across all four dementias. Combined with ε3/ε3, this is the strongest reassurance the data provides.
6. C9orf72 hexanucleotide expansion NOT assessable from short-read WGS
Default no testing, but if any 1st-degree relative has FTD, ALS, or early-onset dementia, request repeat-primed PCR — this is the one test the WGS cannot substitute for.
7. TMEM106B heterozygous (rs1990622 0/1)
Modifies LATE neuropathology (limbic-predominant age-related TDP-43 encephalopathy) — a TDP-43 proteinopathy that mimics AD clinically and affects ~25% of brains over 85. No specific treatment exists; modifiable factors are the actionable lever.
8. IDE rs1887922 homozygous + metabolic-AD axis
Insulin-degrading enzyme also degrades Aβ. The current tirzepatide + empagliflozin + imeglimin regimen indirectly supports this axis by improving insulin sensitivity. No regimen change needed — the alignment is already strong.
9. Modifiable factors > genetics in this profile
Without ε4, the cumulative dementia genetic risk is approximately 1.2–1.4× population baseline. The biggest leverage now lives in:
- Hearing assessment (largest single modifiable factor — Lancet 2024)
- BP < 130 mmHg systolic (already targeted by telmisartan)
- LDL aggressive lowering (newly upgraded — Repatha 140 mg q2wk active)
- Glucose control (already optimized)
- Sleep optimization (glymphatic Aβ clearance)
- Sustained aerobic + resistance exercise
- Social engagement
10. Recent regimen updates close most gaps from the prior version
The April regimen changes directly address the dementia-axis gaps the previous version of this report flagged at MODERATE/LOW priority:
- Repatha (replaces bempedoic acid) — aggressive LDL lowering for cerebrovascular small-vessel disease (Williams 2020 JAMA Neurol MR signal)
- Avmacol Extra Strength (new) — sulforaphane source for NRF2 / microglial polarization (closes 5-report convergent gap)
- Momentous Multi to full dose (4 caps) — improved 5-MTHF / methyl-B12 / P5P / B2 coverage for MTHFR + cerebrovascular cross-link
- NACET increased 100 → 200 mg — appropriate dose for the convergent 4-report glutathione bottleneck
- Lithium orotate 5 mg evening (new) — microdose tau-axis insurance via GSK3β inhibition